Sarah Riyadh Adnan![]() | Aqeel Majeed Breesam*
| Aqeel Majeed Breesam*![]() | Alaa Hussein Abdulaal
| Alaa Hussein Abdulaal![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Alzheimer's disease functions as the leading dementia disorder and creates a major health problem for millions of patients worldwide. Effective preventive intervention requires AD detection during the Mild Cognitive Impairment stage. The study employs VGG16 together with MobileNet architectures to classify Alzheimer's disease through MRI image analysis. The adoption of transfer learning for pre-trained models allowed us to modify MobileNet using the Snake Optimization Algorithm (SOA) for superior performance outcomes. Accurate AD classification through deep learning technology depends on transfer learning combined with hyperparameter optimization mechanisms, which process image datasets as input. When the MobileNet model operated with the SOA optimizer, the system reached a 97.71% accuracy, outperforming the results obtained from the VGG16 model. Our optimized model achieved superior performance across all other metrics with both high precision and recall rates in addition to reaching a 97.71% accuracy in AD stage diagnosis. The MobileNet+SOA algorithm exhibits higher precision and accuracy rates than its counterparts for MRI image diagnosis, as shown by comparative performance evaluation. The combination of deep learning methods, transfer learning and hyperparameter optimization produces an efficient solution for MRI image-based Alzheimer's disease classification. The MobileNet+SOA model shows promise as an advanced AI-based AD diagnosis system that can help detect AD at an earlier stage to better manage this damaging neurological disease.
MRI-based AD diagnosis, deep learning, metaheuristic optimization, Snake Optimization Algorithm (SOA), transfer learning, MobileNet
Alzheimer's disease (AD) is the most common form of dementia, impacting millions worldwide. Despite extensive research, no treatment has been identified to halt or reverse its progression [1]. Early-stage Alzheimer's disease classification from neuroimaging data provides considerable challenges due to subtle brain changes, high data dimensionality, and heterogeneous disease presentations. Conventional machine learning methods with manually generated parameters usually exhibit low accuracy in distinguishing early-stage Alzheimer's disease from moderate cognitive impairment (MCI) and normal aging.
In 2020, approximately 6 million Americans had Alzheimer's disease, with the figure predicted to rise to 14 million by mid-century [2]. Early AD diagnosis is crucial since it allows for treatment before full clinical symptoms appear. MCI, which affects 20% of seniors over the age of 65, is a stepping stone between normal aging and Alzheimer's disease, with 35% progressing to the latter within three to five years [2, 3]. An autopsy remains the most definitive approach to make an Alzheimer's diagnosis [4].
With healthcare costs projected to exceed USD 1.1 trillion by 2050 [2] and USD 305 billion in 2020, AD has a substantial financial impact. These alarming figures demonstrate how urgently improved diagnostic tools are required. Thus, the purpose of this study is to halt the progression of Alzheimer's disease by creating advanced computational tools for early detection.
To detect Alzheimer's disease in its early stages, decision making algorithms capable of distinguishing between AD, MCI, and normal cognitive function are required. Traditional classification approaches are severely limited due to challenges such as overfitting from tiny MRI datasets and the significant amount of human feature engineering required [5]. Furthermore, standard diagnostic procedures make it difficult to distinguish the fine-grained transition borders between AD and MCI.
When contemporary neuroimaging and machine learning (ML) are combined, the diagnosis of Alzheimer's disease looks promising. Contests like the AD large data challenge [6] and the MCI prediction challenges [7] have demonstrated the efficacy of machine learning techniques. However, the robustness and reproducibility of these methods can yet be improved [8, 9].
Deep learning (DL), a type of machine learning (ML), has grown in popularity for medical imaging jobs due to its ability to extract complex data without human interaction [10]. DL approaches are great at integrating data from multiple brain regions, learning representations that are invisible to the human eye, and detecting hidden patterns in MRI scans. When compared to alternative imaging techniques, convolutional neural networks (CNNs) have been demonstrated to be more effective in Alzheimer's disease classification tasks than conventional approaches.
The performance of DL models is heavily influenced by hyperparameter tweaking. The Snake Optimization Algorithm (SOA), which is inspired by biological snake motions, provides a viable way for automatically modifying hyperparameters to improve classification accuracy without requiring a lot of manual labor.
Transfer learning (TL), particularly for small datasets, has emerged as a powerful strategy for improving deep learning models [11, 12]. TL improves generalization and accelerates convergence by leveraging knowledge from related fields. TL-based approaches are particularly effective at distinguishing between progressive MCI (pMCI) and stable MCI (sMCI) [13, 14].
This research uses deep learning architectures VGG16 and MobileNet and transfer learning and optimizes hyperparameters by applying the SOA to specifically address AD classification problems. Our method will eliminate current technique restrictions by leveraging deep learning model feature extraction abilities to optimize their performance for AD classification from MRI images. We integrate advanced computational techniques to build a better diagnostic method for detecting AD in early stages and its subsequent management.
Deep learning and machine learning-based approaches for Alzheimer's disease diagnosis have lately received substantial attention in computer vision and medical imaging research. To do this, machine learning algorithms that use image or voxel intensity, tissue density, and form as feature input test classifiers can discriminate between AD patients with MCI and cognitively normal (CN) people.
A new deep learning technique for identifying AD compared to a healthy control was presented by Sarraf et al. [15]. The study’s sample consisted of 15 healthy people serving as a control group and 28 AD patients who were gathered from the ongoing multicenter AD Neuroimaging Initiative. Skull stripping, motion correction, registration, denoising, and spatial smoothing with a full-width-at-half maximum value of 5 mm were all included in the preprocessing. Following preprocessing, the data was fed into the Le-Net model, yielding a 96.85% accuracy. A different research by Mathew et al. [16] used 158 MRI images (71 NC and 87 patients) in our dataset from Alzheimer’s disease dementia (ADD) to introduce the early diagnosis of AD. Preprocessing, which includes normalizing, resizing, deforming, and flipping for improved learning, is the last phase. Principal Component Analysis (PCA) and Discrete Wavelet Transform were used for feature extraction, while Support Vector Machine (SVM) was used for classification. We were able to get an accuracy of 84% for AD vs. CNs and 91% for MCI vs. CFs.
