Rutuja Kande![]() | Minal Chhatre
| Minal Chhatre![]() | Radhika Bhagwat*
| Radhika Bhagwat*![]() | Kritika Dubey
| Kritika Dubey![]() | Gauri Joshi
| Gauri Joshi![]() | Priyanka Paygude
| Priyanka Paygude![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Among cancers, breast cancer continues to be a leading cause of mortality. Early detection is crucial for improving the chances of remission, but interpreting medical imaging, such as mammograms and ultrasounds, remains challenging due to factors like tissue density and human error. Artificial intelligence (AI), particularly machine learning (ML) and deep learning (DL), holds the potential to refine the accuracy of diagnoses. This study implements and compares the performance of nine classic ML algorithms (Random Forest, XGBoost, LightGBM, Support Vector Machine (SVM), AdaBoost, K-Nearest Neighbors (KNN), Naïve Bayes, Logistic Regression, and Decision Tree) and pre-trained Convolutional Neural Networks (CNNs), specifically ResNet50, DenseNet121, InceptionV3, EfficientNetB0, and VGG19, customized for this application along with CNN’s trained from scratch for ultrasound and mammogram images with accuracy 86% and 97% respectively. These models were assessed using accuracy, precision, recall, and F1-score as performance metrics, with the deep learning models showing significant improvement over the traditional ML models. The study used three datasets for breast cancer detection: CBIS-DDSM (mammograms), MIAS (mammograms), and a breast ultrasound dataset. The results give a deep analysis of model performance, offering an analysis of the advantages and limitations of each method throughout the datasets. The major contribution of this study paper lies its coverage of performance of both ML and DL models on multiple datasets covering different types of scans (ultrasound and mammogram) along with a density-based implementation of models to address challenges due to breast tissue density. This paper aims to identify the best-performing models and explore factors influencing their efficacy in clinical applications, contributing to the future of AI-driven breast cancer diagnostics.
artificial intelligence (AI), machine learning (ML), breast cancer, deep learning (DL), Convolutional Neural Networks (CNNs)
Breast cancer is the most prevalent and deadly cancer among women, despite the abundance of research done on it. In 2022 alone, over 2 million cases of this fast-spreading, deadly cancer were detected, with over 600,000 of them resulting in death. While there are a multitude of risk factors contributing to the development of cancer, including hereditary, hormonal, and lifestyle factors, it is estimated that nearly half the cases that occur have no traceable risk factors [1-5]. Due to this, early detection is critical in order to improve chances of remission.
The advances made in medical imaging, such as mammography and ultrasound, are pivotal to early diagnosis. But interpreting these images remains challenging due to a variety of factors, ranging from density of breast tissue to simple human error. Artificial Intelligence provides a possible solution for this. The application of machine learning (ML) and deep learning (DL) models has exhibited significant potential in improving detection of breast cancer.
This paper focuses on implementing and analyzing the performance of classic ML algorithms and DL models for detection of breast cancer using mammograms and ultrasound images. Each model was implemented on three distinct datasets, each offering unique characteristics, to ensure a thorough analysis of the models. A total of nine ML algorithms (Random Forest, XGBoost, KNN, LightGBM, SVM, AdaBoost, Naïve Bayes, Logistic Regression, and Decision Tree) and four deep learning architectures (InceptionV3, ResNet50, EfficientNetB0, and DenseNet121) were employed to cover a wide spectrum of approaches.
The key contribution of this paper resides in its comparative evaluation of these models across the datasets. By evaluating the robustness and shortcomings of each approach, this study focuses on providing understanding of their effectiveness for breast cancer detection and identifying the best-performing models. This study highlights the positive effect of preprocessing on fatty tissue mammogram images. It systematically compares traditional ML and CNNs across three different imaging datasets, in contrast to earlier efforts which are usually focused on a single dataset. It also highlights how transfer learning and data augmentation can improve the efficiency and generalization of models. Furthermore, we explore the underlying factors contributing to the observed performance differences and discuss their implications for clinical applications.
