Mohammed M’hamedi*![]() | Mohammed Merzoug
| Mohammed Merzoug![]() | Mourad Hadjila
| Mourad Hadjila![]() | Mohamed Hichem Hachemi
| Mohamed Hichem Hachemi![]() | Amina Bekkouche
| Amina Bekkouche![]() | Omar Azzoug
| Omar Azzoug![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Cardiovascular disease continues to be the primary global cause of mortality, yet existing remote monitoring solutions remain prohibitively expensive for widespread adoption. Addressing this critical gap, we present an affordable, real-time cardiac monitoring system that integrates biomedical sensing with cloud-based deep learning analytics. Our solution employs an AD8232 ECG module for capturing cardiac electrical activity alongside a SIM808 module for simultaneous GPS tracking, with data processed through a WeMos microcontroller and transmitted to a cloud database. For advanced ECG interpretation, we developed a novel hybrid CNN-TCN deep learning architecture that classifies heartbeats into five diagnostic categories: normal (N), supraventricular ectopic (S), ventricular ectopic (V), fusion (F), and unknown (Q) beats. This integrated hardware-software platform demonstrates three key innovations: (1) cost-effective real-time data acquisition, (2) robust cloud-based storage and accessibility, and (3) state-of-the-art arrhythmia detection through our optimized deep learning model. According to the results, the proposed method outperforms previous methods in cardiac rhythm classification, achieving competitive performance with an overall accuracy of 98.55%, sensitivity of 91.2%, and specificity of 99.4%. The combination of portable hardware with accurate algorithmic classification offers significant value for telemedicine applications and decentralized patient management, particularly in resource-constrained healthcare environments.
cardiac patients, remote monitoring, ECG signal, SIM808 GPS/GPRS/GSM module, AD8232 ECG module, CNN, TCN, decision making
The rapid development of the internet has led to the emergence of the vast network known as the Internet of Things (IoT) [1, 2]. IoT-enabled "smart" assets now seamlessly connect to global networks, autonomously exchanging valuable data without human intervention, as demonstrated in modern traffic management systems [3]. These intelligent systems prove particularly transformative for individuals with limited independence. In healthcare applications, IoT facilitates continuous real-time monitoring through networked sensors that track patient status, including geolocation, vital signs, and other critical health parameters. This technological paradigm shift enables a proliferation of IoT applications that will fundamentally transform nearly all aspects of daily life, accelerating the development of truly intelligent environments.
The rapid proliferation of IoT devices has profoundly impacted numerous sectors, with healthcare representing one of the most significant areas of transformation [4]. Within medical applications, IoT enables the deployment of interconnected electronic devices and specialized medical sensors, with remote patient monitoring emerging as a particularly valuable use case [5, 6]. For the millions worldwide suffering from chronic conditions, IoT-based telemedicine solutions-especially medical telemonitoring systems-offer substantial potential to mitigate health risks through continuous monitoring while keeping clinicians informed of their patients' status in real time.
This paper proposes an IoT-based remote monitoring system dedicated to CPs. The system acquires a patient's ECG signal, calculates the heart rate, and transmits this data to a database in real-time. The system utilizes a WeMos D1 Mini module as a microprocessor for calculations and Wi-Fi connection. Additionally, two other modules are integrated: a heart rate module for ECG signal acquisition and a GSM/GPRS/GPS module for patient geolocation and anomaly alert transmissions via SMS. To assist doctors in making faster decisions, the system implements a hybrid deep learning classifier that merges Convolutional Neural Networks (CNN) with Temporal Convolutional Networks (TCN) trained on the MIT-BIH dataset. This model analyzes the ECG signal and detects various types of cardiac arrhythmias.
The main contribution involves an innovative IoT-based remote monitoring system created especially for cardiac patients (CPs), which incorporates three key components: (1) a WeMos D1 Mini microprocessor module handling computations and Wi-Fi connectivity, (2) an ECG acquisition module for cardiac signal measurement, and (3) a GSM/GPRS/GPS module enabling patient geolocation and SMS-based anomaly alerts. To enhance clinical decision-making, we implement a hybrid (CNN-TCN) deep learning classifier that merges Convolutional Neural Networks (CNN) with Temporal Convolutional Networks (TCN) trained on the MIT-BIH dataset, capable of detecting and classifying various cardiac arrhythmias from the acquired ECG signals. This proposed work is motivated by the need to enhance public health through better diagnostic performance, increased accessibility, lower healthcare costs, and real-time data acquisition with cloud-based analytics.
The remainder of the paper is organized as follows. Section 2 discusses the motivation, associated works, and general information leading to the proposed IoT-based monitoring CPs system. Section 3 describes the IoT system in its global view by showing its components, such as the WeMos D1 Mini board and the two associated modules, the AD8232 and the SIM808. In Section 4, we will present in detail the practical realization of our dedicated IoT project for monitoring CPs. Section 5 covers ECG classification based on the CNN-TCN model. The conclusion is given in Section 6.
In this section, we provide and analyze a range of research studies that are linked to the present contribution. The impetus for this research endeavor has been prompted by the necessity to enhance the surveillance of individuals with heart conditions through an IoT-based system.
The monitoring system for CPs is a specific decision-making system. It is designed to collect real-time health data from sensors to provide medical care to CPs at a distance. It is a simulated consultation from a doctor to the patient that enables the patient’s medical data to be viewed, monitored, and analyzed instantly. Therefore, in essence, as we are still in the period of Coronavirus (or Covid 19), the proposed remote monitoring system for CPs bears great significance in reducing needless visits to the hospital and emergency room [7-9]. In this sense, many research projects and systems management with CPs have been engineered. In this context, we mention some works.
Gharsellaoui et al. [10] have provided a new approach for CPs based on pacemaker devices. In this work, the authors developed a new e-Health Application (or e-HA) based on an IoT system for CPs who still have a heart problem and are employing a pacemaker device. The e-HA developed by the authors offers the following three functions: heart rate measurement, blood pressure monitoring, and oxygen consumption monitoring. As a result of this, the primary goal of the proposed e-HA is to assist the CPs who have a pacemaker whenever and wherever they are. In conclusion, the authors attested that the proffered e-HA based on the IoT system is the first solution through cloud computing-based applications for CPs with pacemakers in real-time and alerting the proposed system in the event of an abnormal behavior [10].
Health information and communication technology (ICT) encompasses the various activities and solutions facilitated by computing resources. These resources enable the collection, processing, storage, transmission, access, and utilization of healthcare information. Additionally, they facilitate digital communication between individuals and organizations in the healthcare sector [11-17]. In the scope of this study, Esteves et al. [11] invented a widespread web application that notifies patients, their caretakers, and family members through SMS messages. These alerts are sent in advance and, when necessary, as determined by healthcare specialists, from the Clinical Indicators basis of Business Intelligence (or CIBI) database. As the authors explained, the proposed CIBI application is more professional, cheaper, faster, and more customizable than sending text messages directly from a smartphone. As a final point, the authors agreed that the proffered CIBI application can reduce waste of time, personnel, and cost [11]. In addition, there is the possibility of a system that can be adapted to the patient’s behavior. In this regard, Botia et al. [18] designed a specific monitoring system named “AAL: Ambient Assisted Living” to monitor patients living by themselves. In the same context [18], Sung and Chang [19] introduced an Android-based application for the IoT that is designed for the Home Remote Health Care (HRHC) system. The authors suggest an HRHC system that leverages a multi-sensor data fusion method to gather and evaluate medical data for patient diagnosis. This is achieved through the use of cloud computing power. Ultimately, the key element of the HRHC system is the identity preservation of the patients [19].
