S. Jackson Irudhayam*![]() | Hariram Venkatesan
| Hariram Venkatesan![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The objective of this research is to analyze the dissemination of stress in the bone surrounding orthopedic implants composed of various compositions of CFR-PEEK, a material that can be tailored with diverse physical, mechanical, and surface characteristics. Also, this study aims to compare the stress distribution between models constructed with PEEK components, GFR-PEEK, implants reinforced with 30% carbon fiber (30% CFR-PEEK), and implants reinforced with 60% carbon fiber (60% CFR-PEEK), considering different geometric variations. The one-piece dental implant was modelled using solidworks (CAD) software. A 3D FEA model was created to simulate the one-piece dental implant system and the surrounding bone. The model incorporated various geometric design variables, including implant length, diameter and thread pitch. Different loading conditions were enforced to assess the stress dissemination within the implant and bone. The 3D FEA simulations revealed that varying the geometric design variables of the one-piece dental implant significantly influenced the stress distribution. Moreover, the choice of biomaterial for the implant played a crucial role in stress distribution. The findings indicate that a 60% CFR-PEEK implant with continuous carbon fiber disperses pressures in a similar manner to a titanium implant. However, for optimal performance, the study suggests that a percentage of endless carbon fibers within the PEEK matrix below 60% would provide the most ideal elasticity while maintaining minimum deformability and minimal stress distribution during loading. It is important to consider the biological characteristics of the materials along with the study's results. For dental implants with specific parameters (0.8 mm single thread pitch and Type II bone quality), the study suggests that the next best option after a 60% CFR-PEEK material would be a 30% CFR-PEEK material. This is because the higher concentration of carbon fiber in the 60% CFR-PEEK material increases the risk of potential contact with individuals, posing a safety concern.
finite element analysis, implant, stress distribution, CFR PEEK, dental biomaterials, implant design
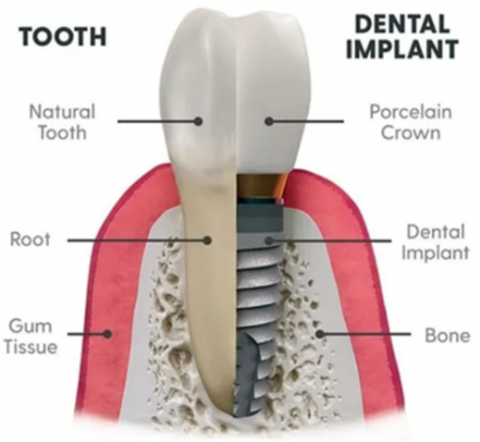
Dental implants are employed to substitute teeth that are lost or impaired in individuals who possess either a complete or partial set of teeth [1]. The fibrous connective tissue that exists among the cementum and alveolar bone in the presence of real teeth serves as a resilient barrier to protect against occlusal forces [2]. Figure 1 provides a detailed view of the dental implant. Osseointegrated implant-supported dentures have revolutionized clinical dentistry treatments. The long-term viability of the implant is a crucial determinant in enhancing the efficacy and durability of implants. Thus, obtaining primary rigidity during implant loading is one of the most essential and basic goals of implant implantation [3]. The main steadiness of the implant is determined by factors such as the quantity of the implant as well as the quality of the bone, the procedure used, and the shape of the implant. Inadequate initial stability results in failure of the implant. To ensure the success of Osseointegration, dental implants are specifically engineered to provide main stability. In order for osseointegration, the process of bone fusing with a dental implant, to be effective in a traditional dental implant repair, a continuous healing period lasting three to six months is necessary [4].
Figure 1. Dental implant with natural teeth
Source: www.rexburgappletreedental.com
Osseointegrated dental implants provide direct load transfer from the implant's static and dynamic pressures to the surrounding bone of the patient. Possible consequences of these pressures include prosthetic failure, fracture at the bone-implant interface, instability of the implant-abutment structure, and unintentional tissue in the bone disintegration [5]. The efficacy of these implants relies on the direct transmission of forces across the implant and adjacent bone. The transfer of load is essential for the osseointegration process, which involves the establishment of a strong and functional contact among the implant and the adjacent bone [6].
It is emphasized that the implant's static and dynamic forces must be meticulously controlled to guarantee the implant's success. In addition, they emphasize the several causes that might contribute to the failure of an implant, including fracture at the point of contact between the bone and the implant, deterioration of the implant-abutment framework, and unintentional loss of bone tissue. Hence, understanding the interplay between the implant and the adjacent bone is crucial for achieving effective osseointegration. Shamami et al. [7] conducted research that emphasizes the significance of load transmission in the success of implants. The authors highlight the need of a "favorable biomechanical environment" to guarantee the implant's ability to endure the applied pressures throughout its use. In addition, they provide an explanation of the several variables that might influence load transfer, including aspects such as implant design, bone density, and the quality of the contact between the implant and bone.