AI is becoming a crucial tool for physicians and radiologists in the identification of breast cancer since it improves speed and accuracy while lowering human error [6, 7]. By increasing precision, cutting down on pointless procedures, and assisting radiologists in classifying tumours as benign or malignant, artificial intelligence refines and optimizes the diagnosis of breast cancer [8, 9]. Research indicates that the diagnostic accuracy of AI plus pathologists is 99.5%, which is higher than that of AI (92%) and pathologists alone (96%). For gene expression and imaging analysis, models such as K-Nearest Neighbors (KNN) and Support Vector Machine (SVM), Recursive Feature Elimination (RFE) achieve 97.5% on WBCD [10-12]. AI models such as Discrete Wavelet Transform-based Markov Random Field (DWT-based MRF) improve the quality of mammograms, and multilayer perceptron (MLP) and KNN increase the identification of breast cancer, enabling a more accurate diagnosis in the early stages [13-15].
Breast cancer affected 2.23 million women and became the most malignant tumour in women [16], Since tumours under 10 mm have an 85% remission rate, early diagnosis is essential. However, many go unnoticed until they are over 20 mm. Early detection, accuracy, and speed of diagnosis are improved by machine learning and deep learning [17, 18]. Malignant tumours created by aberrant cell proliferation are the precursors of breast cancer. To stop the spread of cancer and increase the likelihood of remission, early detection is essential [19]. Understanding the hereditary, hormonal, environmental, and lifestyle factors driving breast cancer growth is crucial as research progresses [20].
Various researchers have extensively adopted deep learning methods, leading to exceptional accuracy scores [21]. Deep learning outperforms conventional techniques in medical imaging and pathology to improve breast cancer detection by increasing accuracy and facilitating early diagnosis [22, 23]. By analyzing medical pictures, increasing accessibility, decreasing expenses, and improving accuracy, CNNs have completely changed the detection of breast cancer. AI provides quicker, more accurate, and less expensive diagnoses despite obstacles [22, 23]. Accurate diagnosis, particularly in dense tissue, is made more difficult by deep learning in medical diagnostics due to issues including the requirement for sizable labelled datasets and the unpredictability of medical pictures [6, 13, 24]. Medical picture variability makes generalization difficult, however, methods like preprocessing, transfer learning, and data augmentation improve model performance and adaptability over a range of datasets [22, 25].
Recent developments in AI for breast cancer detection highlight the effectiveness of deep learning models such as CNNs, MLPs, and DWT-based MRFs in improving early diagnosis by enhancing image clarity and classification precision. Methods like transfer learning, data augmentation, and feature selection techniques (like SVM-RFE) have significantly enhanced model accuracy across various datasets. Nonetheless, key challenges persist, including the scarcity of large, well-labelled datasets, inconsistency in medical imaging, and the lack of interpretability in deep learning model outputs.
3.1 Dataset
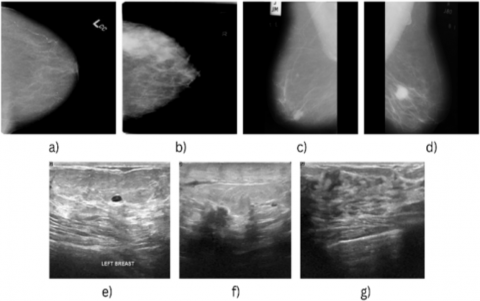
The datasets- CBIS-DDSM mammography dataset, MIAS mammography dataset, and ultrasound breast cancer image dataset were used for this study. The CBIS-DDSM, MIAS, and ultrasound datasets were chosen because they are publicly available, offer sufficient sample sizes, and offer broader scope for evaluation of model performance across different types of breast cancer imaging data [26, 27]. All three datasets are publicly available on Kaggle. Figure 1 shows a few sample images from each of these datasets.
Figure 1. Sample images
Table 1 gives a concise overview of the datasets considered for this study, including the name of the dataset, size, total image count, their format, and the number of classes considered for the classification task.
Table 1. Information about the datasets considered for this study
|
Sr. No. |
Dataset |
Size |
No. of Images |
Image Format |
Number of Classes |
|
1 |
CBIS DDSM breast cancer image dataset |
6 GB |
10239 |
.jpg |
2 (Benign and Malignant) |
|
2 |
MIAS Dataset |
322 MB |
330 |
.pgm |
2 (Normal and Abnormal) |
|
3 |
Ultrasound |
256 MB |
780 |
.png |
3 (Normal, Benign, and Malignant) |
3.2 Implementation
This work was implemented in 3 parts. In the 1st part, the work explored the performance of classic ML algorithms on all three datasets. The second part concentrated on analyzing the execution of established DL models, again on all three datasets. Finally, the 3rd part included the development and evaluation of a custom CNN architecture. This proposed CNN was developed incrementally, adding layers with varying filter sizes and depths. By observing the change in accuracy with each added layer, we were able to rate the effect of different architectural choices on the model's performance in breast cancer detection. The aim behind this was to thoroughly evaluate different models’ performance on different datasets, to gather a detailed assessment of their performance across datasets.