Simultaneously, Hosseini-Asl et al. [17] suggested the use of a deep three-dimensional convolution neural network, or 3D-CNN, for AD diagnosis. Using MRI data from 70 AD, MCI, and NC patients from the ADNI dataset, they tested their studies. Local features were extracted from the 3D input pictures using convolutional neural networks.
Convolutional autoencoder (CAE), a CAD-Dementia dataset of T1-weighted MRI scans of AD, CN, and NC individuals was used to train the model. Skull peeling and spatial normalization comprised preprocessing. Features from the CAD-Dementia dataset were used as biomarkers in the fine-tuning to identify AD in the ADNI dataset. A ten-fold cross-validation produced a classification accuracy of 97.6% when comparing AD with NC.
Ju et al. [18] created a deep neural network for an AD diagnostic task using MRI and textual data (age, gender, and genetic). Using MRI scans of 91 patients with mild cognitive impairment (MCI) and 79 normal controls, together with the matching genetic data from the ADNI-2 dataset, they assessed our proposed technique. They also looked into the relationships between ApoE genotype, age, sex, and MCI. Data Processing and Analysis for Brain Imaging (DPABI) was used for data preparation [19, 20].
In order to do this, they fed correlation coefficient data and Rf-MRI time-series data into LDR, LR, and SVM models (authors their findings indicated that incorporating correlation coefficient data increased test accuracy. The accuracy, sensitivity, and specificity of the LDR model were 65%, 66%, and 67.72%, respectively. Accuracy in the LR model was 71.38%, with a sensitivity of about 77% and specificity of about 62%. Its specificity is 64%, sensitivity of the model is 79%, and accuracy is 78.91%. With an accuracy of 86.47%, sensitivity of 92%, and specificity of 81%, as determined by correlation coefficient data, the autoencoder network demonstrated superior performance.
Deep learning models were used by Farooq et al. [21] for the multi-class categorization of AD. They divided the data into four classes using the ADNI dataset. These classes included 33, 22, 449, and 45 MRI images, respectively. While ResNet-18 and ResNet-152 attained accuracies of 98.01% and 98.14%, respectively, GoogLeNet yielded an accuracy of 98.88%.
A straightforward and effective method for identifying AD using brain MRIs and a three-dimensional convolutional neural network architecture (3D ConvNet) was reported by Bäckström et al. [22]. They extracted automatic features after completing preprocessing operations such as cortex reconstruction, edge clipping, picture resizing, and intensity normalization. The study made use of 1190 MRI images and 340 people from the ADNI dataset, which included 196 AD patients (of whom 103 were male and 96 were female) and 141 normal controls (of whom 75 were male and 66 were female). The model obtained an accuracy of 98.78%.
Gautam et al. [23] introduced a one-class classification (OCC) method that needs training data to come from only one class. By adding the lowest variance data to the OCC design, they improved the classifier’s capacity to generalize and decreased intra-class variation. Tests was done on eighteen reference datasets showed that the suggested technique beat previous methods by more than 5% in F1 score. The primary benefit of the one-class classifier is its efficacy in scenarios when there are either extremely few or no data samples available from other classes.
In the study conducted by Liu et al. [24], a framework consisting of two deep learning models was introduced. The first model is a multi-task deep CNN intended for AD classification and hippocampal segmentation. A binary segmentation mask of the hippocampal region is produced by this model. Nevertheless, it was discovered that the characteristics this multi-task model learnt were insufficient for precise AD classification. In order to make up for these shortcomings, 3D patch hippocampal characteristics were derived using the centroid as a guide. In order to train features for AD classification, the second model, a 3D-DenseNet, was used to differentiate between three classes for AD/NC classification, the suggested strategy outperformed the voxel-wise (86.1%) and area of interest (ROI) (84.7%) characteristics, achieving a classification accuracy of 88.9%.
Functional MRI (fMRI) data from the ADNI dataset was used by Kazemi and Houghten [25] to categorize the various phases of AD. They gathered information from 197 participants—107 women and 90 men—during five courses. With an average accuracy of 97.63%.
Tajbakhsh et al. [26] investigated which approach—training a CNN from scratch or using a fine-tuned CNN approach—is more successful for medical image analysis. They experimented with both approaches and found that, in terms of medical picture classification, detection, and seg- mentation, the optimized method on the ImageNet dataset performed better than training from scratch. Large labeled training datasets, which are sometimes hard to come by in the medical in- dustry, along with a great deal of experience, memory use, and processing power are all necessary for training a CNN from scratch. On the other hand, a CNN that had been trained beforehand using the ImageNet dataset yielded encouraging outcomes for a range of uses, such as the interpretation of medical images.
Ebrahimi-Ghahnavieh et al. [27] used transfer learning to identify AD from MRIs in the ADNI dataset. They performed MRI scan trials with 132 participants per group (AD; NC). They combined recurrent neural networks (RNN) with CNNs. Moreover, identifying improved sequence associations of input photos was the primary goal. After feeding the characteristics into one of our CNNs, we trained an RNN on top of it to increase accuracy.
Using MRI data, Wang et al. [28] presented a 3D CNN-based model using DenseNet. With better information and gradient propagation, these dense connections in the 3D-CNN minimized overfitting and made training easier by bridging the gap between feature extractions caused by the intrinsic lack of data. The authors combined base classifiers using a fusion approach to create an ensemble-based model with a 97.19% accuracy. Table 1 shows a comparison of related works to AD diagnosis.
