Deepak Mane | Rashmi Ashtagi* | Prashant Kumbharkar | Sandeep Kadam | Dipmala Salunkhe | Gopal Upadhye
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Melanoma mortality rate is very high and is one kind of skin cancer. So, it is essential to identify skin cancer at an initial phase hence we can minimize the mortality rate, but sometimes recognition of the skin lesion type is very difficult due to its similarity leads to wrong treatment. Hence it is required to classify the skin lesion accurately at an initial phase for medicating a patient accurately and to save their lives. Here we proposed a framework for a very precise skin lesions classification. This uses transfer learning along with a pre-trained model and MobileNet. By using our proposed system, we can categorize the different skin lesion types accurately. Lesions are divided into eight types including melanoma, benign keratosis, basal cell carcinoma, actinic keratosis, melanocytic nevus, vascular lesion, dermatofibroma, and squamous cell carcinoma. The dataset used is ISIC 2019 challenge dataset to perform experiment on types of skin lesions. If the input image is not classified in any one of the eight types, then that image is classified as an unknown image. Hence, according to experiment our proposed system able to find the lesion type very accurately and will help to dermatologist to do accurate treatment.
melanoma, types of skin cancer, classification, MobileNet
All type of skin cancer has become fatal diseases in human history. Among all, the deadliest kind of skin cancer is Melanoma. Malignant Melanoma (MM) is a sort of skin cancer, which occurs infrequently in comparison to other types of skin cancer, but has highest mortality rate. If diagnosed early, MM can be treated by removing lesions; however, if diagnosed later, the risk of death increases. As a result, an exact and precise analysis of MM is critical for any infected patient. Histological examination of a skin lesion is the most remarkable diagnosis and prognosis process. Physicians and patients, on the other hand, see it as an invasive, costly, and the time-consuming method of avoiding diagnostic skin biopsies. In the diagnosis process, a visual examination of malicious lesions and an investigation of the patterns of skin lesions are used. Non-invasive and optical dermatoscopy, when compared to a human test, allows for more accurate lesion prediction. As a result, the ability to diagnose a patient using dermatoscopy is linked to the specialized expertise of a dermatologist. As per World Health Organization (WHO), around 20 to 30 lakh cases of non-melanoma or around 132K melanoma skin cancer cases would be diagnosed worldwide annually, with skin cancer accounting for one in every three cancer cases. In the 2018 year, the overall prevalence of skin cancer (non-melanoma and melanoma both) was indeed third highest among several other cancers, including 1,329,781 new cases. Even though the melanoma wasn't as common as other skin cancers, accounting for about 1% of skin cancer cases, this makes up the bulk of skin cancer deaths [1-3].
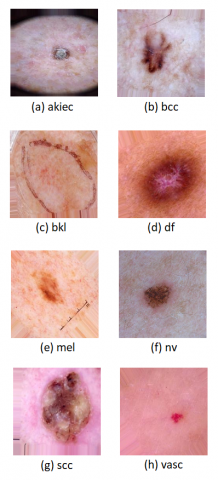
Figure 1 shows the different skin cancer types. Basically, eight skin cancer types are mentioned below. Figure 2 shows type of skin cancer classification.
Figure 1. Various types of skin cancer
Figure 2. Classification of skin lesions based on type of skin cancer
1. BCC is a cancer of lower epidermis's round cells. This kind of cell is responsible for around 80% of all skin malignancies. Basal cell carcinomas are the name given to these malignancies. Basal cell carcinoma is mostly seen on neck and head, although it may occur elsewhere on the body. It is mostly induced by sun exposure or occurs in youngsters who have undergone radiation treatment. Skin cancer of this kind develops slowly and seldom spreads to other areas of body.
2. Nevus (NV): The medical name for a mole is nevus. The average person has between 10 and 40. Common nevi are clusters of colourful cells that are completely harmless. Small brown, tan, or pink dots are the most common appearances. A common nevus is a single-colored, smooth, spherical mole.
3. Actinic keratosis, commonly known as sun keratosis, is a precancerous lesion that may progress to squamous cell carcinoma. Excessive exposure to UV rays from sun causes the disease. AKIEC may appear as a tiny, dry, scaly, or crusty skin patch. These patches may be red, tan, white, pink, flesh-toned, or a combination of these hues.