3.2.1 Data preprocessing
Image preprocessing was tailored to each dataset. For CBIS-DDSM, missing image paths were addressed, pathological classifications were mapped to binary (benign/malignant) labels, and images were resized to 224×224 pixels before flattening. MIAS images (.pgm format) were read in grayscale, resized to 64×64, and subsequently flattened. Ultrasound images, classified into benign, malignant, or normal, were converted to grayscale, resized to 128×128, and flattened. Contrast enhancement was tested on the ultrasound dataset but showed minimal impact. Given the limited size of the ultrasound and MIAS dataset, the ImageDataGenerator function was employed during neural network training to augment the data.
Experimentation discovered that the density of the surrounding tissue affects how well breast cancer is detected. Images having a density categorization of F tended to exhibit lesser accuracy than those with D (dense glandular) or G (glandular): according to our examination of the MIAS dataset. A specialized preprocessing pipeline was developed to address this issue for density F images. A tailored image preparation routine was developed to tackle the difficulties inherent in density F (fatty) images. This involved boosting the difference between light and dark areas, reducing distracting background elements, and highlighting the finer points within the fatty tissue. Contrast and brightness adjustments were also performed using linear intensity transformation as shown in Eq. (1):
$I_{n e w}(x, y)=\propto \cdot I_{o l d}(x, y)+\beta$ (1)
where,
$I_{\text {new }}$ and $I_{\text {old }}$ are the pixel intensities before and after enhancement,
$\propto$ controls contrast,
$\beta$ adjusts brightness.
By making those crucial details more distinct, the technique substantially increased how accurately models could categorize density F images.
3.2.2 ML models
Various ML models were examined after image preprocessing. Random Forest, LightGBM, and XGBoost were selected for their effectiveness with high-dimensional data and complex relationships. Logistic Regression gave a simpler, interpretable approach. AdaBoost, using HOG features for images and encoded features for tabular data, showed robustness, particularly with datasets which are not balanced. Naive Bayes, using different encoding techniques, offered efficient and consistent accuracy. Also, kernel-based models, SVM (RBF kernel) and KNN, were explored to address non-linear separability.
Table 2 gives highlights about the selected hyperparameters for the ML models considered in this study. The hyperparameters were chosen based on common best practices as well as the previous studies to balance performance and computational efficiency.
Table 2. Hyperparameters chosen for ML models considered in the study
|
Model |
Selected Hyperparameters |
|
Random Forest |
n_estimators = 100, random_state = 42 |
|
Logistic Regression |
max_iter = 1000 |
|
Decision Tree |
random_state = 42 |
|
XGBoost |
objective = 'multi:softmax', num_class = 3, random_state = 42 |
|
LightGBM |
objective = 'multiclass', num_class = 3, random_state = 42 |
|
SVM |
kernel = 'rbf', C = 1, gamma = 'scale' |
|
KNN |
n_neighbors = 5, weights = 'uniform', metric = 'minkowski' |
|
AdaBoost |
n_estimators = 50, learning_rate = 1.0, base_estimator = DecisionTree(max_depth=1) |
|
Naive Bayes |
var_smoothing = 1e-9 |
3.2.3 DL models
The DL algorithms- ResNet50, DenseNet121, EfficientNetB0, InceptionV3 and VGG19 were implemented. The model ResNet50, based on ImageNet pre-trained weights, was used to distribute the images into either benign or malignant classes. Another transfer learning algorithm applied in this paper was VGG19 due to its ability to extract hierarchical features and efficiency for image-based tasks. The next model we explored was DenseNet121, which has been trained on a large dataset of diverse images. This model has learned rich visual features that can be transferred to our breast cancer classification task. EfficientNetB0 was another neural network applied due to its high performance, time efficiency, and scalable architecture that makes it capable to handle medical imaging datasets with large resolutions and diverse patterns. A previously trained InceptionV3 model was utilized for breast cancer image classification, using its deep feature extraction capabilities while adding custom layers for task-specific learning.