The research conducted by Chun et al. [3] examines the many elements that might influence the process of osseointegration. The success of the implant is determined by the design, surface qualities, and surgical location of the implant, according to their observations. Additionally, they highlight the need of taking into account the implant's interaction with adjacent elements, such as abutments, in order to effectively regulate load distribution. Therefore, the effectiveness of osseointegrated dental implants relies on the accurate handling of load distribution among the implant and surrounding bone. Chun et al. [3], Aguir et al. [6], and Shamami et al. [7] have emphasized the significance of load transfer in multiple studies, stressing the requirement for a favourable biomechanical setting and meticulous evaluation of the implant's design, surface properties, and proximity to adjacent components. Hence, it is crucial to take into account the interplay among the bone and the implant for the achievement of good osseointegration, as well as their correlation with adjacent components [8]. A literature study conducted to evaluate the appropriateness of zirconia as a material for dental implants. The authors performed an extensive search across several databases to locate relevant papers published between 1990 and 2011 [9].
The evaluation included both laboratory-based and live organism-based research that assessed the compatibility with living tissue, physical characteristics, and real-world effectiveness of zirconia implants. The researchers discovered additional studies that satisfied the predefined criteria for inclusion and conducted an analysis of the findings in order to form definitive conclusions on the efficacy of zirconia as a material for implants. The review found that zirconia had excellent biocompatibility, with minimal inflammatory responses observed in vivo studies. Zirconia also exhibited high mechanical strength, fracture resistance, and wear resistance, making it a viable alternative to traditional titanium implants. However, the review also identified some potential concerns with zirconia implants. For example, zirconia has relatively low fracture toughness and susceptibility to fatigue failure may increase the risk of implant fractures, particularly in areas with high occlusal forces. The study also emphasized the need for longer-term clinical trials to evaluate the efficacy of zirconia implants over extended periods. Titanium materials have additionally been linked with medical concerns including scattered radiation, interface degradation and infection related to peri-implantitis, and occasional metal hypersensitivity and allergies. As the importance of very attractive implants increases, the metallic appearance of Titanium materials might provide a challenge [10].
Researchers found that zirconia is a potential titanium implant substitute with good biocompatibility and mechanical qualities. The evaluation also noted the need for further research to thoroughly assess zirconia implants long-term function and identify any issues. The study provides light on zirconia implants and emphasizes the need for further research [9]. Dental implants should have long-term operational stability, reduced surgical and prosthetic operations, good treatment result prediction, and appropriate structural design. Ensuring the transmission of occlusal forces to the implant interface is vital for the success of dental implants. Factors such as stress type, interface topography, bone volume, material properties of the implant, and implant design all influence the transmission of forces at the interface between the bones and the implant. If the implant profile could decrease deformation, stress, or homogenize distribution, it would be more successful. Implant materials should be biocompatible, strong, durable, corrosion-resistant, wear-resistant, and fracture-resistant. Zirconia is utilized for its durability, corrosion resistance, and beauty. Numerous studies have demonstrated that zirconia is biocompatible and has lower microorganism accumulation than titanium [11].
Edher and Nguyen [12] reviews studies on porous implant surfaces and osseointegration. Porous dental implants promote bone development. Using sintering, acid etching, or plasma spraying, the implant may be porous. The porous implant surface gives bone cells more room to connect and develop, integrating it with the surrounding bone tissue. Dental implants need osseointegration for long-term success. Biocompatible titanium is used to make porous dental implants that encourage bone formation. They are utilized in implant-supported dentures and single-tooth replacement. However, they cost more and are harder to make than smooth-surfaced implants. It's harder to clean, which may lead to bacterial colonization and implant failure. Porous materials may enhance metal allergy or sensitivity risk. Zirconia implants are weaker than titanium implants. While sturdy and durable, zirconia implants may shatter unlike metals. High chewing pressure might fracture them. Zirconia implants take greater expertise to install since implant parts are commonly connected (one piece). 95% of titanium implants survive years. They live 20 years on average. Not enough study has examined zirconia implants' long-term success. Ceramic or zirconia crowns worsen the lack of flexibility of zirconia implants [13]. The need for novel materials with better mechanical qualities has been prompted by the potential repercussions of this lack of flexibility. Zirconia, which has a high elastic modulus and minimal thermal deterioration, is one material that several researchers have tried to develop as a replacement for titanium dental implants. Additional alternatives have been developed using polymeric materials, such as Polyether ether ketone (PEEK). A linear polycyclic thermoplastic with semi-crystals known as PEEK was created in 1978. It can be used with components such as implant abutments, implant bodies, and superstructures [10].
The objective of the work is based on the following fundamental requirements for the finest dental implants as follows:
By taking into account the fundamental needs, a better implant design is justified in this work utilizing computational methods. The objective of this investigation is to examine the impact of thread pitch and bone behaviors on stress dissemination in bone using 3D computational methods. This computational tool is commonly employed in dental treatment for evaluating various factors in bone, and it similarly enables investigators to forecast the stresses and strains in other areas of the bone implant system.