Onasanya et al. [20] launched a new system project called “Smart Saskatchewan Healthcare (or SSH)”, which exploits IoT and Wireless Sensor Network (or IoT/WSN) technologies. The SSH system has been suggested by the authors, incorporating four services: Business Analytics and Cloud Services (BACSs), Emergency Services (Ess), Operational Services (Oss), and Cancer Care Services (CCSs). The authors’ SSH system has several benefits, including enhancing the electronic medical record project and supporting existing healthcare service delivery alternatives to ensure a high quality of life for CPs, as demonstrated in reference [20].
Ahmed et al. [21] offered a Portable Cardiac Monitoring (PCM) system for CPs. The authors suggested that, based on the hybrid PCM system, a mobile Android application is used to perform cardiac monitoring in a better way, which is employed together with a sensor, to carry out real-time monitoring of the ECG signal, and that for protecting the CPs from life-threatening situations. However, the PCM system has an integrated Bluetooth module for point-to-point communication between the smartphone application and the PCM system, which will be provided for the CPs [21]. In brief, the advantage of a PCM system compared to a conventional cardiac monitoring system is that, first, it is a more efficient telemedicine solution for supporting CPs at home, especially in remote locations, and second, it has great potential to reduce the time required for clinical procedures.
In the same context, Singh et al. [22] developed a wearable ECG sensor for CPs home care, at low cost, which employs Bluetooth wireless capability for displaying real-time ECG signals on a smartphone application using the Android platform.
The cardiovascular value of Blood Pressure (or BP) is enormously variable. Therefore, continuous monitoring of BP should be particularly useful clinically. However, this is a difficult task to perform in a non-hospital environment [23]. For this context, Gong et al. [23] developed a flexible, next-generation wearable system with an integrated gold nanowire, which is designed for continuous non-invasive dynamic cardiac monitoring and for improving the treatment of patients with cardiovascular disease.
Khullar et al. [24] aimed to introduce and evaluate a system that combined IoT and edge (fog) computing to monitor and track health information in real time. The suggested system, referred to as the IoT Fog-Enabled Multi-Node Centralised Ecosystem (FCMN), is designed to promote efficient early detection to identify people who might have been impacted by potentially deadly illnesses such as COVID-19. The proposed system by the authors uses IoT nodes strategically placed in numerous areas to capture body temperature, facial images, and GPS information from people in a non-contact manner. The data is then securely transmitted to a cloud database, allowing healthcare providers and government authorities to track and assess the situation immediately. The goal is to create an intelligent system that can identify, track, and monitor persons who may pose a risk to the spread of infectious diseases early on. This approach is intended to reduce human error while allowing for the introduction of suitable preventative actions [24].
To improve IoT health systems’ security and efficiency, however, the authors have suggested a solution that appears to be promising, termed CSSS (Certificateless Secure Signature) [25]. Through the combination of digital signature and cryptography in a unique process, the technique of CSSS removes the complications related to the management of certificates experienced by traditional signature systems, and consequently, the simplicity of the management of certificates is attained. Additionally, the use of elliptic curve cryptography enables the generation of both strong and secure keys, which provide essential security properties. So security will be enhanced as much as possible. In the end, for resource-constrained IoT devices, the CSSS technique is intended to provide strong security while maintaining computational efficiency [25].
Krishna et al. [26] proposed an IoT nano-quantum antenna based on a circuit in which serial and parallel R-L-C high-pass filters are combined. It appears that the method of obtaining an equivalent circuit was created especially to make it possible to represent this novel kind of tiny quantum antenna for the IoT. Furthermore, the methodology leverages the characteristic modes’ frequency to produce the overall response. In this paper, important factors, including input impedance, quality factor, and resonant frequency, are assessed. Additionally, a rational formulation of the frequency coefficients of the fundamental circuits is used to derive the circuit parameters. It would also be possible to use these quantum antennas as optical sensors in biomedical engineering, fast wireless communications, and optical imaging solutions, employing an analyte material to monitor frequency deviations [26].
Research in healthcare is mostly concerned with the IoT and medical device connectivity. The application of healthcare data has received very little scientific attention. Nonetheless, as we will demonstrate in this paper, it is feasible to incorporate this data into AI to support sustainability. The laborious, labor-intensive, and error-prone management of health data frequently results in a lack of trust within companies. For instance, in order to ensure the safe flow of data between the different stakeholders in the healthcare industry, Rana et al. [27] proposed establishing a system based on blockchain technology. Furthermore, they created a distributed access architecture that provides accurate access control, immutability, and traceability to medical records, all based on the Ethereum blockchain [27].
Recent advances in ECG signal classification have been marked by progressively sophisticated deep learning models, which have achieved high diagnostic performance. Shan et al. [28] develop and evaluate an automatic ECG anomaly detection framework called ECG-AAE, which leverages an adversarial autoencoder and temporal convolutional network (TCN), to efficiently detect abnormal ECG signals using only normal ECG data during training. The ECG-AAE framework was tested on two public datasets: the MIT-BIH arrhythmia and CMUH. Achieved strong performance, with 96.73% accuracy, 94.86% Recall, 98.6% specificity, and 96.99% F1-score, demonstrating its effectiveness for arrhythmia detection. Rajpurkar et al. [29] developed a 34-layer deep Convolutional Neural Network (CNN) for arrhythmia detection, reporting 92.0% accuracy, 92.6% sensitivity, and 95.3% specificity, reaching cardiologist-level precision. Building on CNN architectures, Acharya et al. [30] introduced a 9-layer CNN model for automated heartbeat classification, improving results to 94.03% accuracy, 94.9% sensitivity, and 96.8% specificity by enhancing feature learning. Kachuee et al. [31] advanced the field by incorporating ResNet with raw ECG signals and RR intervals, achieving 93.4% accuracy, 91.7% sensitivity, and 93.4% specificity, demonstrating the power of deep residual connections. Shifting toward attention-based mechanisms.
Most recently, Mika and Komorowski [32] proposed a novel method for atrial fibrillation (AFIB) detection based on higher-order spectral analysis, specifically the bispectrum of ECG signals, combined with Convolutional Neural Networks (CNNs). Recognizing that ECG signals are inherently non-linear, non-stationary, and non-Gaussian, the authors utilized bispectral representations to preserve higher-order statistical features critical for distinguishing AFIB rhythms. Their approach involved transforming ECG signals into two-dimensional bispectrum images, which were then fed into two CNN models: a pre-trained, modified GoogLeNet and a newly designed architecture called AFIB-NET. Using the MIT-BIH Atrial Fibrillation Database (AFDB), AFIB-NET achieved a accuracy of 94.5%, sensitivity of 95.3%, specificity of 93.7%, and an AUC of 98.3%, while GoogLeNet showed a sensitivity of 96.7%, specificity of 82%, and AUC of 96.7%. Irid et al. [33] proposed a Bidirectional Long Short-Term Memory (BiLSTM) deep neural network (DNN) for classifying ECG signals and detecting cardiac arrhythmias, trained on the five-class MIT-BIH dataset. To handle class imbalance, they applied re-sampling techniques during data preprocessing. Using a multiple-class classification framework, the BLSTM model achieved outstanding results, reaching 98.25% accuracy in accurately identifying five distinct arrhythmia types.
Hassan et al. [34] introduced a CNN-BiLSTM hybrid model for automatically classifying cardiac arrhythmias from ECG signals. The MIT-BIH and St. Petersburg datasets were used to assess the model, which can distinguish between five beat types (N, S, V, F, and Q). On MIT-BIH, its accuracy is up to 98%. The method demonstrates the efficacy of deep learning for accurate and timely arrhythmia diagnosis and outperforms a number of current models.
This section offers a thorough analysis of a few pertinent studies. Our discussion will be expanded by summarizing and critically assessing these studies, as demonstrated by our examination of the work provided by Rajpurkar et al. [29]. Despite its contributions, the study's large dataset, sourced from a single-lead wearable monitor, limits its generalizability to other ECG devices or multi-lead hospital settings. Furthermore, the study's deep 34-layer CNN is too computationally demanding for low-power IoT or wearable devices, and it ignores class imbalance, which could weaken robustness.