Table 1. Comparison of related work on AD diagnosis
|
Ref. |
Method |
Dataset |
Accuracy (%) |
Advantages and Disadvantages |
|
[15] |
Le-Net |
ADNI |
96.85 |
High accuracy but limited to small sample sizes. |
|
[16] |
SVM and PCA |
ADD |
84 |
Effective for early diagnosis; Lower accuracy compared to deep learning models. |
|
[17] |
3D-CNN |
ADNI |
Not specified |
Extracts local features effectively; accuracy not specified. |
|
[18] |
Deep Neural Network |
ADNI-2 |
78.91 |
Incorporates genetic data, but moderate accuracy. |
|
[19, 20] |
Autoencoder |
CAD-dementia and ADNI |
97.6 |
High accuracy with cross-dataset validation; computationally intensive. |
|
[21] |
GoogLeNet, ResNet |
ADNI |
Up to 98.88 |
Very high accuracy; requires substantial computational resources. |
|
[22] |
3D ConvNet |
ADNI |
98.78 |
High accuracy; preprocessing may introduce data loss. |
|
[23] |
One-class Classifier |
Multiple datasets |
Not specified |
Good for limited data scenarios; may not generalize well across diverse datasets. |
|
[24] |
Multi-task CNN and 3D-DenseNet |
ADNI |
88.9 |
Good for AD/NC classification; initial features may be insufficient without further tuning. |
|
[25] |
fMRI analysis |
ADNI |
97.63 |
High accuracy; fMRI data may not be widely available. |
|
[26] |
CNN (Fine-tuning) |
ImageNet and medical images |
Varies |
Lower resource requirement than training from scratch; dependent on pre-trained model relevance. |
|
[27] |
RNN and CNN |
ADNI |
Not specified |
Aims to improve sequence learning; complexity may hinder practical application. |
|
[28] |
3D CNN with DenseNet |
ADNI |
97.19 |
Reduces overfitting with dense connections; complex model structure. |
Specific researchers have created a thorough deep learning system, which detects multiple stages of AD through magnetic resonance imaging neuroimaging data. Data acquisition and exploratory data analysis form the first steps of this methodology since they provide vital perspectives about both the input data's distribution and its quality. 3,714 T1-weighted MRI scans exist in the dataset, which are categorized as NonDemented, MildDemented and VeryDemented. All images underwent processing that included scaling them to 224 pixels by 224 pixels as well as RGB conversion for activation with pre-trained convolutional neural networks. During the EDA process experts examined the data sets while running statistical tests to find imbalanced classes alongside unique features. Normalization of pixel values followed by the application of horizontal flips and rotations occurred after data preprocessing. The categorical labels underwent one-hot encoding during this process. An 80/20 ratio was used for stratified partitioning, which let the model evaluate its performance in a standardized way.
The central mechanism adopts transfer learning with VGG16 and MobileNet, which were pre-trained on ImageNet images. Both models functioned as embedded feature extractions that received their initial classification layers replaced by newly created dense layers for processing AD stage categories. The trained networks had global average pooling layers which were followed by four serial fully connected layers consisting of nodes with decreasing numbers (1024, 512, 256, 128) with ReLU activation. A Softmax output layer with three neurons was added as the last component of the model structure for multi-class prediction. During training the researchers kept the first network layers frozen while focusing on developing the additional layers with AD dataset information. Models benefited from the integration of generalizable features acquired from broad-scale data, which they applied to AD-specific MRI scan characteristics. The training lasted for 10 epochs using 32 batch instances for prediction while the Adam optimizer and categorical cross-entropy defined the loss parameter.
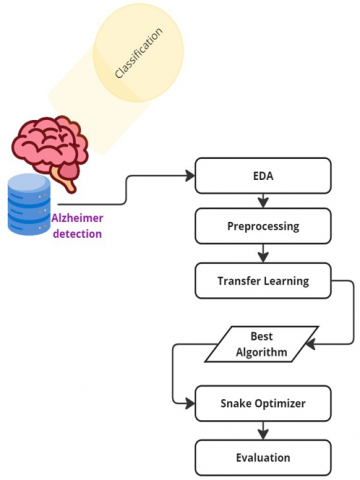
The model performance was strengthened through using the SOA to optimize learning rate and dropout rate, together with dense layer size. SOA functions as a nature-inspired algorithm that builds its operation off snake movement patterns, which adapt and use sinusoidal behavior in multidimensional search spaces. The evaluation of candidate hyperparameter sets through validation accuracy takes place in the SOA. The algorithm repeatedly adjusts the velocity and positioning of every snake following the global best solution influence through a sinusoidal exploration mechanism. The MobileNet model achieved better performance after retraining it with the most effective hyperparameters discovered through the PSO algorithm. Figure 1 illustrates the proposed work.
Figure 1. Proposed scheme
The evaluation metrics involved accuracy, precision, recall and F1-score computation where the results were macro-averaged across all three classes to achieve balanced measurement of performance. The enhanced deep learning framework proves its ability to identify and classify early-stage AD right after optimization.
A Python-based approach adopted TensorFlow together with Keras frameworks for developing the model. The dataset was divided into an 80-20 split of training and testing sections and it contained an extra validation group obtained from the training data. The research experiments operated from a GPU-based system platform. The assessment utilized accuracy together with precision and recall and F1-score metrics that performed an average calculation across all classes to maintain balance during evaluation of data sets with unbalanced classes.
3.1 Dataset overview
Our research used an open-access MRI neuroimaging database, which was developed for classifying AD. The database features 3714 T1-weighted magnetic resonance imaging (MRI) scans that received classification labels based on three clinical diagnostic categories, which describe cognitive decline development stages from NonDemented, MildDemented and VeryDemented. The classified dataset utilizes definitive AD diagnostic stages, so it produces a meaningful multi-class classification system similar to the medical diagnostic procedures faced by clinicians.
The imaging data originated from established repositories for medical images before the images underwent a preparatory step, which included both skull-stripping operations and intensity normalization tasks. All images received pre-processing treatment by being resized to 224 × 224 pixels and being converted to RGB color mode even though they originated as grayscale scans. Before inputting the images to VGG16 and MobileNet networks we performed this conversion because both networks need three-channel images as their source data.