3.2.4 Custom CNN models/proposed model
(1) Ultrasound
By gradually improving its architecture, this study created a customized CNN for ultrasound and mammography datasets. Additional convolutional layers (64, 128, 256, and 512 filters) with max-pooling, dropout, and data augmentation gradually enhanced feature extraction and generalization after a basic model with an accuracy of 0.68 was used as a starting point. With 512 filters and data augmentation, the final model's accuracy of 0.86 showed how well it handled variances in the real world. The accuracy improvement can be represented as:
Final Accuracy = Initial Accuracy $+\sum \Delta A_i$ (2)
where, $\Delta A_i$ represents the accuracy gain from each enhancement step, such as additional layers or data augmentation.
(2) Mammogram
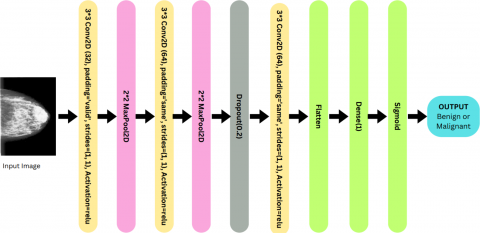
Starting with a 32-filter convolutional layer (3×3 kernel, stride 1, ‘valid’ padding) and ReLU activation to extract low-level features, we present a bespoke CNN for medical image categorization. After reducing spatial dimensions and complexity with MaxPooling (2×2), further convolutional layers (64 filters, 3×3, 'same' padding) are used to extract high-level features (see Figure 2). Overfitting is avoided by a Dropout layer (0.2), and feature maps are transformed for completely connected layers by a Flatten layer. Binary categorization is made possible by the last Dense layer with a sigmoid activation. The model’s efficacy for medical image analysis was demonstrated by its iterative revisions, which increased accuracy from 62% to 97%. The iterative improvements in the model can be expressed as Eq. (3):
$A_n=A_0+\sum_{i=1}^n f\left(T_i, D_i, P_i\right)$ (3)
where, $A_n$ is the final accuracy, $A_0$ is the initial accuracy, and $f\left(T_i, D_i, P_i\right)$ represents the contribution of transformations $T_i$, dropout $D_i$, and pooling $P_i$, at each step $i$.
Figure 2. Design of the suggested CNN model for mammograms
This section gives an overview of the findings of this study in terms of performance metrics- Precision, recall, and F1-score. Precision measures the accuracy of positive predictions (True Positives / (True Positives + False Positives)): Recall quantifies the ability to identify all positive instances (True Positives / (True Positives + False Negatives)): and F1-score is the harmonic mean of precision and recall, providing a balanced measure (2 * (Precision * Recall) / (Precision + Recall)). These metrics help in evaluating the performance, especially in imbalanced datasets.
4.1 Machine learning
The performance of different models varied across the three datasets, as summarized in Table 3, where Decision Tree performed best on MIAS, AdaBoost on ultrasound, and Random Forest on CBIS-DDSM. Random Forest consistently achieved strong results, followed by XGBoost, LightGBM, and Decision Tree. Naive Bayes, KNN, and SVM generally showed lower accuracy.
As observed in Table 3, models based on tree (RF, XGBoost, Decision Tree, LightGBM) generally outperformed others. This is likely because these models are good at capturing complex, non-linear relationships between features and are more tolerant of noise and missing data. In contrast, Naive Bayes showed poor performance, particularly on the MIAS dataset, likely due to its assumption that features are independent. Logistic Regression and SVM also struggled, probably because they are better suited for linear patterns and don’t handle non-linearity or complex interactions as effectively.
Table 3. Accuracy attained by each of the implemented machine learning models for the considered datasets
|
Dataset |
MIAS Mammography |
Ultrasound |
CBIS-DDSM Mammography |
|
Random Forest |
0.69 |
0.74 |
0.72 |
|
Logistic Regression |
0.57 |
0.60 |
0.65 |
|
XGBoost |
0.7 |
0.71 |
0.60 |
|
LightGBM |
0.62 |
0.73 |
0.64 |
|
Decision Tree |
0.75 |
0.58 |
0.57 |
|
Naive Bayes |
0.29 |
0.71 |
0.69 |
|
AdaBoost |
0.55 |
0.79 |
0.69 |
|
SVM |
0.58 |
0.70 |
0.61 |
|
KNN |
0.55 |
0.68 |
0.56 |
The performance of models is significantly affected by the standard of the dataset. For example, MIAS suffers from label duplication and inconsistent entries, leading to redundant and noisy data. Although ultrasound images are generally of high quality, they tend to produce inconsistent results and are limited by a small sample size. CBIS-DDSM, while standardized, has issues with format conversion and lacks essential metadata. These challenges can hinder both the training procedure and the model's potential to generalize, emphasizing need for clean, accurate, and well-labelled data.