Numerous researchers [9-12] who conducted material selection study proposed that PEEK might be used as an implant body, implant abutment, or superstructure.
PEEK provides a number of therapeutic advantages over Ti as a dental implant material.
PEEK demonstrates reduced stress absorption in comparison to Titanium (Ti) as the main anchoring element for implants in teeth due to its robust characteristics that are perfectly compatible with bone. PEEK abutments, reinforced with titanium, might be a superior alternative to traditional titanium abutments because PEEK has enhanced capacity to maintain bone length and stability in soft tissue. PEEK is a biocompatible substance that has a lower likelihood of triggering allergic responses compared to titanium. Additionally, it exhibits greater resistance to corrosion [14].
PEEK has a considerably decreased modulus of elasticity when compared to substances made of bone from the cortical region, titanium, and ceramics. The heightened modulus of elasticity of PEEK is crucial for implant-related components, namely for abutments and superstructures. strengthened PEEK composites, such as CFR-PEEK and GFR-PEEK, may attain modulus of elasticity of 19.7 GPa, 18 GPa, 150 GPa, and 10.5 GPa, accordingly. Table 1 is a list of the various materials along with their Young's modulus and corresponding Poisson ratio. PEEK is already known for its biocompatibility, but its mechanical properties, such as strength and stiffness, can be improved by adding fibers.
This research conducted a comparative analysis of multiple designs comprising of PEEK components, GFR PEEK, implant teeth reinforced with 30% CFR PEEK, and dental prostheses reinforced with 60% CFR PEEK to examine how they distributed of stress in the bone next to it of the implant. The study was performed using the 3D computational approach [15].
Table 1. Young’s modulus of various materials
|
Materials |
Young’s Modulus (GPa) |
Poisson Ratio |
|
Cortical bone |
13.7 |
0.3 |
|
Dense cancellous bone Type II, Type III |
1.37 |
0.3 |
|
Low-dense cancellation bone |
0.231 |
0.3 |
|
Titanium |
110 |
0.35 |
|
Zirconia |
210 |
0.24 |
|
PEEK |
4.1 |
0.4 |
|
CFR-PEEK |
12 |
0.4 |
|
30% CFR PEEK |
18 |
0.39 |
|
60% CFR PEEK |
150 |
0.35 |
|
GFR-PEEK |
10.5 |
0.35 |
Based on the literature review, there are four primary classifications of bone. Since type 1 bone is exclusively made up of the cortical bone, we focused our investigation on Type II, III, and IV bones. The cortical bone layer thickness has been modified to distinguish between different kinds of bones. The Type II model had a condensed core of cancellous bone encircled by a cortical bone shell measuring 2 mm in thickness. The main distinction between Type III bone and type IV bone is in their internal structure. Type III bone is characterized by a compact cancellous bone core, whereas type IV bone has a less dense cancellous bone core that is encased by a 1 mm thick layer of cortical bone. Type II bone is the optimal choice for achieving osseointegration of implanted teeth [16]. Initial stabilities are ensured by effective cortical anchoring. The work focuses on analysing the Type II bone.
It has been suggested that modifications to dental implant design can raise the survival rate of initial loading by achieving primary stability and reducing micromotions. Maximizing first contact, enhancing initial stability, and improving stress distribution are all goals of the thread design. Other significant geometric variables utilised to assess the effects of biomechanical pressures and bone implant contact include thread depth, width, pitch, helix, and face angle. Therefore, taking into account the implant thread profile is crucial for the advancement of dental implant systems. The impact of implant thread pitch on surface interactions and insertion speed makes it a crucial design factor. The dental implants were fabricated using a single threaded thread design, which consisted of a V-shaped cylinder of 3.5 mm in diameter and 13 mm in length. The collar had a height of 0.3 mm, and the helix angle was set at 60°. This geometry was created by using three different pitch values: 0.8 mm, 1.0 mm, and 1.2 mm. The implant has dimensions of 3.5 mm. The bone transplants were fabricated using Type II bone density. The screw threaded implant structure shown in Figure 2 was created with SolidWorks software (SOLIDWORKS EDU Edition 2022-23), a 3D modelling tool, with a pitch value of 0.8 mm. Measurements are obtained from the manufacturer and the dimensions are within the specified range for Type II bone, as stated in the literature.