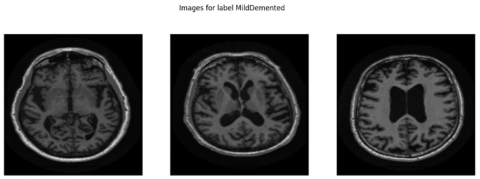
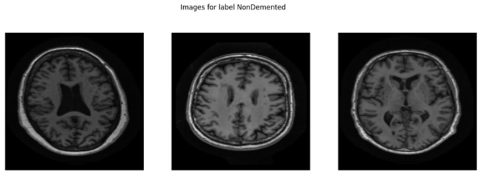
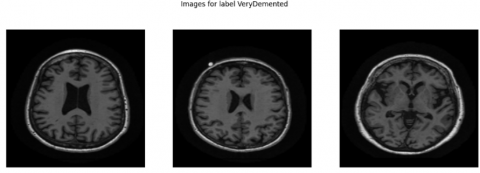
The structural parameters of this dataset show mild bias since it contains 1,216 NonDemented scans while MildDemented scans reach 1,792 images and VeryDemented scans total 706 images. The research data shows good clinical accuracy because healthcare professionals routinely examine more patients with MildDemented conditions. This visual representation in Figure 2 shows MRI cutting planes from each class to represent their structural and intensity differences. The anatomical differences between samples in cognitive processing centers become noticeable in these examples which supports accurate model functioning during training and inference. The varied content of this database enables deep learning models to become effective while they demonstrate multispectral capabilities for AD detection at an early stage.
Figure 2. Sample MRI images from different classes
3.2 EDA and preprocessing
A proper Exploratory Data Analysis (EDA) was performed in advance to uncover the structural features alongside visual elements and distribution imbalances throughout the dataset. The underlying database consists of 3,714 T1-weighted brain MRI images containing clinical labels of NonDemented, MildDemented and VeryDemented cognitive stage classifications. The three stages of AD organize into separate categories which the labels represent. The main goal of Exploratory Data Analysis included two objectives: first displaying representative images from each class category as shown in Figure 2 and second applying analysis techniques to examine statistical properties which would guide further preprocessing steps and model development.
EDA began with investigating the class label distribution which showed a moderate imbalance with 1,216 NonDemented images and 1,792 MildDemented images and 706 VeryDemented images. Without balancing the data distribution, the model would lean toward classifying instances primarily as MildDemented because this category represents the largest population. As a result, it would be harder to detect cases of both early and advanced dementia. To address the problem of unequal minority classes, data augmentation was developed. According to EDA findings, pixel intensity histograms revealed discernible differences in brightness and contrast levels between images from different classes. The evaluation demonstrated the importance of intensity normalization in maintaining continuous contrast levels that maximize the performance of neural network training.
EDA included qualitative anatomical examinations in several classes as a supplement to histogram analysis. The charting of typical sections images revealed distinct differences in brain structures, particularly at the medial temporal lobe and ventricular areas, which are associated with AD progression. The investigation confirmed that spatial relationships and image textures must be consistently maintained during preprocessing techniques. The team used suitable resizing processes to create standardized images with 224 × 224 pixel dimensions in RGB format, rather than using harsh compression techniques. To suit the needs of pre-trained convolutional networks like VGG16 and MobileNet, which prefer RGB inputs, MRI pictures need to be transformed into three RGB channels.
The research findings guided a systematic approach to developing the preprocessing system for deep learning-based classification. The core steps included:
$y_i=\left\{\begin{array}{c}1 \text {, if class } i \text { corresponds to the given label } \\ 0, \quad \text { otherwise }\end{array}\right.$
The model received augmented data through random horizontal flips and small-angle rotations extending from ±10° plus zoom adjustments and brightness transformations that strengthened training capacity while addressing class unbalance issues. The preprocessing techniques obtained their direction from EDA outcomes and established critical components for creating unbiased and sturdy models.
Through the EDA process researchers gained essential data knowledge while developing essential preprocessing methods for their operation. The standardized integrated strategy allowed our input data to prepare effectively for training deep learning models dedicated to AD classification.
3.3 Transfer learning
In this section, we discuss the major area of AD classification using transfer learning. Pre-training a model simply means that we will train our own custom dataset with some pre-opened models to perform really well on tasks of another new type, from all the past collections trained already. This substantially reduces the effort of training models in similar tasks and improves overall accuracy using previously learned features from a related domain.
We used two different pre-trained models: VGG16 and MobileNet on the classification of AD. They were pre-trained on large image datasets and are popular for different tasks of generalized image recognition.
VGG16 is one of those deep Convolutional Neural Networks that has been used a lot in image classification challenge. It contains several convolutional layers, which act as filters to learn important features from the input images. In our implementation, given the pre-trained VGG16 without top layers for ImageNet classification (implemented by Keras). We did not replace the feature extractor with another CNN architecture but rather used custom fully connected layers to re-purpose it for AD classification. These layers allow the model to learn features particular to this problem making it more capable of distinguishing between different levels of dementia.
In the experiments, another deep learning model called MobileNet was also used because of its lightweight architecture which makes it more suitable to run in resource-constrained environments. MobileNets uses depthwise separable convolutions to reduce the number of parameters the net is modified in such a way that reduces a huge number of parameter and retains same accuracy. Similar to the VGG16, we replaced the top layers with our custom intermediate layers on MobileNet.
In both configurations, we retained the initial layers frozen during training rest of the model using Generative Adversarial Networks to force and constrain PCA transformation from base inputs. These custom layers were trained on the AD dataset to recognize certain patterns differentiating between stages of dementia.
In the post training phase, performance evaluation on accuracy, precision or recall and similar metrics for both the models are performed. We compared the outcomes of these models to establish an optimal method for AD classification by 6.
Transfer learning has been applied in this context and is shown to be effective using pre-trained models, which can achieve state of the art results with minimal training data. This makes it an important tool for medical image analysis. We are going to report the results for each model and explore what they mean in terms of detecting AD.