4. Dermatofibroma (DF) is a rare kind of skin cancer, which starts at middle layer of skin. A tiny lump that appears like a deep-seated pimple or a rough area of skin is typically the first symptom of DFSP. It may also mimic a scar, and in youngsters, it might appear like a birthmark.
5. Benign keratoses (BKL) are noncancerous (benign) skin growths that some individuals acquire as they become older. They are most often seen on the back or chest, although they may also be found on other areas of the body. Seborrheic keratoses are slow-growing keratoses that may develop in clusters or individually. Seborrheic keratosis affects the majority of individuals at some point in their lives.
6. Melanoma (Mel) is a malignancy of melanocytes. It is deadliest form of skin cancer.
7. Squamous cell carcinoma (SCC) is kind of skin cancer, which is induced mostly by sun exposure and may affect any part of the body. It may also appear on skin that has been burnt, chemically injured, or has been exposed to x-rays. It is most frequently seen on lips and at scar sites. Squamous cell carcinomas spread to other areas of the body in around 2% to 5% of cases, making them more prone to spread than basal cell carcinomas.
8. Vascular lesion (VASC): Three forms of vascular lesions are haemangiomas, pyrogenic granulomas, and vascular malformations. While these birthmarks may seem to be the same at times, they are distinct in terms of genesis and treatment requirements.
An early diagnosis aids to reduce mortality rate hence it requires to recognize skin cancer at an initial phase and with accurate class. Wrong classification leads to wrong treatment also leads to death hence detection of skin cancer at an initial phase with accurate class is important for appropriate treatment. Hence, the proposed system for classification of skin lesion into eight types, for that we utilized transfer learning (TL) approach along with an Improved MobileNet model.
Nowadays, one method from the branch of machine learning (ML) known as deep learning (DL) can be utilized to identify objects in images. DL is a new ML technique, quickly gaining popularity. As compared with other ML approaches, DL has a higher degree of sensitivity. The creation of a deep neural network (DNN) with a MobileNet was utilized in skin cancer classification research. Depth wise separable filters, also known as depthwise separable convolution, are foundation of MobileNet. These convolution layers that are a sort of factorized convolutional factorization, convert a standard convolution into a depthwise convolution called as a pointwise convolution. Hence presented a deep convolutional neural network with a high precision to identify skin lesions in to eight groups. The TL technique has been used with a pre-trained improved MobileNet model. Convolutional neural network (CNN) based DL offers a complete solution that accomplishes high precision without any need for feature engineering. The proposed system identifies 8 classes, these are various types of skin cancer, namely, NV, BCC, AKIEC, BKL, DF, Mel, SCC and VASC. Very limited research is available on classification of skin cancer based on dermoscopic images.
The main contribution of the proposed system is to detect type of skin cancer. The input is dermoscopic image dataset which is given to proposed mobilenet model. This classifies images into its particular skin type. The steps involved are: pre-processing, augmentation, train the system and evaluate using evaluation metrics. The dataset used is ISIC 2019 challenge training data. There are 25,331 images in the ISIC 2019 dataset. The proposed algorithm achieves the accuracy of 83.0%. By providing easier access to skin examinations based on images, we will increase our chances of detecting skin cancer in its earliest and most curable form.
Further, paper is arranged as follows: section 2 contains brief literature survey. In 3rd section system architecture, methodology and algorithms used are described; dataset description, evaluation parameters and results analysis are discussed in the 4th section, and at last, the conclusion is mentioned.
Bichakjian et al. [4] given guidelines for the cutaneous melanoma, according to authors if it is detected earlier than it can be curable. They reviewed biopsy techniques for defining the cutaneous melanoma also explained surgical and non-surgical treatments. Also summarized genetically occurred melanoma.
Apalla et al. [5] reviewed the evidences for increased skin cancer and investigated that is true or not. Authors also discussed about the challenges faced during diagnosis and complexities in creating treatment methods for cancer. For that they did some case studies and presented key case studies for highlighting the practice challenges of selecting the accurate treatment. Also, they have considered risks and advantages of increased exposure to the sun.