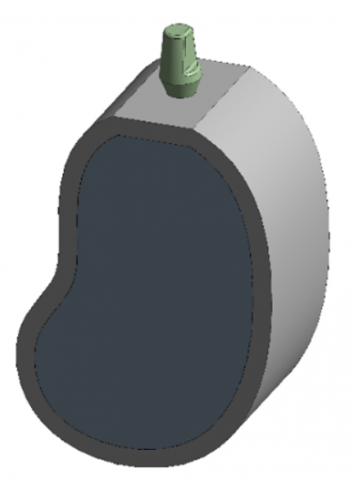
Figure 3 illustrates the correlation between the bone and the implant for Type II Bone Integrity. Artificial teeth structural model was discretized using the first-order four-node tetrahedral components. Table 2 presents a thorough breakdown of the quantity of nodes and items that are now present. The existing computational models were imported into the Ansys workbench (ANSYS 20.0 R1 software) application to perform simulations. The implant and bone were believed to establish an optimal connection. The connections between various structures were joined together, using the linear analysis. The friction coefficient of the implant-bone contact is influenced by the force exerted and the chemical constituents of the material. An optimal coefficient of friction for PEEK material in the manufacture of dental implants is approximately 0.2, as indicated [17]. A nonlinear frictional interaction element was included in the creation of the FEA model to ensure initial stabilization when subjected to rapid loading conditions.
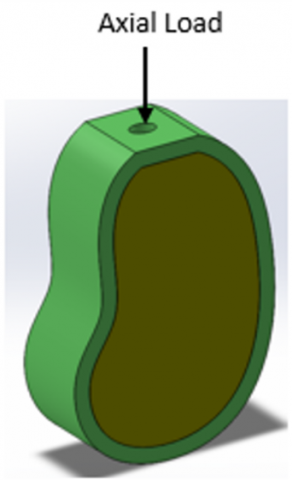
Horita et al. [18] found that the nodes on the inner, outer, and lower surfaces of the bone-implant models were restricted from moving in any direction (as shown in Figure 4). During this study, a 200 N axial load was exerted on the central region of the abutment surface. Implants engineered to bear axial stresses often exhibit enhanced resistance to lateral and oblique loads, owing to their structural integrity and the high quality of their implant-bone contact.
Figure 2. Single thread with Pitch of 0.8 mm
Figure 3. Bone-implant interface–Type II
Table 2. Meshed nodes and elements for each thread design
|
Material |
Node |
Element |
|
0.8 mm Pitch Single Thread–Type II Bone type |
||
|
30%CFR PEEK |
669006 |
468103 |
|
60%CFR PEEK |
669006 |
468103 |
|
PEEK |
669006 |
468103 |
|
GFR PEEK |
669006 |
468103 |
|
1mm Pitch Single Thread–Type II Bone type |
||
|
30%CFR PEEK |
662790 |
464576 |
|
60%CFR PEEK |
662790 |
464576 |
|
PEEK |
662790 |
464576 |
|
GFR PEEK |
662790 |
464576 |
|
1.2mm Pitch Single Thread–Type II Bone type |
||
|
30%CFR PEEK |
658987 |
462356 |
|
60%CFR PEEK |
658987 |
462356 |
|
PEEK |
658987 |
462356 |
Figure 4. Loads and restrictions
3.1 Stress analysis in bone
The findings included a comparison of three distinct pitches and their corresponding bone properties. Tables 3 and 4 provide the highest von-Mises stresses observed in cancellous bone and cortical bone under axial strain for four distinct materials and three distinct pitches, all of which had Type II bone quality.
Table 3. Cancellous bone–von-Mises stress
|
Cancellous Bone |
MIN (MPa) |
MAX (MPa) |
AVE (MPa) |
|
(Type II Bone Quality, Single Thread 0.8 mm, Vertical Load) |
|||
|
30% CFR PEEK |
2.4818e-002 |
8.5696 |
0.24811 |
|
60% CFR PEEK |
3.0796e-002 |
7.2483 |
0.28159 |
|
PEEK |
1.727e-002 |
11.534 |
0.21799 |
|
GFR PEEK |
2.2705e-002 |
9.1442 |
0.23732 |
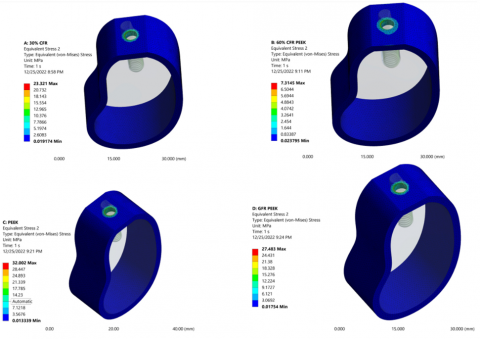
Table 4. Cortical bone–von-Mises stress
|
Cortical Bone |
MIN (MPa) |
MAX (MPa) |
AVE (MPa) |
|
(Type II Bone Quality, Single Thread 0.8 mm, Vertical Load) |
|||
|
30% CFR PEEK |
1.9174e-002 |
23.321 |
0.19981 |
|
60% CFR PEEK |
2.3795e-002 |
7.3145 |
0.16296 |
|
PEEK |
1.3339e-002 |
32.002 |
0.25463 |
|
GFR PEEK |
1.754e-002 |
27.483 |
0.21789 |
3.2 Vertical load
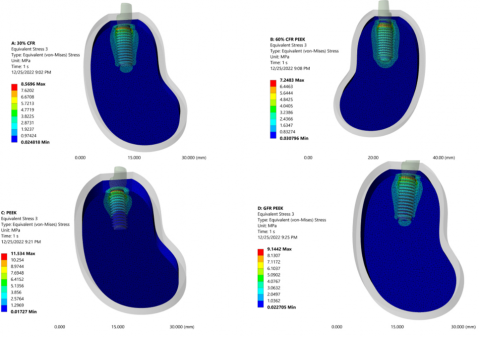
The PEEK, GFR PEEK, 30% CFR PEEK, and 60% CFR PEEK materials exhibited the greatest von-Mises stresses in cancellous bone when subjected to a vertical load with pitch sizes of 0.8, 1.0, and 1.2 mm. This was true independent of the implant pitch for Type II bone quality. The stress distribution of a single threaded implant with a pitch of 0.8 mm in cancellous bone, constructed from various implant materials, is shown in Figure 5. Comparatively, the von-Mises stress attained is lowest in 60% CFR PEEK and subsequently in 30% CFR PEEK, in comparison with the other two materials.