The rationale for selecting VGG16 and MobileNet stems from their complementary characteristics. VGG16, with its deep architecture and proven success in medical imaging tasks, provides a strong baseline for feature extraction, while MobileNet's lightweight design makes it more suitable for real-time applications where computational resources are limited. Additionally, to validate the effectiveness of our optimizer choice, we conducted comparative experiments where the SOA was evaluated against traditional optimizers such as Adam and SGD. Table 2 presents the model's parameters and values.
Table 2. Model parameters and values
|
Parameter |
VGG16 |
MobileNet |
|
Pre-trained Weights |
ImageNet |
ImageNet |
|
Input Size |
224 × 224 × 3 |
224 × 224 × 3 |
|
Global Average Pooling |
Yes |
Yes |
|
Dense Layer 1 Units |
1024 |
1024 |
|
Dense Layer 2 Units |
512 |
512 |
|
Dense Layer 3 Units |
128 |
256 |
|
Dense Layer 4 Units |
64 |
128 |
|
Activation Function |
ReLU |
ReLU |
|
Output Layer Activation |
Softmax |
Softmax |
|
Optimizer |
Adam |
Adam |
|
Loss Function |
Categorical Crossentropy |
Categorical Crossentropy |
|
Batch Size |
32 |
32 |
|
Epochs |
10 |
10 |
|
Trainable Layers |
Custom Dense Layers |
Custom Dense Layers |
3.4 Snake optimizer
In this study we applied SOA as a hyperparameter optimization strategy for improving performance in the MobileNet architecture for multi-class AD classification. SOA serves as a new biological metaheuristic that uses snake network behavior to discover solutions within complex search spaces which adapt their bodies while remaining aware of environmental conditions. This design suits deep learning model optimization because it helps experts find perfect generalization performances through several dependent hyperparameter adjustments.
All snakes in the population serve as potential solutions because each contains one distinct hyperparameter configuration for the MobileNet model. The algorithm launches its operation by randomly placing snakes across the hyperparameter space where every position represents individual sets of hyperparameters values. Each snake element in the population receives its unique initial velocity direction, which allows it to shift through the search territory. The MobileNet model receives its present set of hyperparameters from each snake in order to conduct training operations during each sequence. The model uses validation accuracy to evaluate the solutions, which have been assessed for fitness.
Snakes who reach the best validation accuracy when tested become the global best solution after which all other snakes adjust their movements based on this position. The software implements position and velocity updating procedures that follow these rules:
velocityi = velocityi + (best position − positioni) × learning factor (1)
positioni = positioni + velocityi + sin(iteration) × sinusoidal factor (2)
Here, velocityi represents the velocity of snake i, positioni denotes the current position of snake i in the hyperparameter space, and best_position is the position of the best-performing snake.
The learning factor is the weighting of how much a snake’s speed gets adapted by moving towards to top snakes position, and the sinusoidal factor puts some periodic behavior into how we update our position.
Finally, an optimal set of hyperparameters is obtained as the snake with the highest fitness after a predefined number optimization cycles. These hyperparameters are then put to use for fine tuning of the deep learning model which boosts its performance. The best model then goes through more advanced physical and mathematical testing using an independent test set of data to give functionality in terms of accuracy, precision also recalls.
In our implementation, the SOA was specifically used to optimize the following hyperparameters of the MobileNet model:
The results obtained with the optimized model show better classification result which proved its prowess regarding to performance SOA.
To sum up, the optimal algorithm for hyperparameter optimization of deep learning is reliable to get higher accuracy with better generalization. This use case of the algorithm for Alzheimer classification highlights its ability to improve complex models having many hyperparameters.
|
Algorithm 1. SOA |
|
1: Input: Population size n, number of iterations T, learning factor α, sinusoidal factor β 2: Output: Best hyperparameters best_position 3: Initialize population of n snakes, each with random positions and velocities 4: Evaluate fitness of each snake based on validation accuracy of the model 5: Identify the best snake best_snake with highest fitness 6: for iteration = 1 to T do 7: for each snake i in the population do 8: Update velocity: velocityi = velocityi + α × (best_position − positioni) 9: Update position: positioni = positioni + velocityi + β × sin(iteration) 10: Evaluate new fitness of snake i 11: if new fitness of snake i is better than best fitness then 12: Update best_snake and best_position 13: end if 14: end for 15: end for 16: Return: best_position as the optimal hyperparameters |
3.5 Evaluation metrics
One of key ingredients in evaluation (I also talked a bit on this), is metrics, as importance comes attached with its critical role especially for medical imaging domain where everything revolves around life and death. Metrics: Common metrics used in the diagnosis of AD through machine learning approaches are Accuracy, Precision Recall and F1-Score. These metrics are used to generate understanding of the model performance at different angles such as overall correctness, ability to detect positive cases and trade-off between precision recall [29].
$Accuracy =\frac{T N+T P}{T P+T N+F P+F N}$ (3)
$Precision=\frac{T P}{F P+T P}$ (4)
$Recall=\frac{T P}{T P+F N}$ (5)
$F 1- Score =2 \times \frac{P R E \times R E C}{P R E+R E C}$ (6)
The study assessed deep learning models VGG16 and MobileNet when used for multiple AD class identification through MRI image analysis. Moreover, the results distinguish between the performance strength of VGG16 and MobileNet models with and without utilization of SOA. Medical imaging results require evaluation through accuracy, precision, recall and F1-score measurements because wrong positives and wrong negatives produce critical outcomes in this field.
The VGG16 model delivered 91.39% accuracy in its operations as shown in Table 3. According to the detailed classification report the precision score for Mild Demented cases reached 0.95 while the recall metric reached 0.91 and F1-score existed at 0.93. The NonDemented category obtained values measuring 0.95 for precision and 0.91 for F1-score and 0.88 for recall. The VeryDemented class exhibited lower model efficiency reflected through 0.82 precision and 0.96 recall and an F1-score of 0.88. VGG16 demonstrates excellent performance detecting VeryDemented cases yet generates numerous wrong positive diagnoses shown by its poor precision value. The model demonstrates weak performance stability across different groups of subjects.