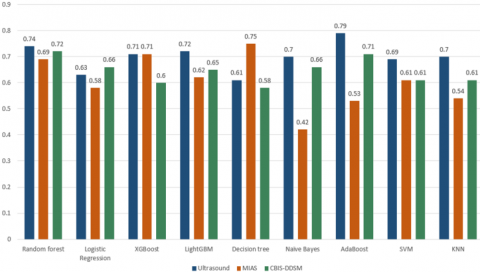
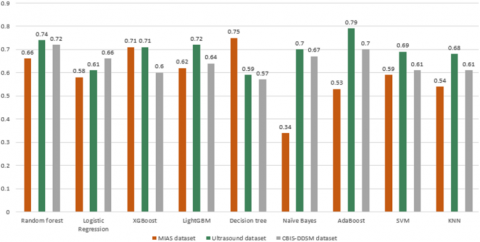
The bar graphs in Figure 3 and Figure 4 portray the performance of ML models based on weighted precision and weighted recall respectively. The bar graph depicted In Figure 5 depicts the performance of all nine ML models for MIAS, ultrasound, and CBIS-DDSM datasets based on F Score.
Figure 3. Performance of ML algorithms across datasets (Precision)
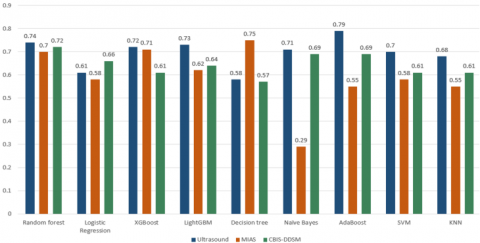
Figure 4. Performance of ML algorithms across datasets (Recall)
Figure 5. Performance of ML algorithms across datasets (F Score)
4.2 DL
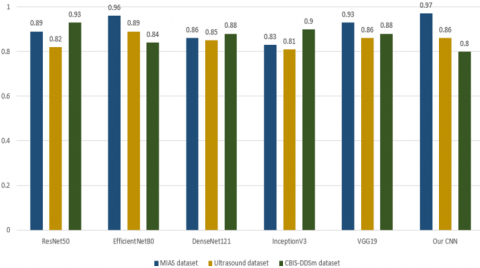
The performance of DL models was higher in comparison to machine learning models. It was noted that RestNet50 gave the best accuracy for the CBIS-DDSM dataset, while EfficientNetB0 performed better on the MIAS and ultrasound datasets, as observed in Table 4.
Table 4. Accuracy attained by DL models for the datasets considered in the study
|
Dataset |
Our CNN |
ResNet50 |
DenseNet121 |
InceptionV3 |
EfficientNetB0 |
VGG19 |
|
Ultrasound |
0.86 |
0.86 |
0.87 |
0.82 |
0.89 |
0.86 |
|
CBIS-DDSM Mammography |
0.80 |
0.93 |
0.88 |
0.90 |
0.84 |
0.88 |
|
MIAS Dataset |
0.97 |
0.91 |
0.88 |
0.83 |
0.89 |
0.86 |
From Table 4, ResNet50 and EfficientNetB0 performed well across all datasets. Their relatively simple and efficient architectures help reduce overfitting, making them better suited for smaller or less consistent datasets. In contrast, DenseNet121 and InceptionV3, which have more complex architectures, showed weaker performance on smaller datasets but performed better on CBIS-DDSM, likely due to its larger size and better standardization. These results suggest that simpler models tend to generalize better on limited data, while more complex models benefit from larger, high-quality datasets.
The proposed CNN achieved remarkable accuracy, demonstrating its effectiveness in classifying medical images with minimal misclassifications. The iterative refinement of the architecture, from a basic model with a single convolutional layer to the final configuration, significantly improved performance. Key enhancements, including MaxPooling layers for feature extraction and noise reduction, additional convolutional layers for learning complex features, and Dropout for regularization, collectively boosted accuracy from 62% to 97% (see Table 5). These refinements enabled the model to generalize well across test data by mitigating overfitting and extracting deeper hierarchical features essential for classification. This progression validates the CNN's reliability and robustness for medical imaging applications.