Khan et al. [6] proposed a system for recognizing melanoma by utilizing image processing methods. For eliminating a noise Gaussian filter is used and also utilized improved K-mean clustering for segmentation. Then extracted color and texture and utilized support vector machine for classifying melanoma from nevus skin lesions. For testing, they used DERMIS dataset which consists of cancer images.
Abdel-Zaher and Eldeib [7] presented model for enhancing the accuracy of the computer aided system (CAD) due to its utilization in diagnosis. Here authors utilized the CAD for diagnosing of a breast cancer and the deep belief network unsupervised path trailed by back propagation (BP) supervised path used. They performed a test on Wisconsin Breast Cancer Dataset (WBCD).
Zhou et al. [8] used Convolutional spiking neural networks (CSNNs) with unsupervised spike-timing-dependent plasticity (STDP) learning rule for a classification of melanoma. It classified the melanoma and benign by utilizing CSNNs and STDP learning rule. Also, they have presented feature selection for selecting the most diagnostic feature that helps to enhance the performance of classification. This enhancement helps for increasing the accuracy and efficiency of diagnosis and classification. The proposed model consists of three convolutional layers.
Using a TL method, Ashraf et al. [9] proposed Region of Interest (ROI) based model for identifying or distinguishing melanoma. ROIs are extracted from the images utilizing an enhanced k-mean algorithm. These ROI-based approaches aid in the identification of discriminative features.
Barata et al. [10] published a review on feature extraction in skin cancer dermoscopy image analysis. They've defined various kinds of features utilized in dermoscopy image analysis.
Oliveira et al. [11] investigated the computational skin lesions diagnosis from dermoscopic images by combining features based on texture analysis, colour variation, and shape properties which were derived utilizing a variety of feature extraction approaches. Different colour spaces are utilized to extract features related to colour and texture. Several classification methods, also several feature selection techniques for the classification, were used to evaluate a proposed feature extraction stage.
Pathan et al. [12] presented a study of the different techniques and algorithms utilized in CAD approach to identify pigmented skin lesions. The authors conducted a study method utilized in CAD systems, beginning with the domain aspects of melanoma and going on to the common techniques used in each treatment. The steps are pre-processing of dermoscopic images, segmentation, feature extraction and choosing of abnormal features, and relegation of skin lesion. They discussed a value of each approach used in literature, as well as the results obtained in this context. The flaws are illustrated, as well as potential study directions.
Patil and Bellary [13-17] presented methods to detect melanoma from benign, and also type and stage detection of melanoma. Mane and Kulkarni [18] suggested CCNN for Handwritten Marathi Numeral Recognition. The proposed CCNN automatically learn features and guess numeral category from a large dataset. The authors also demonstrated the simulation of the intermediate CCNN layers, which describes the dynamics of the network they described. A handwritten Marathi numerals dataset with 80000 illustrations have been organized. Furthermore, larger data collection increases the filter's weights, which improves classification accuracy even more.
Kassem et al. [19] proposed an approach using transference learning and pre-trained Google Network was developed for ISIC 2019 Challenges Data Set. Eight types of lesions were classified.
Gessert et al. [20] discuss their solution for ISIC 2019 challenge in this paper. There are two tasks in this challenge. The first task entails classifying skin lesions using dermoscopic pictures. Dermoscopic images and extra patient meta data are utilized in job 2. For both tasks, their DL-based solution came in first. With this method, they address a number of issues. First, the test set contains an unknown class that will address using a data-driven technique. Then, loss balancing attempts to correct a major class imbalance. Next, images with varying resolutions necessitate 2 separate cropping procedures as well as multi-crop evaluation. Finally, they get patient meta data that will combine with a thick neural network branch. experts use a search technique to pick an ensemble of DL frameworks, comprising EfficientNets, SENet, and ResNeXt WSL, to classify skin lesions. For training, researchers use various model input resolutions and two cropping techniques. Researchers use a loss balancing strategy to address severe class imbalance. Experts apply a data-driven strategy to forecast an additional, unknown class.