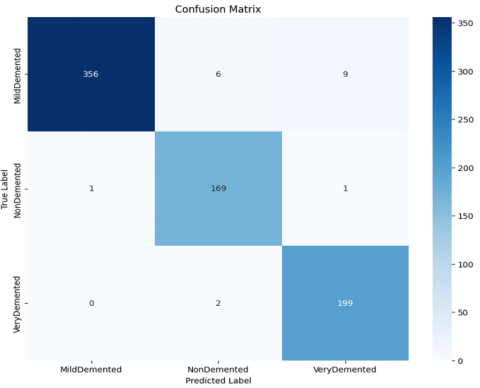
MobileNet demonstrated superior performance than VGG16 according to all measurement criteria where it achieved a total accuracy score of 96.50% as shown in Table 3. The MildDemented category achieved an F1-score of 0.97 together with a precision level of 0.99 and recall measurement of 0.95. The detection metrics for NonDemented equaled 0.93, 0.99, and 0.96 and VeryDemented metrics showed 0.95, 0.96, and 0.95. The confusion matrix in Table 4 demonstrates the model's excellent reliability by properly identifying 355 cases of MildDemented along with 176 instances of NonDemented and 186 VeryDemented cases among the total 743 instances. MobileNet achieved superior class distribution together with enhanced generalization capabilities by reducing the number of wrong negative outcomes and incorrect positive predictions. The model achieves good performance due to its lightweight structure and efficient depthwise separable convolutions that eliminate parameter redundancies and enhance prediction generalization capabilities.
Table 3. Summary of experiment results
|
Model |
Accuracy (%) |
Precision |
Recall |
F1-Score |
|
VGG16 |
91.39 |
0.91 |
0.92 |
0.91 |
|
MobileNet |
96.50 |
0.96 |
0.97 |
0.96 |
|
MobileNet + Snake optimizer |
97.71 |
0.97 |
0.98 |
0.98 |
Table 4. Comparison of accuracy between related work and proposed work
|
Ref. |
Method |
Dataset |
Accuracy (%) |
|
[16] |
SVM |
ADD |
84 |
|
[17] |
3D-CNN |
ADNI |
Not specified |
|
[18] |
Deep neural network |
ADNI-2 |
78.91 |
|
Proposed Work |
MobileNet + Snake Optimizer |
ADNI |
97.71 |
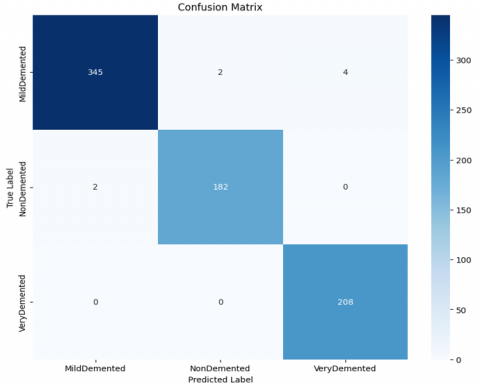
MobileNet achieved a 97.71% accuracy level after the SOA implementation as shown in Table 3. The assessment metrics for MildDemented category showed precision at 0.99 and recall at 0.97 along with an F1-score of 0.98. The accuracy scores for NonDemented amounted to 0.92, 0.99, 0.95 while VeryDemented achieved a perfect or near-perfect accuracy of 1.00, 0.99, 1.00.
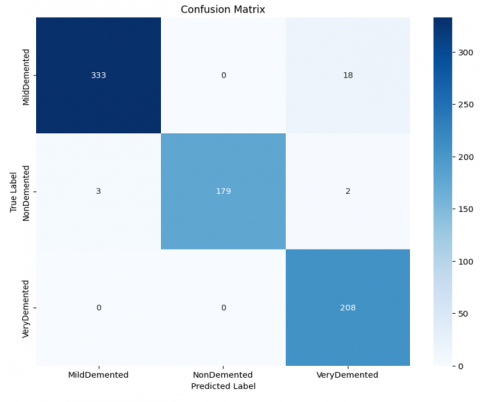
The evaluation of the proposed models was conducted through the analysis of confusion matrices, which provide a comprehensive overview of classification performance across different AD stages. Figure 3 presents the confusion matrix for the VGG16 model, where a moderate number of misclassifications is observed, particularly between MildDemented and VeryDemented categories. Figure 4 shows the confusion matrix for the MobileNet model, which demonstrates improved classification performance compared to VGG16, with fewer misclassified instances and a clearer distinction between classes. Finally, Figure 5 illustrates the confusion matrix for the hybrid model combining MobileNet with Snake algorithms. This hybrid model exhibits the most balanced and accurate classification performance, with near-perfect separation between the MildDemented, NonDemented, and VeryDemented classes. The significant reduction in misclassifications highlights the effectiveness of the proposed hybrid optimization approach in enhancing AD stage prediction accuracy.
Figure 3. Confusion matrix of the VGG16 model for Alzheimer's disease stage classification
Figure 4. Confusion matrix of the MobileNet model for Alzheimer's disease stage classification
Figure 5. Confusion matrix of the hybrid MobileNet model optimized with Snake algorithms for AD stage classification
The SOA improved critical parameters including learning rate alongside dropout by which the system achieved enhanced performance during convergence and robust operation.
The extensive outcome from these studies establishes MobileNet as a powerful solution which is strengthened through SOA optimization. Harsh limitations from VGG16 occurred due to its weighty structure while performing tasks with limited datasets. MobileNet's efficient structure contributed with SOA parameter optimization to achieve superior balanced performance results throughout all AD categories.
A comparison of the proposed method with multiple approaches for AD classification is shown in Table 4. The table features findings from important literature studies that present information about different approaches including their implemented models and datasets coupled with reported accuracy rates. The ADD dataset was analyzed by Authors using Support Vector Machine (SVM) which produced 84% accuracy and another approach by Ju et al. [18] introduced deep neural networks with ADNI-2 data achieving 78.91% accuracy. Hosseini-Asl et al. [17] used a 3D-CNN architecture on the ADNI dataset but neglected to provide accuracy results.