Table 5. Trends in the accuracy after addition of CNN layers for the proposed CNN for mammograms
|
Model Version |
Layers Added |
Accuracy |
|
Basic Model |
1 Convolutional Layer, Flatten, Dense |
0.62 |
|
Version 2 |
+ MaxPooling Layer |
0.75 |
|
Version 3 |
+ Additional Convolutional Layer |
0.85 |
|
Version 4 |
+ Dropout Layer |
0.91 |
|
Final Model |
+ Third Convolutional Layer |
0.97 |
Figure 6. Performance of DL algorithms across datasets (Precision)
Figure 7. Performance of DL algorithms across datasets (Recall)
Figure 8. Performance of DL algorithms across datasets (F-Score)
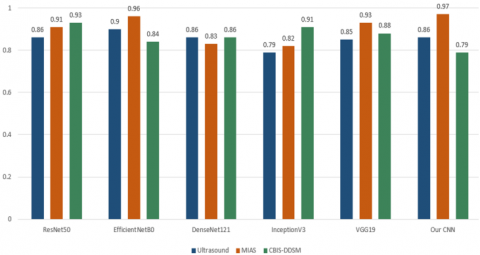
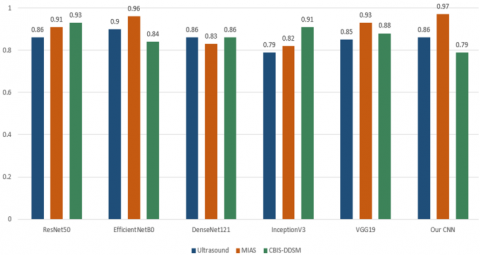
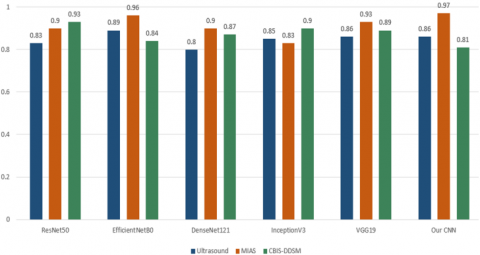
The bar graphs in Figure 6 and Figure 7 portray the performance of DL models based on weighted precision and weighted recall, respectively.
The bar graph depicted in Figure 8 represents the results of all five DL models and our own CNN’s for MIAS, ultrasound, and CBIS-DDSM datasets.
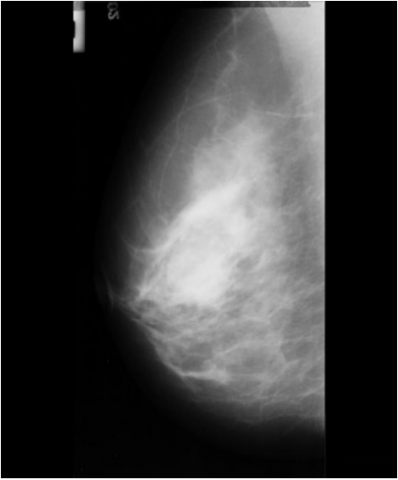
The performance of DL models on different datasets can vary due to data quality, size, and consistency. For example, the MIAS mammography dataset and CBIS-DDSM yield good results because they are curated, annotated, and large-scale datasets with standardized formats, which help models learn effectively. However, limitations like duplicated labels in MIAS and missing age information in CBIS-DDSM can impact the robustness of results. In contrast, the ultrasound dataset has inconsistencies, such as smaller sample size (780 images), potential class imbalance, and lower resolution, leading to varying accuracy. Such issues emphasize the importance of dataset quality, proper preprocessing (e.g., handling DICOM to JPEG conversion): and addressing flaws like labelling errors to ensure reliable model performance. Figure 9 shows one of the images wrongly classified as benign.