Mika and Komorowski [32] introduced an interesting approach, but it had a few limitations. The model focused only on binary classification (AFIB vs. no-AFIB), limiting its applicability to other arrhythmia types. The paper also lacks a discussion of real-time implementation and the computational overhead of bispectrum feature extraction.
Furthermore, an optimized CNN for ECG class detection that was implemented on a Pynq-Z2 FPGA board was proposed by Fradi et al. [35]. Despite its remarkable results, the study has several flaws. The evaluation is restricted to the MIT-BIH dataset and has not been verified on diverse populations or noisy real-world ECG signals. Furthermore, generalization to other conditions or multi-lead inputs is not covered; it solely addresses ECG class detection. Finally, large-scale or low-cost deployment may be limited by the relatively high cost and specialized development effort required for FPGA hardware, especially in healthcare settings with limited resources.
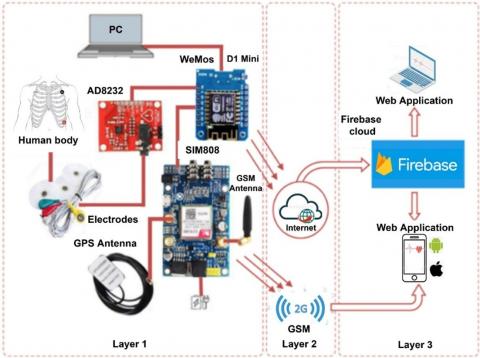
An IoT model consists of three main layers. Our proposed prototype follows this same decomposition (see Figure 1). The first layer is equipped with a WeMoS D1 Mini board (ESP8266) to perform the necessary calculations and at the same time connect to the WiFi network to transmit the data collected by the system to the database in real-time, a GSM/GPRS/GPS module (SIM808) equipped with a GPS antenna to detect the GPS position of the CPs, a GSM antenna to send an SMS alert in the event of anomalies, and a heart rate sensor (AD8232) to pick up the ECG signal. For the second layer, we will use a wireless AP (or WiFi network) to connect to the Internet to send the information collected by the sensor, and a SIM card to attach to GSM networks in order to alert. In the third layer, we used IoT Cloud platforms to receive the information sent by our system; in addition, we developed a web application. This system operates by first acquiring a patient’s ECG signal through the AD8232 sensor. It then calculates the number of heartbeats per minute and compares it with standard values to identify any cardiac abnormalities. Detected abnormalities are promptly transmitted in real-time to a database via WiFi, facilitated by the WeMoS. Additionally, in instances of abnormalities, the system activates GPS to pinpoint the patient’s location and dispatches SMS alerts to the doctor through the SIM808 module.
3.1 WeMos D1 Mini (ESP8266)
The Arduino platform offers a vast selection of modules (>20), including Arduino UNO, Mini, Nano, Micro, and Mega2560 [36]. However, for this project, we opted for the WeMos D1 Mini (ESP8266) module due to its convenient Wi-Fi connectivity without requiring an additional shield.
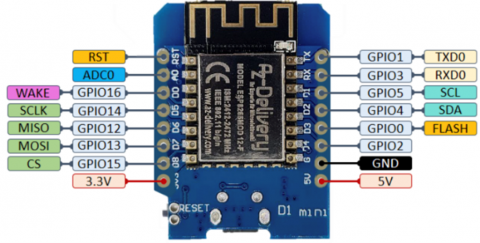
The WeMos D1 Mini is a microcontroller board with a built-in Wi-Fi module [37-40]. This low-cost development board caters specifically to the IoT. It offers user-friendly operation and boasts superior memory and processing power compared to Arduino boards. The module can function as a client or server on existing Wi-Fi networks, or even establish its own network using a Wi-Fi transceiver. Figure 2 illustrates the various pins on the WeMos D1 module.
Figure 1. Cardiac monitoring and alert system
Figure 2. The pins of the WeMos D1 Mini module
3.2 GSM/GPRS/GPS module (SIM808)
The SIM808 is a compact module developed by SIMCOM. This module integrates GSM/GPRS and GPS functionalities. It supports quad-band frequencies (850/900/1800/1900 MHz) and incorporates GPS technology for satellite navigation with 22 tracking channels and 66 acquisition receiver channels. This combined solution streamlines development by reducing the time, energy, and cost associated with creating GPS-based applications. The SIM808 operates on 3.3V or 5V and is controlled using AT commands. It connects directly to GSM and GPS antennas via an external connector. The key functionalities of the GSM/GPRS/GPS module (SIM808) include [6, 41]: transmission and reception of GPRS data (TCP/IP, HTTP, etc.); reception of GPS and A-GPS data; transmission and reception of SMS; transmission and reception of telephone calls.
3.3 Connecting the WeMos board with the SIM808 module
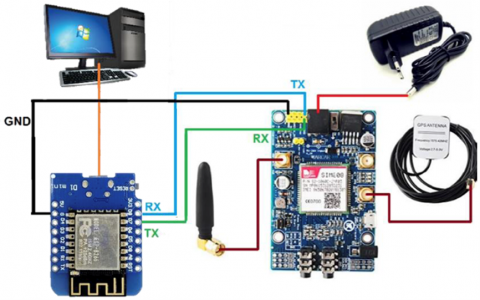
The setup, as shown in Figure 3, represents a location system using the SIM808 module. This system can determine the position of the CPs thanks to a GPS receiver and allows sending its position information by SMS to the doctor. For this to work, it is necessary to have a SIM card.
Figure 3. Communication of the WeMoS card and the SIM808 card
This section provides a detailed presentation of the suggested system’s design, which is specifically designed to monitor heart attacks. We start by assembling the system, then describe the algorithms used to operate it, and finally present the obtained experimental results. The monitoring system we have developed consists, as described above, of a WeMoS D1 Mini board (ESP8266), a GSM/GPRS/GPS module (SIM808), and a heart rate sensor (AD8232).
The system is managed by the WeMoS D1 Mini, which relies on the ESP8266 to manage communications and data processing. The SIM808 module provides the ability to connect to a cell and track its GPS location. Finally, the AD8232 device assesses the heart’s electrical activity to identify the risk of heart attacks.
4.1 Overall IoT system operation algorithm
The operating principle of this system is to read the ECG signal captured by the AD8232 sensor and count the number of beats per minute and compare it to normal values to detect and diagnose cardiac abnormalities, and then send it to the cloud via the WeMoS module that provides us with the WiFi connection. On the other hand, the system is equipped with a SIM808 module, which provides geolocation by GPS and allows SMS alerts to be sent to the doctor in the event of anomalies observed in the patient.
The overall algorithm of system operation contains two main functions, as well as the import of libraries. We imported the following libraries:
In the setup function, we have configured the serial connection at the speed of 19200 bauds for the ESP8266 and the SIM808, configured the input-output pins, and defined the WiFi parameters. The setup function is executed only once, after each power-up or reset of the WeMoS board. The loop function runs in an endless loop, in which it is checked that the electrodes are first placed on the body so that the function of reading the electrocardiogram is called to calculate the number of heartbeats to compare it to normal values and determine the patient’s health status, then all values are sent to the Firebase cloud [42-46].
The IoT cardiac monitoring prototype integrates the AD8232 ECG sensor, a WeMos D1 Mini microcontroller, and a SIM808 GSM/GPRS/GPS module in a sequential pipeline. The AD8232 captures analog ECG signals, which the WeMos digitizes, preprocesses, and forwards either to a Firebase cloud database via Wi-Fi or to the SIM808 for geolocation and SMS alerts. Potential latency arises at three stages: (1) analog-to-digital conversion and local processing on the WeMos (a few milliseconds), (2) Wi-Fi transmission to the cloud, where network congestion can add variable delay, and (3) GPRS/GSM-based SMS dispatch, which typically incurs the highest latency (up to a few seconds). Geolocation data is reliably connected to anomalies that are detected, and buffering guarantees that no data is lost. Overall, the system achieves clinically acceptable real-time performance for remote arrhythmia detection while maintaining signal integrity despite slight delays.