In addition, the average stress was reduced when Type II bone was treated with 0.8 mm pitch single threaded implants made of 30% CFR PEEK and 60% CFR PEEK. When compared to comparable implants with a 0.8mm thread pitch, 60% CFR PEEK achieves the least amount of stress in cortical bone which is shown in Figure 6. When 0.8mm, Type II bone grade 60% CFR PEEK is used instead of 30% CFR PEEK, the percentage of average stress is reduced rapidly.
Figure 5. von-Mises stress distribution in cancellous bone for 0.8 mm pitch
Figure 6. Cortical bone von-Mises stress distribution for 0.8 mm pitch
Dental implants' success is determined by number of biomechanical parameters, considering the type of load applied to the implant, its surface properties, its shape, and how well the surrounding bone is working [19]. Numerous factors, including the implant's length, depth, diameter and pitch of the thread, can determine how much weight is transferred to the neighbouring bone [20, 21]. Threads are engineered to maximize the efficiency of the first contact, improve the initial balance, increase the surface region of the implant, and enable the distribution of stress at the contact area [22, 23]. Moreover, several structural features like thread depth, thickness, helix angle, face angle, and pitch may be modified to impact the effectiveness of the thread and alter the way the load is distributed throughout the implant. Of all the characteristics of a thread, the thread pitch is considered crucial because to its significant clinical implications for a treatment and potential effects on implantation time and functional comfort [12].
This research mainly concentrates on the pitch. The thread pitch, type of bone, and properties of the materials used for the implants are the key factors affecting the dental plant's ability to survive. Bone quality affects how stress is distributed. The Type II bone Quality is the major subject of this investigation. Depending on the direction of the fibres, fiber-containing polymers like Endoligns exhibit varying moduli of elasticity [24]. The early stability of implants is significantly influenced by cortical bone thickness. According to the study, when compared to the same type of implant in Type II bone, the micromotion of the 0.8 mm pitch single threaded implant rose by 357.6% and 668.7% in type IV bone, respectively, under vertical and horizontal stresses [25]. Numerous works on dental implants using the finite element analysis make the assumption that every material is isotropic and linearly elastic, and that the von-Mises stresses are the measurement unit for the observed stresses [26]. Since the elements utilised in implants will transfer the stress caused by a load in bone, they are crucial in terms of biochemical and biomechanical qualities. Therefore, the main focus of this study is on the types of materials used today that are not titanium and zirconium, hence the convergence test and mechanical validation is not taken as scope of this research.
It is used to alter the physical characteristics of bioactive substances in various types of living bone tissues. The bioactive properties of PEEK implants, such as their ability to adhere to cells and withstand shear forces, may be enhanced by the use of plasma surface treatments and other coating methods [27]. PEEK is used as a material in this inquiry because to its many benefits.
In a number of studies, components of an orthopaedic implant comprised of a CFR-PEEK composite shown notable advantages, particularly in terms of durability. To promote the safe use of CFR-PEEK materials, additional research should be carried out [14, 28]. The implant materials did not have any discernible impact on the stress state. The stress values reached their maximum levels, which were quite near to the strengths of PEEK and (GFR-PEEK), suggesting a significant risk of failure. Implants having lower elastic modulus, such as PEEK and its composites, undergo more deformation at the cortical bone. Implants made of materials that have stronger elastic moduli, such as titanium and zirconia, transfer a greater load to the cancellous bone, as opposed to other materials [15, 29].
Nevertheless, the recorded stresses remained under the threshold of bone strength. Stronger implants, such as those composed of zirconia and titanium, cause less pressure on the bone due to the stress shielding effect. On the other hand, unfilled PEEK implants, which have a lower elastic modulus, show excessive strain and a greater likelihood of overload and fracture. When evaluating one-piece implants made of CFR-PEEK to PEEK, the latter demonstrated a better balance between bone stress and strain, suggesting reduced chances of failure. When designing dental implants that promote better bone preservation, overload resistance, and fracture prevention, it is important to investigate alternate materials that have a similar elastic modulus [30, 31].