We obtained a substantially improved accuracy level of 97.71% using the MobileNet algorithm optimized through SOA on the ADNI dataset. The reinforcement of performance through our method demonstrates both qualitative and theoretical importance. Our proposed framework combines transfer learning features with SOA for metaheuristic optimization, which improves both generalization and classification outcomes by fine-tuning hyperparameters in traditional machine learning and deep learning modeling approaches.
The results support the superiority and resilience of our proposed technique. SOA adoption improves performance by identifying superior configurations that would otherwise go undiscovered through ordinary manual tuning or grid search operations. MobileNet's robust architectural features allow it to provide both computing speed and accuracy while remaining lightweight. The implementation is particularly important for clinical practice since it combines precision and scalability requirements. The data in Table 4 confirms both the numerical benefits and the essential contributions to cutting-edge strategies for rapid and precise AD diagnosis.
The study developed and validated a new deep learning technique for multi-class AD identification using T1-weighted MRI neuroimaging data. The fundamental value of this project stems from the combination of MobileNet architecture with SOA for autonomous hyperparameter modification. The suggested system achieved a classification accuracy of 97.71% using ImageNet transfer learning, optimal learning rate and dropout rate settings, and dense layer parameter configuration changes. The synergistic effect of combining MobileNet with physiologically motivated optimization resulted in higher performance results over VGG16.
The MobileNet + SOA model displayed high precision while maintaining superior recall and F1-scores for the NonDemented, MildDemented, and VeryDemented depression phases, demonstrating its capacity to detect both simple and advanced levels of cognitive decline. The confusion matrices verified the classification method's consistent conclusions by demonstrating low misclassification errors and uniform sensitivity values across classes. Early detection of mild cognitive impairment using this model is critical for clinical practice because it enables healthcare practitioners to identify appropriate interventions to prevent disease progression while enhancing patient quality of life.
This framework demonstrates how deep learning combined with metaheuristic optimization can result in successful diagnostic tools that scale effectively and intelligently. MobileNet deployment allows for real-time applications in constrained medical contexts because this low-cost computational approach is efficient. Solid ware optimization as a service system provides researchers with a standardized approach to optimizing deep learning models via automatic configuration tweaks, resulting in improved repeatability across test datasets.
Further research can be initiated through the findings presented in this study. The framework should benefit from incorporating PET imaging data including cerebrospinal fluid biomarkers and genetic markers as this addition would supply supplementary information that increases diagnostic accuracy. Further research should apply this methodology to Parkinson’s Disease or Huntington’s Disease to determine its application range across different neurodegenerative conditions as well as clinical implications. The system's clinical adoption potential will improve through explainable methods (Grad-CAM or SHAP) which reveal interpretable model decisions to the clinicians.
The research demonstrates how MobileNet + SOA-based framework improves Alzheimer’s Disease diagnosis by achieving high accuracy levels. The model provides promising potential for deployment in intelligent healthcare systems because it shows high performance rates and operational efficiency and adaptability in neurodegenerative disorder examination and therapy planning.
[1] Hardy, J. (1997). Amyloid, the presenilins and Alzheimer's disease. Trends in Neurosciences, 20(4): 154-159. https://doi.org/10.1016/S0166-2236(96)01030-2
[2] Alzheimer's Association. (2021). Facts and Figures. Alzheimer’s Disease and Dementia. https://www.alz.org/alzheimers-dementia/facts-figures, accessed on 16 January 2021.
[3] Jicha, G.A., Parisi, J.E., Dickson, D.W., Johnson, K., et al. (2006). Neuropathologic outcome of mild cognitive impairment following progression to clinical dementia. Archives of Neurology, 63(5): 674-681. https://doi.org/10.1001/archneur.63.5.674
[4] Klöppel, S., Stonnington, C.M., Chu, C., Draganski, B., Scahill, R.I., Rohrer, J.D., Fox, N.C., Jack, Jr, C.R., Ashburner, J., Frackowiak, R.S. (2008). Automatic classification of MR scans in Alzheimer's disease. Brain, 131(3): 681-689. https://doi.org/10.1093/brain/awm319
[5] Rathore, S., Habes, M., Iftikhar, M.A., Shacklett, A., Davatzikos, C. (2017). A review on neuroimaging-based classification studies and associated feature extraction methods for Alzheimer's disease and its prodromal stages. NeuroImage, 155: 530-548. https://doi.org/10.1016/j.neuroimage.2017.03.057
[6] Allen, G.I., Amoroso, N., Anghel, C., Balagurusamy, V., et al. (2016). Crowdsourced estimation of cognitive decline and resilience in Alzheimer's disease. Alzheimer's & Dementia, 12(6): 645-653. https://doi.org/10.1016/j.jalz.2016.02.006
[7] Sarica, A., Cerasa, A., Quattrone, A., Calhoun, V. (2016). A machine learning neuroimaging challenge for automated diagnosis of mild cognitive impairment. Journal of Neuroscience Methods. https://www.kaggle.com/c/mci-prediction, accessed on 18 Jan. 2021.
[8] LeCun, Y., Bengio, Y., Hinton, G. (2015). Deep learning. Nature, 521(7553): 436-444. https://doi.org/10.1038/nature14539
[9] Samper-González, J., Burgos, N., Bottani, S., Fontanella, S., et al. (2018). Reproducible evaluation of classification methods in Alzheimer's disease: Framework and application to MRI and PET data. NeuroImage, 183: 504-521. https://doi.org/10.1016/j.neuroimage.2018.08.042
[10] Ali, S.M., Abbosh, Y.M., Breesam, A.M., Ali, D.M., Alhummada, I.A. (2024). Heart diseases classification through deep learning techniques: A review. AIP Conference Proceedings, 3232: 020022. https://doi.org/10.1063/5.0236126
[11] Mesnil, G., Dauphin, Y., Glorot, X., Rifai, S., Bengio, Y., Goodfellow, I., Lavoie, E., Muller, X., Desjardins, G., Warde-Farley, D., Vincent, P., Courville, A., Bergstra, J. (2012). Unsupervised and transfer learning challenge: A deep learning approach. In Proceedings of the 2011 International Conference on Unsupervised and Transfer Learning workshop, Washington, USA, pp. 97-111.