4.2 Algorithmic structure of the system workflow
Algorithm 1 represents the overall IoT system. Additionally, the heart rate calculation is executed through the ReadHeartBeat function, which involves counting the number of beats within a ten-second interval and then multiplying this count by 6.
Algorithm 2 illustrates the underlying principle of this function. Moreover, the sendData function allows us to store ECG values in character strings and send them to Firebase every 10 seconds. The operation of this function is described by Algorithm 3. Finally, the main role of the sendGPSbySMS function is to read the GPS value received by the SIM808 and then send it via SMS (see Algorithm 4).
|
Algorithm 1: Overall IoT system |
|
Require: Libraries importation pins definition Variables declaration and initialization Objects creation setup Function I/O pin configuration Connection to the WiFi network Firebase configuration SIM808 configuration loop Function if (LO+ = 1 & LO− = 1) then return to loop function else call ReadHeartBeat() Function sendData() Function if (BP M < 60 or BP M > 100) then call sendGPSbySMS() Function end if end if End |
|
Algorithm 2: ReadHeartBeat Function |
|
Require: Read ECG values if (peak detected) then Increment number of peaks Calculate RR interval Turn on LED else Turn off LED end if if (Time > 10s) then Calculate BMP Reset variables end if |
|
Algorithm 3: SendData Function |
|
if (Time < 9s) then store ECG values else send BMP value to Firebase send ECG value to Firebase end if |
|
Algorithm 4: SendGPSbySMS Function |
|
if (get GPS value) then send GPS values by SMS else read the GPS value received by SIM808 end if |
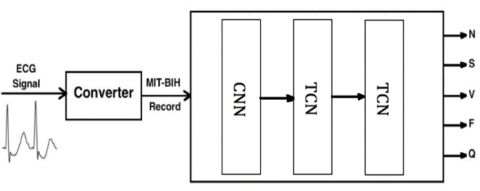
A schematic of the proposed artificial intelligence classifier is illustrated in Figure 4. To ensure compatibility with the CNN-TCN classifier [47-49], an ECG signal indicating a potential cardiac anomaly must be converted into the format of the MIT-BIH Arrhythmia Database before cloud transmission. This conversion aligns the real-time data from the AD8232 module with the classifier's foundational training dataset. This conversion was motivated by the fact that the MIT-BIH dataset remains the benchmark reference for arrhythmia detection studies, and aligning our input data with its specifications allows both interoperability and meaningful comparison with existing literature. There were multiple sequential steps in the process. To reduce noise while preserving clinically meaningful information, digital bandpass filtering in the 0.5-40 Hz range was used to condition the raw ECG signals, which inherently contain baseline wander, muscular artifacts, and powerline interference. Baseline drift was corrected using polynomial detrending or high-pass filtering, and amplitude normalization was applied to match the 10 mV range and 11-bit resolution characteristic of MIT-BIH recordings. Since the AD8232 module does not natively sample at 360 Hz, which is the standard sampling frequency of MIT-BIH signals, the ECG traces were resampled by interpolation to precisely align with this reference rate. Once preconditioning was complete, the continuous signals were segmented into heartbeat-centered windows. This segmentation relied on R-peak detection, typically via a threshold-based or Pan-Tompkins method, followed by extraction of fixed-length intervals of 187-188 samples around each peak, replicating the structure used in the MIT-BIH CSV version. Each segment was then annotated with a heartbeat label (Normal, Supraventricular, Ventricular, Fusion, or Unknown) based on its morphological and temporal features. Finally, the preprocessed data was saved in the canonical MIT-BIH file structure consisting of three complementary files: a .dat file containing the ECG waveform, a .hea header file storing metadata such as patient ID, duration, and sampling rate, and an .atr file recording annotations and beat locations. In addition to making our deep learning experiments reproducible and allowing for equitable benchmarking against earlier work in ECG-based arrhythmia detection, this structured pipeline guarantees that the real-time signals are rendered fully interoperable with PhysioNet-compatible tools. The MIT-BIH Arrhythmia Database is a widely recognized benchmark in the field, forming the basis for numerous research initiatives, including the development of arrhythmia detection algorithms and the evaluation of diagnostic methodologies across a broad range of studies [50-54].
Figure 4. ECG classifier
Combining Convolutional Neural Networks (CNN) with Temporal Convolutional Networks (TCN) in a single model offers a powerful approach for analyzing sequential and time-series data. CNNs are effective at extracting local temporal features through small, sliding convolutional windows, allowing the model to detect short-term patterns or fluctuations. In contrast, TCNs leverage dilated causal convolutions to capture long-range dependencies efficiently across time, enabling the model to understand broader temporal relationships without the limitations of recurrent structures. By integrating CNN and TCN layers, the model benefits from both detailed local feature extraction and a wide temporal receptive field, leading to improved accuracy and robustness. This hybrid architecture also trains faster and more efficiently than traditional RNNs or LSTMs, as it allows for full parallelization and avoids issues like vanishing gradients. Overall, the combination enhances the model’s ability to generalize across complex temporal dynamics, making it particularly suitable for applications such as intrusion detection in IoMT, physiological signal analysis, or any domain involving multiscale temporal patterns.
5.1 Dataset description
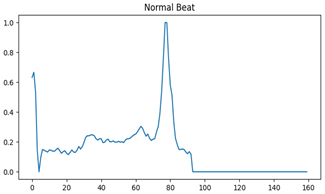
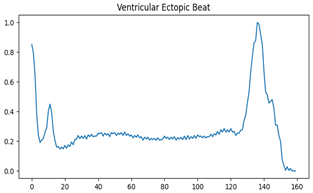
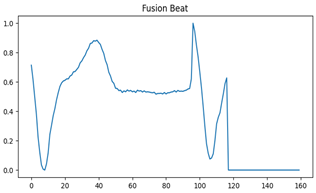
To train our system for arrhythmia classification, we leveraged the well-established MIT-BIH arrhythmia dataset. This dataset adheres to the Association for the Advancement of Medical Instrumentation (AAMI) EC57 standard [55] and encompasses 48 ECG recordings, each lasting 30 minutes. The recordings originated from 47 different patients. The dataset features digitized ECG data with a sampling rate of 360 Hz per channel, 11-bit resolution, and two types of ECG signals-Lead II and Lead V5-captured within a 10 mV range. For this experiment, we specifically focused on Lead II ECGs. We extracted the ECG recordings, applied appropriate scaling, and segmented them into five categories (Table 1, Figures 5-9): Normal (N), Supraventricular (S), Ventricular (V), Fusion (F), and Unknown (Q) [56].