The study's results indicate that the stress distribution in a bony segment is mostly influenced by the implant material, pitch variable, and bone quality. The highest stress levels were recorded under vertical loading for all pitch values, different PEEK reinforced with materials, and cortical bone quality. In cancellous bone, however, the situation is the opposite; vertical loading was where the lowest stress levels were found. In light of this, it can be said that vertical loading will spread out horizontal loading if any, and that this means that loading is a crucial element affecting the distribution of stress in cortical bone.
For Type II bone features, the cortical bone experiences more stress than the cancellous bone, and the strength of the stress varies with implant pitch. It demonstrates how altering the dental implant pitch for all bone types can change how stress is distributed. When the implant is subjected to vertical load, a different outcome is seen, and it is shown that, for Type II bone quality, cortical bone experiences the highest stress distribution relative to cancellous bone under these loading conditions. Therefore, using Type II implants of varying pitches has led to inconsistent results in the bony region for vertical loading.
The results demonstrate that pitch modulation significantly alters how cortical and cancellous bone behave biomechanically. This result was in line with other studies that suggested the geometry and thread profile of the implant had an effect on the amount of stress transferred from the implant to the bone [32, 33].
The biochemical performance of the materials utilised for implants is also shown by these results. According to it, the cortical and cancellous bone's maximum stress increases from 60% CFR-PEEK to 30% CFR-PEEK to GFR PEEK to PEEK. This demonstrates that when compared to other materials, 60% CFR-PEEK material achieves the smallest and maximum stress.
According to reliable information in the literature, the pitch of the implant has a vital role in decreasing or lowering the highest levels of stress at the boundary among the bone-implant contact [34]. A three-dimensional finite element study demonstrates that using a narrower thread pitch for a titanium implant reduces the concentration of maximum stress in the bony region. Furthermore, a thread pitch of 0.8 mm is advised, since it is also correlated with the reduction of stress concentration and the preservation of the implant's initial stability [35].
Furthermore, it's crucial to properly transfer occlusal loads to the bone-implant contact, and the functional surface area of the implant body has an impact on how well the implant transfers loads. Edher and Nguyen [12] states that the pitch, depth, and depth of thread design features have an impact on the effective surface area of the implant's body. In order to meet the necessary stress distribution criteria, it is vital to enhance the surface area of the implant by including additional pitches.
The results of this study are consistent with this idea. The bone-implant structure experiences the most stress when an implant's thread pitch is greater than 0.8 mm. When bone density declines, changing the dental implant pitch has no negative impact on how stress is distributed in the bone [36]. Therefore, in this study, which is definitely smaller than 1.6 mm, the pitches of 0.8 mm, 1.0 mm, and 1.2 mm were taken into consideration.
[1] Pjetursson, B.E., Thoma, D., Jung, R., Zwahlen, M., Zembic, A. (2012). A systematic review of the survival and complication rates of implant‐supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clinical Oral Implants Research, 23: 22-38. https://doi.org/10.1111/j.1600-0501.2012.02546.x
[2] Shacham, S., Castel, D., and Gefen, A. (2010). Measurements of the static friction coefficient between bone and muscle tissues. Journal of Biomechanical Engineering, 132(8): 084502. https://doi.org/10.1115/1.4001893
[3] Chun, H.J., Cheong, S.Y., Han, J.H., Heo, S.J., Chung, J.P., Rhyu, I.C., Choi, Y.C. Baik, H.K. Ku, Y., Kim, M.H. (2002). Evaluation of design parameters of osseointegrated dental implants using finite element analysis. Journal of Oral Rehabilitation, 29(6): 565-574. https://doi.org/10.1046/j.1365-2842.2002.00891.x
[4] Sugiura, T., Yamamoto, K., Kawakami, M., Horita, S., Murakami, K., Kirita, T. (2015). Influence of bone parameters on peri-implant bone strain distribution in the posterior mandible. Medicina Oral, Patologia Oral y Cirugia Bucal, 20(1): e66-73. https://doi.org/10.4317/medoral.19878