Many studies on using skin cancer images to diagnose cancer have been done. These studies included use of different machine learning techniques such as Support Vector Machines, K-Nearest Neighbours, Naive Bayes, Multi-layer perceptron, Decision Tree, Random Forest, Artificial Neural Networks, etc. Most solutions rely on a combination of techniques, such as the use of several learning functions or alternate algorithms for determining qualities. Researchers used Segmentation or mixed methods to increase classification success rate for heart sounds also performing basic pre-processing task such as noise removal, data normalization are important to improve the overall performance of model. Recently, deep neural nets have been used frequently in diagnosing skin cancer by examining images of infected lesions. Recently, Tiwari et al. [21] applied three transfer learning models on thermal breast cancer images and got significant 99% testing accuracy with VGG 16.
3.1 MobileNet
MobileNet is an image classification and the computer vision architecture model based on CNN. There are several other models, but MobileNet stands out because it runs and applies transfer learning with very little computational resources. This makes it suitable for handheld devices, embedded systems, and computers that don’t have a GPU or have low computational performance but still need to be accurate. As a result, it's particularly well-suited to web browsers, which have computational, graphic processing, and storage limitations. The dataset used is very large, using Mobilenet model time required for execution will be comparatively less.
3.1.1 Architecture of MobileNet
• MobileNets are proposed for mobile and embedded vision applications, and are based on a simplified architecture, which creates light weight deep neural networks utilizing depthwise separable convolutions.
• Two basic global hyper parameters that essentially trade off latency and accuracy are introduced. Depthwise separable filters, also known as Depthwise Separable Convolution, are foundation of MobileNet.
3.1.2 Depth wise separable convolutions
Different affiliations shall be listed in separate lines. Do not insert any punctuation at the end of each affiliation. If all the authors are affiliated to the same organization, type that affiliation just once.
Depth wise separable convolutions are referred as a kind of factorized convolution where a regular convolution is factorized it into depth wise convolution and a 1*1 convolution known also as pointwise convolution. Depth wise convolution in MobileNet put on a single filter to every input channel. After that, pointwise convolution put on a 1*1 convolution to integrate depth wise convolution's outputs. Distinction between regular convolution and depth wise separable convolution is demonstrated in the diagram (Figure 3) below.
Figure 3(a). Standard convolution filters
Figure 3(b). Depthwise convolution filters
Figure 3(c). Pointwise convolution filters
3.1.3 Advantages of using MobileNet
• MobileNet designed for enhancing the accuracy.
• MobileNet used for object detection.
3.2 Our contribution
The proposed system architecture is shown in Figure 4. The input is dermoscopic image dataset which is given to proposed mobilenet. This classifies images into its particular skin type. The proposed framework comprises of following advances:
3.2.1 Pre-processing
n from 600X450 px resolution.
Keras Image Data Generator was used to pre-process images of skin lesions. To render images consistent with the MobileNet model, images from a dataset were resized to 224X224 px resolution from 600X450 px resolution.
3.2.2 Augmentation
Data Augmentation (DA) allows for a rebalancing of the dataset’s genders, lightening other minority classes. DA is a technique for increasing number of training data by changing many constraints of the image, such as fill mode, zoom range, rotation range, vertical and horizontal flip, and so on, at random.
3.2.3 Training algorithm
We utilized MobileNet CNN, which was pre-trained on 25331 images from the ISIC 2019 Challenge containing 1,000 object groups. For the current analysis, a multi-layered MobileNet architecture was developed. Four Conv2D layers, eight Batch Normalization layers, eight ReLU layers, single DepthwiseConv2D, three ZeroPadding2D layers, Global Average Pooling, Dense layers, and Dropout are included in this collection.
Figure 4. System architecture
3.2.4 Assessment measures
Accuracy, macro average of recall, macro average of precision, and macro average of F1-score were all utilized to evaluate the model's overall results. True positive (Tp), false positive (Fp), true negative (Tn), and false negative (Fn) estimates are used to create these metrics.
(1) Accuracy: It is computed using:
Accuracy $=\frac{T_p+T_n}{T_p+T_n+F_p+F_n}$ (1)
(2) Precision: In all positive prediction cases, precision implies true positive probability. All positive predictions are true positive if the prediction is 1, but there are also the positive (+ve) samples that are wrongly predicted as negative (-ve).