Table 1. Distribution of heartbeat category in the MIT-BIH dataset [33, 50]
|
Beat Type |
Target |
Number of samples |
Percentage (%) |
|
Normal (N) |
0 |
72494 |
82.87 |
|
Supraventricular ectopic (S) |
1 |
2188 |
2.5 |
|
Ventricular ectopic (V) |
2 |
5788 |
6.62 |
|
Fusion (F) |
3 |
613 |
0.7 |
|
Unknown beat (Q) |
4 |
6391 |
7.31 |
Figure 5. Normal beat
Figure 6. Unknown beat
Figure 7. Ventricular ectopic beat
Figure 8. Supraventricular ectopic beat
Figure 9. Fusion beat
Table 2. One-hot encoding
|
Class |
One-Hot Vector |
|
0 1 2 3 4 |
[1, 0, 0, 0, 0] [0, 1, 0, 0, 0] [0, 0, 1, 0, 0] [0, 0, 0, 1, 0] [0, 0, 0, 0, 1] |
The MIT-BIH dataset is structured as two separate CSV files: one dedicated to the train set and the other for the test set. Both files share the same format, containing 109446 samples, with each sample comprising 188 unique features. As you may observe in Table 2 (which is assumed to be present elsewhere in the document), the dataset exhibits an imbalance in class distribution-certain arrhythmia types might be underrepresented compared to others. We have applied re-sampling techniques [57] to balance the data distribution in order to address the problem of class imbalance and guarantee a more dependable training process. This was implemented using the resample module from scikit-learn, which applies bootstrapping to generate consistent re-samples of arrays or sparse matrices. We have used a random oversampling technique in the MIT-BIH dataset because there is a significant imbalance among the five arrhythmia categories. Specifically, minority classes such as Supraventricular, Ventricular, Fusion, and Unknown were bootstrapped until their sample frequencies matched that of the majority class, Normal beats. This decision preserved the entire set of normal beats while avoiding the loss of important pathological signals that would have resulted from undersampling. Consequently, a balanced dataset was used to train the CNN-TCN classifier, which improved sensitivity to uncommon arrhythmias and decreased bias toward regular heartbeats. Empirical evaluation confirmed that this strategy improved recall for underrepresented categories, particularly Fusion and Supraventricular, without significantly compromising overall specificity. Finally, by avoiding systematic under-recognition of minority arrhythmia types while preserving strong global performance, oversampling improved the classifier's robustness and fairness.
5.2 Multi-class classification
For our arrhythmia detection task, we employ the dataset in its original form with five distinct heartbeat categories: Class 0 (Normal/N), Class 1 (Supraventricular Ectopic/S), Class 2 (Ventricular Ectopic/V), Class 3 (Fusion/F), and Class 4 (Unknown/Q). The complete dataset comprises 109,446 samples, each containing 188 dimensions. The feature space spans columns 0-186, representing the ECG waveform characteristics and derived metrics, while column 187 serves as the classification target containing the annotated heartbeat categories (0-4).
5.3 One-hot encoding
To prepare the data for machine learning algorithms, a pre-processing step is crucial. In this instance, we’ll employ one-hot encoding [58-60] to transform the categorical target variable (“Label”) into a numerical representation suitable for the classification task.
One-hot encoding works by creating a unique binary vector for each class within the target variable. The length of each vector corresponds to the total number of classes. Within a specific vector, a value of 1 is placed in the position matching the class label of the corresponding data sample, while all other positions are filled with 0s (refer to Table 2 for illustration).
For example, if a data sample belongs to class 0 (normal heartbeat), its one-hot encoded vector would be [1, 0, 0, 0, 0]. This approach ensures that the machine learning model can effectively interpret the class labels as numerical features.
5.4 Model implementation
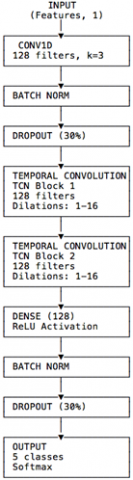
The suggested architecture performs multi-class classification of time-series data, including ECG signals, by combining layers of Temporal Convolutional Networks (TCN) with a one-dimensional Convolutional Neural Network (1D-CNN). In order to extract local temporal features, like sharp QRS complexes, while maintaining morphological detail, the network starts with a 1D convolutional layer with 64 filters and a kernel size of 3. To improve training stability and reduce overfitting, batch normalization and dropout are then used. This convolutional front-end is followed by two stacked TCN blocks, which capture both short- and long-term dependencies within the beat sequence. The first TCN layer, configured with return_sequences=True, outputs the full temporal representation, whereas the second, with return_sequences=False, condenses the signal into a single feature vector. Each TCN block employs 128 filters, a kernel size of 3, and exponentially increasing dilation rates [1, 2, 4, 8, 16], yielding an effective receptive field of approximately 125 samples across the two blocks. Given that each input beat consists of 188 samples at 360 Hz (≈0.52 s), this receptive field spans the QRS complex and substantial portions of the P and T segments, thus aligning well with the physiological duration of a heartbeat and supporting accurate discrimination of AAMI classes. Following the TCN layers, the network includes a dense layer with 128 neurons, batch normalization, and dropout, before terminating in a softmax output layer with five units corresponding to the arrhythmia classes. A dropout rate of 0.30 was empirically selected as the lowest value that consistently minimized the train-validation generalization gap without degrading validation accuracy. Together with L2 regularization, this setting prevented overfitting, as reflected in high validation accuracy and a small terminal train-validation error gap. The chosen filter widths (CNN: 64; TCN: 128) represent a trade-off observed during internal tuning on MIT-BIH splits: they provided sufficient capacity to preserve recall for minority rhythms while maintaining model compactness, an essential requirement for IoT-based deployment.
The Adam optimizer and categorical cross-entropy loss were used to train the model over 100 epochs with a batch size of 512. Together, these training and architectural choices achieve a balance between local morphology extraction and long-range temporal context, resulting in a classifier with high accuracy and specificity that is computationally efficient for deployment in resource-constrained environments.
One-hot encoding is a method utilized to represent categorical data using binary vectors. Each category is depicted by a vector wherein all values are zero except for one, which is set to one, signifying the particular category. This technique finds extensive application in machine learning, especially for handling categorical variables. It enables the transformation of qualitative data into a numerical format usable by machine learning algorithms. Consequently, one-hot encoding streamlines data manipulation and enhances the performance of machine learning models, particularly in classification and prediction tasks. Figure 10 gives the diagram of the used CNN-TCN.
5.5 Results and discussion
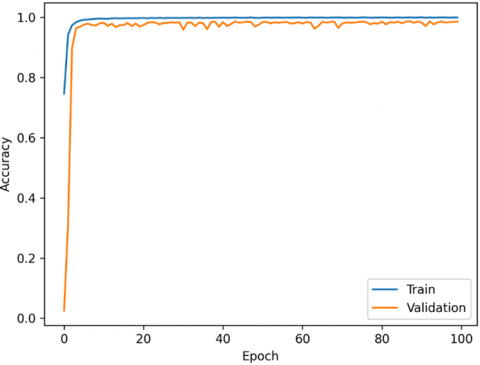
This study implemented a combined Convolutional Neural Network (CNN) with Temporal Convolutional Networks (TCN) in a single model. Extensive testing was conducted to optimize hyperparameters such as network layers, epochs, optimizer selection, and activation functions. The model was trained on a designated training set with validation on a separate set. This iterative process ensured optimal parameter selection. Finally, the model’s effectiveness was evaluated on a dedicated test set. The model achieving the highest accuracy (99.49% training, 96.26% validation) was selected (see Figure 11).
Figure 10. Diagram of the used CNN-TCN model
Figure 11. Model accuracy as a function of epochs during the training process
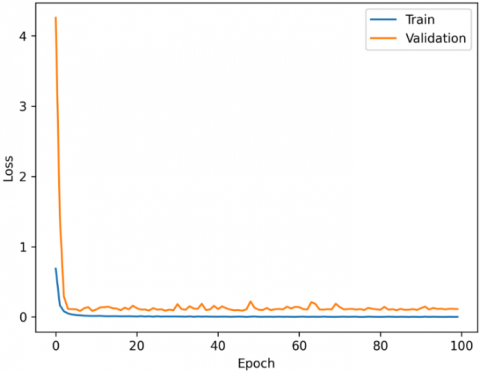
Figure 12. Model loss as a function of epochs during the training process
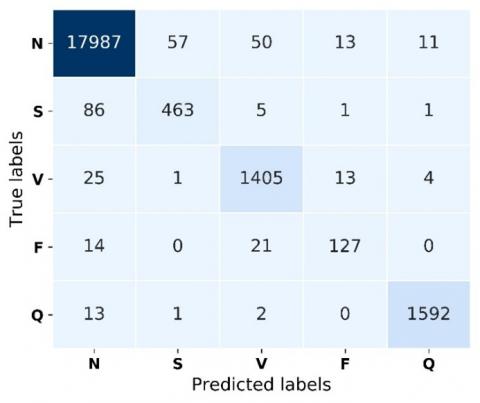
Figure 13. Confusion matrix
The outcomes of this method reveal loss values for both training and validation. Specifically, the training loss stands at 1.5%, while the validation loss is 17.64%, as depicted in Figure 12. Notably, the model achieves optimal accuracy without overfitting the training dataset, accomplished through the application of L2 regularization. Towards the end of the training process, the disparity between training and validation errors (the bias) diminishes, with a margin smaller than 0.1. This reduction indicates a mitigated overfitting of the model to the training examples.