[5] Eskitascioglu, G., Usumez, A., Sevimay, M., Soykan, E., Unsal, E. (2004). The influence of occlusal loading location on stresses transferred to implant-supported prostheses and supporting bone: A three-dimensional finite element study. The Journal of Prosthetic Dentistry, 91(2): 144-150. https://doi.org/10.1016/j.prosdent.2003.10.018
[6] Aguir, H., Mabrouk, Y., Chamekh, R., Saadellaoui, I. (2023). Influence of implants number on the biomechanical behavior of implant-supported complete prosthesis: A 3D finite element analysis. Heliyon, 9(7): e17956. https://doi.org/10.1016/j.heliyon.2023.e17956
[7] Shamami, D.Z., Karimi, A., Beigzadeh, B., Derakhshan, S., Navidbakhsh, M. (2014). A three-dimensional finite element study to characterize the influence of load direction on stress distribution in bone around dental implant. Journal of Biomaterials and Tissue Engineering, 4(9): 693-699. https://doi.org/10.1166/jbt.2014.1230
[8] Chen, Y.Y., Chen, W.P., Chang, H.H., Huang, S.H., Lin, C.P. (2014). A novel dental implant abutment with micro-motion capability—Development and biomechanical evaluations. Dental Materials, 30(2): 131-137. https://doi.org/10.1016/j.dental.2013.10.007
[9] da Costa Valente, M.L., de Castro, D.T., Macedo, A.P., Shimano, A.C., Dos Reis, A.C. (2017). Comparative analysis of stress in a new proposal of dental implants. Materials Science and Engineering: C, 77: 360-365. https://doi.org/10.1016/j.msec.2017.03.268
[10] Özkurt, Z., Kazazoğlu, E. (2011). Zirconia dental implants: A literature review. Journal of oral implantology, 37(3): 367-376. https://doi.org/10.1563/AAID-JOI-D-09-00079
[11] Lin, C.L., Wang, J.C., Chang, W.J. (2008). Biomechanical interactions in tooth-implant-supported fixed partial dentures with variations in the number of splinted teeth and connector type: A finite element analysis. Clinical Oral Implants Research, 19(1): 107-117. https://doi.org/10.1111/j.1600-0501.2007.01363.x
[12] Edher, F., Nguyen, C.T. (2018). Short dental implants: A scoping review of the literature for patients with head and neck cancer. The Journal of Prosthetic Dentistry, 119(5): 736-742. https://doi.org/10.1016/j.prosdent.2017.06.003
[13] Okumura, N., Stegaroiu, R., Kitamura, E., Kurokawa, K., Nomura, S. (2010). Influence of maxillary cortical bone thickness, implant design and implant diameter on stress around implants: A three-dimensional finite element analysis. Journal of Prosthodontic Research, 54(3): 133-142. https://doi.org/10.1016/j.jpor.2009.12.004
[14] Rahmitasari, F., Ishida, Y., Kurahashi, K., Matsuda, T., Watanabe, M., Ichikawa, T. (2017). PEEK with reinforced materials and modifications for dental implant applications. Dentistry Journal, 5(4): 35. https://doi.org/10.3390/dj5040035
[15] Schwitalla, A.D., Abou-Emara, M., Spintig, T., Lackmann, J., Müller, W.D. (2015). Finite element analysis of the biomechanical effects of PEEK dental implants on the peri-implant bone. Journal of Biomechanics, 48(1): 1-7. https://doi.org/10.1016/j.jbiomech.2014.11.017
[16] Lee, J., Pyo, S.W., Cho, H.J., An, J.S., Lee, J.H., Koo, K.T., Lee, Y.M. (2020). Comparison of implant stability measurements between a resonance frequency analysis device and a modified damping capacity analysis device: An in vitro study. Journal of Periodontal & Implant Science, 50(1): 56-66. https://doi.org/10.5051/jpis.2020.50.1.56
[17] Sarot, J.R., Contar, C.M.M., Cruz, A.C.C.D., de Souza Magini, R. (2010). Evaluation of the stress distribution in CFR-PEEK dental implants by the three-dimensional finite element method. Journal of Materials Science: Materials in Medicine, 21: 2079-2085. https://doi.org/10.1007/s10856-010-4084-7
[18] Horita, S., Sugiura, T., Yamamoto, K., Murakami, K., Imai, Y., Kirita, T. (2017). Biomechanical analysis of immediately loaded implants according to the “All-on-Four” concept. Journal of Prosthodontic Research, 61(2): 123-132. https://doi.org/10.1016/j.jpor.2016.08.002
[19] Mohammed Ibrahim, M., Thulasingam, C., Nasser, K.S.G.A., Balaji, V., Rajakumar, M., Rupkumar, P. (2011). Evaluation of design parameters of dental implant shape, diameter and length on stress distribution: A finite element analysis. The Journal of Indian Prosthodontic Society, 11: 165-171. https://doi.org/10.1007/s13191-011-0095-4
[20] Li, T., Hu, K., Cheng, L., Ding, Y., Ding, Y., Shao, J., Kong, L. (2011). Optimum selection of the dental implant diameter and length in the posterior mandible with poor bone quality–A 3D finite element analysis. Applied Mathematical Modelling, 35(1): 446-456. https://doi.org/10.1016/j.apm.2010.07.008