Figure 9. Wrongly classified image
During our experiments with models on mammography, datasets revealed that denser tissue images were more prone to misclassification. Breast tissue density can hide underlying lesions, making them hard to get detected by the naked eye as well as models. Traditional feature extraction techniques may not be enough to detect these complex patterns in dense breast tissue leading to incorrect classification. We applied each DL model density wise to MIAS dataset images and observed a significantly lower accuracy for images with density F(fatty) than images of density G(glandular) and density D(dense glandular). While this problem persists, we were able to notably improve the accuracy of the classification of Fatty tissue images in the MIAS dataset through the additional image preprocessing we applied to them. The increase in accuracy can be observed below in Table 6.
Table 6. Performance on fatty tissue images
|
Image Type |
ResNet50 |
EfficientNetB0 |
DenseNet121 |
InceptionV3 |
VGG19 |
|
Density F |
0.89 |
0.82 |
0.86 |
0.75 |
0.78 |
|
Density F with preprocessing |
0.94 |
0.88 |
0.92 |
0.83 |
0.82 |
This study provides a detailed evaluation of both traditional ML and DL models for breast cancer detection using mammographic and ultrasound images. While DL models such as EfficientNetB0, DenseNet121 and our CNN demonstrated consistently good results in terms of accuracy it was observed that decision tree-based ML models like Random Forest and XGBoost performed better on the smaller datasets where DL models lagged due to insufficient training data till image generation was used to rectify the issue. DL models also require substantial computational resources and large datasets for training, which is not always feasible.
The implementation of DL models density wise on MIAS dataset also revealed significantly lower accuracy for images with fatty breast tissue density. While this limitation was rectified to a certain extent by utilizing additional image processing techniques as observed in this study the accuracy of fatty density still remained lower than that of other densities.
Despite promising advancements significant challenges such as public availablity of large, annotated datasets with images of good quality as well as high computational power requirements stand in the way of integrating AI in cancer detection. Moreover, the lack of interpretability in model decisions makes it hard for clinicians to fully trust and adopt these systems.
[1] Tran, T.X.M., Chang, Y., Kim, S., Song, H., Ryu, S., Park, B. (2023). Association of breast cancer family history with breast density over time in Korean women. JAMA Network Open, 6(3): e232420-e232420. https://doi.org/10.1001/jamanetworkopen.2023.2420
[2] Al-Shami, K., Awadi, S., Khamees, A.A., Alsheikh, A.M., et al. (2023). Estrogens and the risk of breast cancer: A narrative review of literature. Heliyon, 9(9): e20224. https://doi.org/10.1016/j.heliyon.2023.e20224
[3] Micha, J.P., Rettenmaier, M.A., Bohart, R.D., Goldstein, B.H. (2022). Hormone therapy and risk of breast cancer: Where are we now? Journal of Menopausal Medicine, 28(2): 47. https://doi.org/10.6118/jmm.21035
[4] Rainey, L., Eriksson, M., Trinh, T., Czene, K., Broeders, M.J., van Der Waal, D., Hall, P. (2020). The impact of alcohol consumption and physical activity on breast cancer: The role of breast cancer risk. International journal of cancer, 147(4): 931-939. https://doi.org/10.1002/ijc.32846
[5] Shapira, N. (2017). The potential contribution of dietary factors to breast cancer prevention. European Journal of Cancer Prevention, 26(5): 385-395. https://doi.org/10.1097/cej.0000000000000406
[6] Baccouche, A., Garcia-Zapirain, B., Zheng, Y., Elmaghraby, A.S. (2022). Early detection and classification of abnormality in prior mammograms using image-to-image translation and YOLO techniques. Computer Methods and Programs in Biomedicine, 221: 106884. https://doi.org/10.1016/j.cmpb.2022.106884
[7] Halim, E., Halim, P.P., Hebrard, M. (2018). Artificial intelligent models for breast cancer early detection. In 2018 International Conference on Information Management and Technology (ICIMTech), Jakarta, Indonesia, pp. 517-521. https://doi.org/10.1109/ICIMTech.2018.8528140
[8] Bahl, M., Barzilay, R., Yedidia, A.B., Locascio, N.J., Yu, L., Lehman, C.D. (2018). High-risk breast lesions: a machine learning model to predict pathologic upgrade and reduce unnecessary surgical excision. Radiology, 286(3): 810-818. https://doi.org/10.1148/radiol.2017170549
[9] Al-shamasneh, A.R.M., Obaidellah, U.H.B. (2017). Artificial intelligence techniques for cancer detection and classification: Review study. European Scientific Journal, 13(3): 342-370. https://doi.org/10.19044/esj.2017.v13n3p342
[10] Kritz J. (2016). Artificial intelligence achieves near-human performance in diagnosing breast cancer. https://www.sciencedaily.com/releases/2016/06/160620085204.htm.