[12] Raina, R., Ng, A.Y., Koller, D. (2006). Constructing informative priors using transfer learning. In Proceedings of the 23rd International Conference on Machine Learning, New York, United States, pp. 713-720. https://doi.org/10.1145/1143844.1143934
[13] Zhou, L., Wang, Y., Li, Y., Yap, P. T., Shen, D., Alzheimer's Disease Neuroimaging Initiative (ADNI). (2011). Hierarchical anatomical brain networks for MCI prediction: Revisiting volumetric measures. PloS One, 6(7): e21935. https://doi.org/10.1371/journal.pone.0021935
[14] Ker, J., Wang, L., Rao, J., Lim, T. (2017). Deep learning applications in medical image analysis. IEEE Access, 6: 9375-9389. https://doi.org/10.1109/ACCESS.2017.2788044
[15] Sarraf, S., DeSouza, D. D., Anderson, J., Tofighi, G. (2016). DeepAD: Alzheimer’s disease classification via deep convolutional neural networks using MRI and fMRI. BioRxiv, 070441. https://doi.org/10.1101/070441
[16] Mathew, J., Mekkayil, L., Ramasangu, H., Karthikeyan, B.R., Manjunath, A.G. (2016). Robust algorithm for early detection of Alzheimer's disease using multiple feature extractions. In 2016 IEEE Annual India Conference (INDICON), Bangalore, India, pp. 1-6. https://doi.org/10.1109/INDICON.2016.7839026
[17] Hosseini-Asl, E., Keynton, R., El-Baz, A. (2016). Alzheimer's disease diagnostics by adaptation of 3D convolutional network. In 2016 IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, pp. 126-130. https://doi.org/10.1109/ICIP.2016.7532332
[18] Ju, R., Hu, C., Li, Q. (2017). Early diagnosis of Alzheimer's disease based on resting-state brain networks and deep learning. IEEE/ACM Transactions on Computational Biology and Bioinformatics, 16(1): 244-257. https://doi.org/10.1109/TCBB.2017.2776910
[19] Razzak, M.I., Imran, M., Xu, G. (2018). Efficient brain tumor segmentation with multiscale two-pathway-group conventional neural networks. IEEE Journal of Biomedical and Health Informatics, 23(5): 1911-1919. https://doi.org/10.1109/JBHI.2018.2874033
[20] Razzak, M.I., Naz, S., Zaib, A. (2018). Deep learning for medical image processing: Overview, challenges and the future. In Classification in BioApps. Lecture Notes in Computational Vision and Biomechanics. https://doi.org/10.1007/978-3-319-65981-7_12
[21] Farooq, A., Anwar, S., Awais, M., Rehman, S. (2017). A deep CNN based multi-class classification of Alzheimer's disease using MRI. In 2017 IEEE International Conference on Imaging systems and techniques (IST), Beijing, China, pp. 1-6. https://doi.org/10.1109/IST.2017.8261460
[22] Bäckström, K., Nazari, M., Gu, I.Y.H., Jakola, A.S. (2018). An efficient 3D deep convolutional network for Alzheimer's disease diagnosis using MR images. In 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, pp. 149-153. https://doi.org/10.1109/ISBI.2018.8363543
[23] Gautam, C., Mishra, P.K., Tiwari, A., Richhariya, B., Pandey, H.M., Wang, S., Tanveer, M., Alzheimer’s Disease Neuroimaging Initiative. (2020). Minimum variance-embedded deep kernel regularized least squares method for one-class classification and its applications to biomedical data. Neural Networks, 123: 191-216. https://doi.org/10.1016/j.neunet.2019.12.001
[24] Liu, M., Li, F., Yan, H., Wang, K., Ma, Y., Shen, L., Xu, M., Alzheimer’s Disease Neuroimaging Initiative. (2020). A multi-model deep convolutional neural network for automatic hippocampus segmentation and classification in Alzheimer’s disease. Neuroimage, 208: 116459. https://doi.org/10.1016/j.neuroimage.2019.116459
[25] Kazemi, Y., Houghten, S. (2018). A deep learning pipeline to classify different stages of Alzheimer's disease from fMRI data. In 2018 IEEE Conference on Computational Intelligence in Bioinformatics and Computational Biology (CIBCB), St. Louis, MO, USA, pp. 1-8. https://doi.org/10.1109/CIBCB.2018.8404980
[26] Tajbakhsh, N., Shin, J.Y., Gurudu, S.R., Hurst, R.T., Kendall, C.B., Gotway, M.B., Liang, J. (2016). Convolutional neural networks for medical image analysis: Full training or fine tuning? IEEE Transactions on Medical Imaging, 35(5): 1299-1312. https://doi.org/10.1109/TMI.2016.2535302
[27] Ebrahimi-Ghahnavieh, A., Luo, S., Chiong, R. (2019). Transfer learning for Alzheimer's disease detection on MRI images. In 2019 IEEE International Conference on Industry 4.0, Artificial Intelligence, and Communications Technology (IAICT), Bali, Indonesia, pp. 133-138. https://doi.org/10.1109/ICIAICT.2019.8784845
[28] Wang, S., Wang, H., Shen, Y., Wang, X. (2018). Automatic recognition of mild cognitive impairment and alzheimers disease using ensemble based 3d densely connected convolutional networks. In 2018 17th IEEE International Conference on Machine Learning and Applications (ICMLA), Orlando, FL, USA, pp. 517-523. https://doi.org/10.1109/ICMLA.2018.00083
[29] Najjar, E., Alkhaykanee, N.A., Breesam, A.M. (2025). Classification of Arabic documents with five classifier models using machine learning. International Journal on Informatics Visualization, 9(1): 365-370. https://doi.org/10.62527/joiv.9.1.2539