Figure 13 shows the confusion matrix of results for the five classes for the CNN-TCN network. A confusion matrix is used to evaluate the algorithms based on parameters related to accuracy, precision, True Positive Rate (Recall), and the false positive rate metrics [57]. As we can see, the values along the main diagonal of the confusion matrix are high, meaning that our model was successful in correctly classifying the different Heartbeat signals. From this confusion matrix, the values of accuracy, sensitivity, and specificity are 98.55%, 91.2%, and 99.2%, respectively.
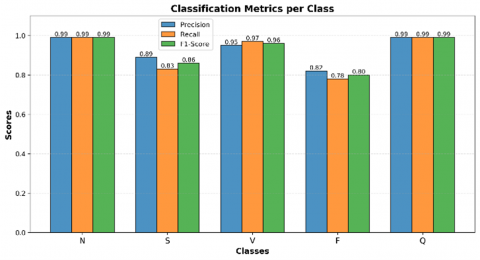
The following charts (see Figures 14 and 15) provide a detailed classification report along with per-class accuracy, where Class 0 (N) represents Normal Heartbeats, Class 1 (S) corresponds to Ectopic Supra-ventricular Beats, Class 2 (V) denotes Ectopic Ventricular Beats, Class 3 (F) indicates Fusion Beats, and Class 4 (Q) refers to Unknown Beats (see Table 1). Figure 9 summarizes precision, recall, and F1-score for each class, while Figure 10 depicts the accuracy distribution across individual classes.
The confusion matrix demonstrates that classification errors are negligible. Such promising outcomes underscore the robustness of our CNN-TCN approach for ECG signal classification. Consequently, we opted to employ the proposed model for real-time analysis of ECG signals, aiming to aid healthcare professionals in the detection and diagnosis of cardiac abnormalities. Table 3 presents a comprehensive comparative analysis of the performance of our proposed CNN-TCN model against previously reported methods in the literature, specifically highlighting improvements in classification evaluation metrics, accuracy (ACC), sensitivity (SEN), specificity (SPE), and F1-Score (F1), across a range of ECG-based arrhythmia detection tasks.
Figure 14. Detailed classification metrics per class
Figure 15. Accuracy distribution across classes
Table 3. Performance comparison between the proposed work and previous studies
|
Reference / Author(s) |
ACC (%) |
SEN (%) |
SPE (%) |
F1 (%) |
|
Rajpurkar et al. [29] |
92.0 |
92.6 |
95.3 |
-- |
|
Acharya et al. [30] |
94.03 |
94.9 |
96.8 |
-- |
|
Kachuee et al. [31] |
93.40 |
91.7 |
93.4 |
-- |
|
Shan et al. [28] |
96.73 |
94.86 |
98.60 |
96.66 |
|
Mika and Komorowski [32] |
95.5 |
95.3 |
93.7 |
94.5 |
|
Irid et al. [33] |
98.17 |
94 |
95.19 |
-- |
|
Hassan et al. [34] |
98.0 |
91.0 |
90.96 |
89.8 |
|
CNN-TCN (Proposed work) |
98.55 |
91.2 |
99.4 |
94.71 |
Our proposed model (CNN-TCN) demonstrates strong but nuanced performance characteristics in sensitivity metrics, achieving a robust 91.2% detection rate for cardiac abnormalities. While this represents competitive performance within the field, it falls slightly below the sensitivity levels reported by Acharya et al. [30] (94.9%) and Mika and Komorowski [32] (95.3%) in their respective studies. This measured difference in sensitivity likely reflects intentional design trade-offs in our architecture, where we prioritized two key factors: (1) maximizing specificity (achieving 99.4%) to minimize false positive diagnoses that could burden healthcare systems, and (2) maintaining balanced accuracy across all five diagnostic classes rather than optimizing for particular abnormality categories.
The suggested model performed well, achieving an F1-score of 94.71%. This result is higher than that reported in study [32] (94.5%) and study [34] (89.8%), but slightly lower than that in study [28], which reported an F1-score of 96.66%.
While recent advanced architectures like AFIB-NET [32], BiLSTM-based models [33], and CNN-BiLSTM hybrid model [34] demonstrate impressive classification performance in terms of accuracy, their practical deployment faces significant challenges due to substantial computational requirements. These sophisticated models typically demand high-power processors, extensive memory resources, and considerable energy consumption-constraints that prove particularly problematic for real-time embedded systems and resource-constrained IoT environments. In contrast, our CNN-TCN hybrid architecture achieves an optimal balance between diagnostic accuracy (98.55%) and computational efficiency. The model maintains a streamlined structure that enables: (1) faster training cycles, (2) lower power consumption, and (3) effective deployment on edge devices-all while preserving clinically relevant classification performance. This efficiency advantage positions our solution as particularly suitable for widespread implementation in both hospital and ambulatory settings, where hardware limitations often dictate system design choices.
This study introduces an innovative Smart IoT Cardiac Patient Monitoring System that bridges advanced sensor technology with cutting-edge deep learning to revolutionize remote cardiac care. At its core, the system combines a robust hardware platform featuring an AD8232 ECG module and a SIM808 communication module interfaced through Arduino architecture with a sophisticated hybrid CNN-TCN deep learning model trained on the clinically validated MIT-BIH dataset. This dual-component architecture achieves remarkable performance metrics, including 98.55% classification accuracy, 99.4% specificity, and 91.2% sensitivity, surpassing existing solutions while maintaining computational efficiency suitable for real-world clinical implementation.
The clinical implications of this integrated system are profound. By enabling continuous, real-time cardiac monitoring with automated abnormality detection, the solution empowers healthcare providers to deliver more timely interventions while extending quality care to traditionally underserved populations. The cloud-based architecture facilitates remote diagnosis while maintaining data security, particularly valuable for rural or resource-constrained settings. Looking ahead, the platform's modular design permits expansion through additional biosensors for comprehensive health assessment, while forthcoming developments in edge computing and personalized model tuning promise to further enhance response times and diagnostic precision. These evolutionary pathways position the system to transition from reactive monitoring to predictive analytics, ultimately advancing preventive cardiology through machine learning-driven risk stratification. Collectively, this work demonstrates how the strategic integration of IoT and artificial intelligence can transform cardiac care delivery, making high-quality monitoring more accessible, intelligent, and proactive across diverse healthcare ecosystems.