[11] Tehrani, N., Miller, D. (2018). The impact of artificial intelligence on cancer. Global Journal of Advanced Research, 5(1): 1-3.
[12] Bhola, A., Tiwari, A.K. (2015). Machine learning based approaches for cancer classification using gene expression data. Machine Learning and Applications: An International Journal, 2(3/4): 1-12. https://doi.org/10.5121/mlaij.2015.2401
[13] Zhen, L., Chan, A.K. (2001). An artificial intelligent algorithm for tumor detection in screening mammogram. IEEE Transactions on Medical Imaging, 20(7): 559-567. https://doi.org/10.1109/42.932741
[14] Agarap, A. F. M. (2018). On breast cancer detection: an application of machine learning algorithms on the Wisconsin diagnostic dataset. In Proceedings of the 2nd International Conference on Machine Learning and Soft Computing, Phu Quoc Island, Vietnam, pp. 5-9. https://doi.org/10.1145/3184066.3184080
[15] Miller, D.D., Brown, E.W. (2018). Artificial intelligence in medical practice: The question to the answer? The American journal of medicine, 131(2): 129-133. https://doi.org/10.1016/j.amjmed.2017.10.035
[16] Guo, Y., Liu, Y., Oerlemans, A., Lao, S., Wu, S., Lew, M.S. (2016). Deep learning for visual understanding: A review. Neurocomputing, 187: 27-48. https://doi.org/10.1016/j.neucom.2015.09.116
[17] Cancer survival statistics. https://www.wcrf.org/preventing-cancer/cancer-statistics/cancer-survival-statistics/.
[18] Roslidar, R., Rahman, A., Muharar, R., Syahputra, M.R., et al. (2020). A review on recent progress in thermal imaging and deep learning approaches for breast cancer detection. IEEE Access, 8: 116176-116194. https://doi.org/10.1109/ACCESS.2020.3004056
[19] Sengar, P.P., Gaikwad, M.J., Nagdive, A.S. (2020). Comparative study of machine learning algorithms for breast cancer prediction. In 2020 Third International Conference on Smart Systems and Inventive Technology (ICSSIT): Tirunelveli, India, pp. 796-801. https://doi.org/10.1109/ICSSIT48917.2020.9214267
[20] Sun, Y.S., Zhao, Z., Yang, Z.N., Xu, F., et al. (2017). Risk factors and preventions of breast cancer. International Journal of Biological Sciences, 13(11): 1387. https://doi.org/10.7150/ijbs.21635
[21] Ciregan, D., Meier, U., Schmidhuber, J. (2012). Multi-column deep neural networks for image classification. In 2012 IEEE Conference on Computer Vision and Pattern Recognition, Providence, RI, USA, pp. 3642-3649. https://doi.org/10.1109/CVPR.2012.6248110
[22] Khuriwal, N., Mishra, N. (2018). Breast cancer detection from histopathological images using deep learning. In 2018 3rd International Conference and Workshops on Recent Advances and Innovations in Engineering (ICRAIE), Jaipur, India, pp. 1-4. https://doi.org/10.1109/ICRAIE.2018.8710426
[23] Shweikeh, E., Lu, J., Al-Rajab, M. (2021). Detection of cancer in medical images using deep learning. International Journal of Online & Biomedical Engineering, 17(14): 164-171. https://doi.org/10.3991/ijoe.v17i14.27349
[24] Singh, A.K., Gupta, B. (2015). A novel approach for breast cancer detection and segmentation in a mammogram. Procedia Computer Science, 54: 676-682. https://doi.org/10.1016/j.procs.2015.06.079
[25] Prakash, S.S., Visakha, K. (2020). Breast cancer malignancy prediction using deep learning neural networks. In 2020 Second International Conference on Inventive Research in Computing Applications (ICIRCA), Coimbatore, India, pp. 88-92. https://doi.org/10.1109/ICIRCA48905.2020.9183378
[26] CBIS-DDSM: Breast cancer image dataset. https://www.kaggle.com/datasets/awsaf49/cbis-ddsm-breast-cancer-image-dataset/data.
[27] Breast ultrasound images dataset. https://www.kaggle.com/datasets/aryashah2k/breast-ultrasound-images-dataset.