[21] Lee, C.C., Lin, S.C., Kang, M.J., Wu, S.W., Fu, P.Y. (2010). Effects of implant threads on the contact area and stress distribution of marginal bone. Journal of Dental Sciences, 5(3): 156-165. https://doi.org/10.1016/S1991-7902(10)60023-2
[22] Winter, W., Klein, D., Karl, M. (2013). Effect of model parameters on finite element analysis of micromotions in implant dentistry. Journal of Oral Implantology, 39(1): 23-29. https://doi.org/10.1563/AAID-JOI-D-11-00221
[23] Murakami, N., Wakabayashi, N. (2014). Finite element contact analysis as a critical technique in dental biomechanics: A review. Journal of Prosthodontic Rresearch, 58(2): 92-101. https://doi.org/10.1016/j.jpor.2014.03.001
[24] Dundar, S., Topkaya, T., Solmaz, M.Y., Yaman, F., Atalay, Y., Saybak, A., Asutay, F., Cakmak, O. (2016). Finite element analysis of the stress distributions in peri-implant bone in modified and standard-threaded dental implants. Biotechnology & Biotechnological Equipment, 30(1): 127-133. https://doi.org/10.1080/13102818.2015.1083887
[25] Velmurugan, D., Alphin, M.S. (2018). Micromotion of immediately loaded zirconia dental implants for various parametric conditions: A three-dimensional finite element study. Journal of Biomaterials and Tissue Engineering, 8(7): 962-971. https://doi.org/10.1166/jbt.2018.1840
[26] Yamaguchi, Y., Shiota, M., Fujii, M., Shimogishi, M., Munakata, M. (2020). Effects of implant thread design on primary stability-A comparison between single-and double-threaded implants in an artificial bone model. International Journal of Implant Dentistry, 6(1): 42. https://doi.org/10.1186/s40729-020-00239-1
[27] Verma, S., Sharma, N., Kango, S., Sharma, S. (2021). Developments of PEEK (Polyetheretherketone) as a biomedical material: A focused review. European Polymer Journal, 147: 110295. https://doi.org/10.1016/j.eurpolymj.2021.110295
[28] Tekin, S., Değer, Y., Demirci, F.A.T.İ.H. (2019). Evaluation of the use of PEEK material in implant-supported fixed restorations by finite element analysis. Nigerian Journal of Clinical Practice, 22(9): 1252-1258. https://doi.org/10.4103/njcp.njcp_144_19
[29] Schwitalla, A.D., Spintig, T., Kallage, I., Müller, W.D. (2016). Pressure behavior of different PEEK materials for dental implants. Journal of the Mechanical Behavior of Biomedical Materials, 54: 295-304. https://doi.org/10.1016/j.jmbbm.2015.10.003
[30] Matos, J.D.M.D., Lopes, G.D.R.S., Queiroz, D.A., Pereira, A.L.J., Sinhoreti, M.A.C., Ramos, N.D.C., Lino, V., Oliveira, F.R.D., Borges, A.L.S., Bottino, M.A. (2022). Influence of the peek abutments on mechanical behavior of the internal connections single implant. Materials, 15(22): 8133. https://doi.org/10.3390/ma15228133
[31] Fabris, D., Moura, J.P., Fredel, M.C., Souza, J.C., Silva, F.S., Henriques, B. (2022). Biomechanical analyses of one‐piece dental implants composed of titanium, zirconia, PEEK, CFR‐PEEK, or GFR‐PEEK: Stresses, strains, and bone remodeling prediction by the finite element method. Journal of Biomedical Materials Research Part B: Applied Biomaterials, 110(1): 79-88. https://doi.org/10.1002/jbm.b.34890
[32] Papaspyridakos, P., Mokti, M., Chen, C.J., Benic, G.I., Gallucci, G.O., Chronopoulos, V. (2014). Implant and prosthodontic survival rates with implant fixed complete dental prostheses in the edentulous mandible after at least 5 years: A systematic review. Clinical Implant Dentistry and Related Research, 16(5): 705-717. https://doi.org/10.1111/cid.12036
[33] Sugiura, T., Yamamoto, K., Horita, S., Murakami, K., Tsutsumi, S., Kirita, T. (2017). Effects of implant tilting and the loading direction on the displacement and micromotion of immediately loaded implants: an in vitro experiment and finite element analysis. Journal of Periodontal & Implant Science, 47(4): 251-262. https://doi.org/10.5051/jpis.2017.47.4.251
[34] Abuhussein, H., Pagni, G., Rebaudi, A., Wang, H.L. (2010). The effect of thread pattern upon implant osseointegration. Clinical Oral Implants Research, 21(2): 129-136. https://doi.org/10.1111/j.1600-0501.2009.01800.x
[35] Regis, M., Bellare, A., Pascolini, T., Bracco, P. (2017). Characterization of thermally annealed PEEK and CFR-PEEK composites: Structure-properties relationships. Polymer Degradation and Stability, 136: 121-130. https://doi.org/10.1016/j.polymdegradstab.2016.12.005
[36] Velmurugan, D., Alphin, M.S. (2018). Influence of geometric design variable and bone quality on stress distribution for zirconia dental implants-A 3D finite element analysis. Computer Modeling in Engineering & Sciences, 117(2): 125-141. https://doi.org/10.31614/cmes.2018.01817