[1] Gubbi, J., Buyya, R., Marusic, S., Palaniswami, M. (2013). Internet of Things (IoT): A vision, architectural elements, and future directions. Future Generation Computer Systems, 29(7): 1645-1660. https://doi.org/10.1016/j.future.2013.01.010
[2] Farooq, U.M., Waseem, M., Mazhar, S., Khairi, A., Kamal, T. (2015). A review on Internet of Things (IoT). International Journal of Computer Applications, 113(1): 1-7. https://doi.org/10.5120/19787-1571
[3] Lilhore, U.K., Imoize, A.L., Li, C.T., Simaiya, S., Pani, S.K., et al. (2022). Design and implementation of an ML and IoT based adaptive traffic-management system for smart cities. Sensors, 22(8): 2908. https://doi.org/10.3390/s22082908
[4] Asghari, P., Rahmani, A.M., Javadi, H.H.S. (2019). Internet of Things applications: A systematic review. Computer Networks, 148: 241-261. https://doi.org/10.1016/j.comnet.2018.12.008
[5] Yuehong, Y.I.N., Zeng, Y., Chen, X., Fan, Y. (2016). The internet of things in healthcare: An overview. Journal of Industrial Information Integration, 1: 3-13. https://doi.org/10.1016/j.jii.2016.03.004
[6] Baker, S.B., Xiang, W., Atkinson, I. (2017). Internet of things for smart healthcare: Technologies, challenges, and opportunities. IEEE Access, 5: 26521-26544. https://doi.org/10.1109/ACCESS.2017.2775180
[7] Benjemmaa, A., Ltifi, H., Ayed, M.B. (2020). Design of remote heart monitoring system for cardiac patients. In Advanced Information Networking and Applications: Proceedings of the 33rd International Conference on Advanced Information Networking and Applications (AINA-2019), pp. 963-976. https://doi.org/10.1007/978-3-030-15032-7_81
[8] Lan, M., Samy, L., Alshurafa, N., Suh, M.K., Ghasemzadeh, H., Macabasco-O'Connell, A. Sarrafzadeh, M. (2012). Wanda: An end-to-end remote health monitoring and analytics system for heart failure patients. In Proceedings of the Conference on Wireless Health, New York, United States, pp. 1-8. https://doi.org/10.1145/2448096.2448105
[9] Lee, S.I., Ghasemzadeh, H., Mortazavi, B.J., Lan, M., Alshurafa, N., Ong, M., Sarrafzadeh, M. (2013). Remote health monitoring systems: What impact can data analytics have on cost. Wireless Health, 10: 2534088-2534108. https://doi.org/10.1145/2534088.25 34108
[10] Gharsellaoui, H., Khemaissia, I., AlShahrani, A. (2023). New approach for cardiac patients based on pacemaker device. Journal of Ambient Intelligence and Humanized Computing, 14(11): 15205-15213. https://doi.org/10.1007/s12652-020-02870-7
[11] Esteves, M., Abelha, A. Machado, J. (2022). The development of a pervasive Web application to alert patients based on business intelligence clinical indicators: A case study in a health institution. Wireless Networks, 28(3): 1279-1285. https://doi.org/10.1007/s11276-018-01911-6
[12] Zhang, N.J., Seblega, B., Wan, T., Unruh, L., Agiro, A., Miao, L. (2013). Health information technology adoption in US acute care hospitals. Journal of Medical Systems, 37: 1-9. https://doi.org/10.1007/s10916-012-9907-2
[13] Finney Rutten, L.J., Agunwamba, A.A., Greene, S.M., Mazor, K.M., Ebbert, J.O., St Sauver, J.L., Dearing, J.W. (2014). Enabling patient-centered communication and care through health information technology. Journal of Communication in Healthcare, 7(4): 255-261. https://doi.org/10.1179/1753807614Y.0000000067
[14] Mamlin, B.W., Tierney, W.M. (2016). The promise of information and communication technology in healthcare: Extracting value from the chaos. The American Journal of the Medical Sciences, 351(1): 59-68. https://doi.org/10.1016/j.amjms.2015.10.015
[15] Buntin, M.B., Burke, M.F., Hoaglin, M.C., Blumenthal, D. (2011). The benefits of health information technology: A review of the recent literature shows predominantly positive results. Health Affairs, 30(3): 464-471. https://doi.org/10.1377/hlthaff.2011.0178
[16] Mettler, T., Vimarlund, V. (2009). Understanding business intelligence in the context of healthcare. Health Informatics Journal, 15(3): 254-264. https://doi.org/10.1177/1460458209337446
[17] Hočevar, B., Jaklič, J. (2010). Assessing benefits of business intelligence systems-A case study. Management: Journal of Contemporary Management Issues, 15(1): 87-119. https://hrcak.srce.hr/53609
[18] Botia, J.A., Villa, A., Palma, J. (2012). Ambient assisted living system for in-home monitoring of healthy independent elders. Expert Systems with Applications, 39(9): 8136-8148. https://doi.org/10.1016/j.eswa.2012.01.153
[19] Sung, W.T., Chang, K.Y. (2013). Evidence-based multi-sensor information fusion for remote health care systems. Sensors and Actuators A: Physical, 204: 1-19. https://doi.org/10.1016/j.sna.2013.09.034.
[20] Onasanya, A., Lakkis, S., Elshakankiri, M. (2019). Implementing IoT/WSN based smart Saskatchewan healthcare system. Wireless Networks, 25(7): 3999-4020. https://doi.org/10.1007/s11276-018-01931-2
[21] Ahmed, H.I., Saleem, D.M., Omair, S.M., Shams, S., Sheikh, N., Tariq, A. (2022). Conceptual hybrid model for wearable cardiac monitoring system. Wireless Personal Communications, 125(4): 3715-3726. https://doi.org/10.1007/s11277-022-09732-9
[22] Singh, M., Singh, G., Singh, J., Kumar, Y. (2021). Design and validation of wearable smartphone based wireless cardiac activity monitoring sensor. Wireless Personal Communications, 119(1): 441-457. https://doi.org/10.1007/s11277-021-08219-3
[23] Gong, S., Yap, L.W., Zhang, Y.X., He, J.Y., Yin, J.L., Marzbanrad, F., Kaye, D.M., Cheng, W.L. (2022). A gold nanowire-integrated soft wearable system for dynamic continuous non-invasive cardiac monitoring. Biosensors and Bioelectronics, 205: 114072. https://doi.org/10.1016/j.bios.2022.114072
[24] Khullar, V., Singh, H.P., Miro, Y., Anand, D., Mohamed, H.G., Gupta, D., Kumar, N. Goyal, N. (2022). IoT fog-enabled multi-node centralized ecosystem for real time screening and monitoring of health information. Applied Sciences, 12(19): 9845. https://doi.org/10.3390/app12199845
[25] Kakkar, L., Gupta, D., Tanwar, S., Saxena, S., Alsubhi, K., Anand, D., Noya, I.D., Goyal, N. (2022). A secure and efficient signature scheme for IoT in healthcare. Computers, Materials and Continua, 73(3): 6151-6168. https://doi.org/10.32604/cmc.2022.023769
[26] Krishna, R., Yaduvanshi, R.S., Singh, H., Rana, A.K., Goyal, N. (2023). Mathematical modeling and parameter analysis of quantum antenna for IoT sensor-based biomedical applications. Journal of Autonomous Intelligence, 6(2): 1-25. https://doi.org/10.32629/jai.v6i2.578
[27] Rana, S.K., Rana, S.K., Nisar, K., Ag Ibrahim, A.A., Rana, A.K., Goyal, N., Chawla, P. (2022). Blockchain technology and artificial intelligence based decentralized access control model to enable secure interoperability for healthcare. Sustainability, 14(15): 9471. https://doi.org/10.3390/su14159471
[28] Shan, L., Li, Y., Jiang, H., Zhou, P., Niu, J., Liu, R., Wei, Y., Peng, J., Yu, H., Sha. X., Chang, S. (2022). Abnormal ECG detection based on an adversarial autoencoder. Frontiers in Physiology, 13: 961724. https://doi.org/10.3389/fphys.2022.961724
[29] Rajpurkar, P., Hannun, A.Y., Haghpanahi, M., Bourn, C., Ng, A.Y. (2017). Cardiologist-level arrhythmia detection with convolutional neural networks. arXiv preprint arXiv:1707.01836. https://doi.org/10.48550/arXiv.1707.01836
[30] Acharya, U.R., Oh, S.L., Hagiwara, Y., Tan, J. H., Adam, M., Gertych, A., San Tan, R. (2017). A deep convolutional neural network model to classify heartbeats. Computers in Biology and Medicine, 89: 389-396. https://doi.org/10.1016/j.compbiomed.2017.08.022
[31] Kachuee, M., Fazeli, S., Sarrafzadeh, M. (2018). ECG heartbeat classification: A deep transferable representation. In 2018 IEEE international conference on healthcare informatics, New York, USA, pp. 443-444. https://doi.org/10.1109/ICHI.2018.00092
[32] Mika, B., Komorowski, D. (2024). Higher-order spectral analysis combined with a convolution neural network for atrial fibrillation detection-preliminary study. Sensors, 24(13): 4171. https://doi.org/10.3390/s24134171
[33] Irid, S.M.H., Moussaoui, D., Hadjila, M., Azzoug, O. (2024). Classification of ECG signals based on MIT-BIH dataset using Bi-LSTM model for assisting cardiologists diagnosis. Traitement du Signal, 41(6): 3245-3253. https://doi.org/10.18280/ts.410640
[34] Hassan, S.U., Mohd Zahid, M.S., Abdullah, T.A., Husain, K. (2022). Classification of cardiac arrhythmia using a convolutional neural network and bi-directional long short-term memory. Digital Health, 8: 1-13. https://doi.org/10.1177/20552076221102766
[35] Fradi, M., Lazhar, K., Zahzah, E.H., Machhout, M. (2024). FPGA implementation of a CNN application for ECG class detection. Traitement du Signal, 41(1): 179-188, 2024. https://doi.org/10.18280/ts.410114
[36] Barrett, S.F. (2022). Arduino Microcontroller Processing for Everyone! Springer Nature. https://doi.org/10.1007/978-3-031-79864-1
[37] Cameron, N. (2021). Electronics Projects with the ESP8266 and ESP32: Building Web Pages, Applications, and WIFI Enabled Devices. Apress Berkeley, CA. https://doi.org/10.1007/978-1-4842-6336-5
[38] Utari, Lukman Hakim. (2022). IOT-based automatic home light monitoring system using WEMOS D1 Mini. Journal of Technomaterial Physics, 4(2): 97-106. https://doi.org/10.32734/jotp.v4i2.8052
[39] Andriani, T., Azzam, M.R., Topan, P.A., Hidayatullah, M., Esabella, S. (2019). Design of flood early detection system using WeMos D1 Mini ESP8266 IoT technology. Journal of Physical Science and Engineering, 4(2): 67-73. https://doi.org/10.17977/um024v4i22019p067
[40] Gowda, M., Gowda, J., Iyer, S., Pawar, M., Gaikwad, V. (2020). Power consumption optimization in IoT based wireless sensor node using ESP8266. In ITM Web of Conferences, Navi Mumbai, India, pp. 03048. https://doi.org/10.1051/itmconf/20203203048
[41] Bharavi, U., Sukesh, R.M. (2017). Design and development of GSM and GPS tracking module. In 2017 2nd IEEE International Conference on Recent Trends in Electronics, Information and Communication Technology, Bangalore, India, pp. 283-288. https://doi.org/10.1109/RTEICT.2017.8256602
[42] Mishra, A., Chakraborty, B., Das, D., Bose, P. (2018). AD8232 based smart healthcare system using internet of things (IoT). International Journal of Engineering Research and Technology, 7(4): 13-16. https://doi.org/10.17577/IJERTV7IS040040
[43] Adardour, H.E., Hadjila, M., Irid, S.M.H., Hachemi, M.H., Benikhlef, M., Benotmane, I. (2021). Embedded system prototype to fight COVID-19 pandemic contamination with less cost. Wireless Personal Communications, 119(4): 3735-3762. https://doi.org/10.1007/s11277-021-08429-9
[44] Moroney, L. (2017). The firebase realtime database. In: The Definitive Guide to Firebase. Apress, Berkeley, CA. https://doi.org/10.1007/978-1-4842-2943-9_3
[45] Li, W.J., Yen, C., Lin, Y.S., Tung, S.C., Huang, S. (2018). JustIoT Internet of Things based on the Firebase real-time database. In 2018 IEEE International Conference on Smart Manufacturing, Industrial and Logistics Engineering, Hsinchu, Taiwan, pp. 43-47. https://doi.org/10.1109/SMILE.2018.8353979
[46] Adardour, H.E., Hadjila, M., Irid, S.M.H., Baouch, T., Belkhiter, S.E. (2021). Outdoor Alzheimer’s patients tracking using an IoT system and a Kalman filter estimator. Wireless Personal Communications, 116(1): 249-265. https://doi.org/10.1007/s11277-020-07713-4
[47] Eedara, P., Dandapat, S. (2023). Multi-label ECG classification using temporal convolutional neural network. arXiv preprint arXiv: 2306.03844. https://doi.org/10.48550/arXiv.2306.03844
[48] Ingolfsson, T.M., Wang, X., Hersche, M., Burrello, A., Cavigelli, L., Benini, L. (2021). ECG-TCN: Wearable cardiac arrhythmia detection with a temporal convolutional network. arXiv preprint arXiv: 2103.13740. https://doi.org/10.48550/arXiv.2103.13740
[49] Alekhya, D., Haritha, D. (2025). Development and comparative analysis of temporal convolutional network for time series data classification. Journal of Neonatal Surgery, 14(13S): 113-122. https://doi.org/10.52783/jns.v14.3195
[50] Moody, G.B., Mark, R.G. (2001). The impact of the MIT-BIH arrhythmia database. IEEE Engineering in Medicine and Biology Magazine, 20(3): 45-50. https://doi.org/10.1109/51.932724
[51] Scherer, J.A., Willems, J.L. (1992). Evaluation of 12-lead ECG synthesis using analysis measurements in 240 patients. In Proceedings Computers in Cardiology, Durham, USA, pp. 91-94. https://doi.org/10.1109/CIC.1992.269439
[52] Goldberger, A.L., Amaral, L.A., Glass, L., Hausdorff, J.M., Ivanov, P.C., Mark, R.G., Stanley, H.E (2000). PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation, 101(23): e215-e220. https://doi.org/10.1161/01.CIR.101.23.e215
[53] Savalia, S., Acosta, E., Emamian, V. (2017). Classification of cardiovascular disease using feature extraction and artificial neural networks. Journal of Biosciences and Medicines, 5(11): 64-79. https://doi.org/10.4236/jbm.2017.511008
[54] De Chazal, P., O'Dwyer, M., Reilly, R.B. (2004). Automatic classification of heartbeats using ECG morphology and heartbeat interval features. IEEE transactions on biomedical engineering, 51(7): 1196-1206. https://doi.org/10.1109/TBME.2004.827359
[55] ANSI/AAMI. (2013). EC57:2012/(R)2020; Testing and reporting performance results of cardiac rhythm and ST segment measurement algorithms. Association for the Advancement of Medical Instrumentation (AAMI). https://doi.org/10.2345/9781570204784
[56] Apandi, Z.F.M., Ikeura, R., Hayakawa, S. (2018). Arrhythmia detection using MIT-BIH dataset: A review. In 2018 International Conference on Computational Approach in Smart Systems Design and Applications, Kuching, Serawak, Malaysia, pp. 1-5. https://doi.org/10.1109/ICASSDA.2018.8477620
[57] Junsomboon, N., Phienthrakul, T. (2017). Combining over-sampling and under-sampling techniques for imbalance dataset. In Procedding of the 9th International Conference on Machine Learning and Computing, New York, USA, pp. 243-247. https://doi.org/10.1145/3055635.3056643
[58] Seger, C. (2018). An investigation of categorical variable encoding techniques in machine learning: Binary versus one-hot and feature hashing. KTH, School of Electrical Engineering and Computer Science. https://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1259073&dswid=214.
[59] Bagui, S., Nandi, D., Bagui, S., White, R.J. (2021). Machine learning and deep learning for phishing email classification using one-hot encoding. Journal of Computer Science, 17(7): 610-623. https://doi.org/10.3844/jcssp.2021.610.623
[60] Zhou, J., Gandomi, A.H., Chen, F., Holzinger, A. (2021). Evaluating the quality of machine learning explanations: A survey on methods and metrics. Electronics, 10(5): 593. https://doi.org/10.3390/ electronics10050593