Precision $=\frac{T_p}{T_p+F_p}$ (2)
(3) Sensitivity or recall is a term that can be used to describe a person's ability in comparison to Precision, Recall shows the likelihood of the forecast being truly negative (Tn) when the outcome is negative (-ve). Similarly, if recall is 1, all -ve predictions are true negatives, but there are always negative samples that are predicted as positives incorrectly.
Recall $=\frac{T_p}{T_p+T_n}$ (3)
(4) F1-score: found a happy medium between precision and recall. F1-score is a better indicator for imbalance distribution groups than precision since it focuses on true positive benefit.
$F 1=2 X \frac{\text { Precision } x \text { Recall }}{\text { Precision }+\text { Recall }}$ (4)
4.1 Description of dataset
We utilized ISIC 2019 challenge training data as a starting point. It is made up of data from the years 2017 and 2018. There are 25,331 images in the ISIC 2019 dataset that can be classified. The proposed model was tested and analysed using the ISIC 2019 challenge dataset. Images of HAM10000 and BCN 20000 can be included in the ISIC 2019 dataset. HAM10000 is a set of 1000 images, each of which is 600450 pixels in size. This dataset was from an earlier ISIC 2018 challenge. The BCN 20000, on the other hand, has 19424 images with a resolution of 1024 1024. There is an extra class named unknown class in test set that was absent in training dataset. Data is split into two parts. For training purpose, first part of dataset was utilized and for testing, second part of dataset was utilized AKIEC, MEL, BCC, NV, BKL, VASC, DF, and SCC are eight groups in ISIC 2019. ISIC 2019 has a total of 25,331 images, with each class having a different number of images (Figure 5):
Figure 5. Number of images per class
Table 1 gives detailed description of the dataset.
Table 1. Dataset description
|
Type of cancer |
Training dataset |
Testing dataset |
|
AKIEC |
853 |
996 |
|
BCC |
3261 |
89 |
|
BKL |
2506 |
139 |
|
DF |
232 |
73 |
|
MEL |
4446 |
16 |
|
NV |
2029 |
14 |
|
SCC |
609 |
9 |
|
VASC |
241 |
22 |
|
Total |
23973 |
1358 |
4.2 Experimental setup
The tests were carried out on a Windows 10 PC with an Intel Core TM i5-6200U CPU @2.30GHz, 8 GB DDRAM, and an NVIDIA GeForce 940MX graphics card. Software was run on an x64-bit Anaconda 2019.3 community version with Python 3.7. The parameter setup for implementing the MobileNet classification method is in the Table 2.
Table 2. Parameters setup of MobileNet classification
|
Number of Classes |
8 |
|
Dropout Rate |
0.25 |
|
Batch Size |
40 |
|
Learning Rate |
0.00001 |
|
Max Epoch |
6 |
|
Optimizer |
Adam |
|
Activation Function |
Softmax |
Figure 6. Accuracy and loss graphs of training and validation
4.3 Results
A comparison of the proposed model with other current methods and approaches is provided in this section. This comparison is provided under the two main phases of the proposed model, both of which this paper refers to. First, the Improved MobileNet classifier algorithm is compared to other classification algorithms. The second distinction is between the MobileNet Classifier Algorithm and the Enhanced MobileNet Classifier Algorithm. The proposed model is compared to those models and techniques that have produced the best results in recent publications and have been considered the best to date in this comparative study. The ISIC 2019 dataset was chosen.
When compared to DL models and state-of-the-art multi-class classification approaches, the experiment results clearly demonstrate that proposed TL model outperform them in multi-class MobileNet classification. Accuracy, recall, F1score, and loss are the output parameters used to compare results. Tables 1 and 2 display the effects of the proposed improved multi-class MobileNet. The proposed algorithm achieves the highest accuracy of 83.0 percent in ISIC 2019 Dataset. When compared to other Classifiers, the proposed Enhanced MobileNet transfer learning models achieve some of the lowest losses. Figure 6. shows accuracy and loss graphs of training and validation.
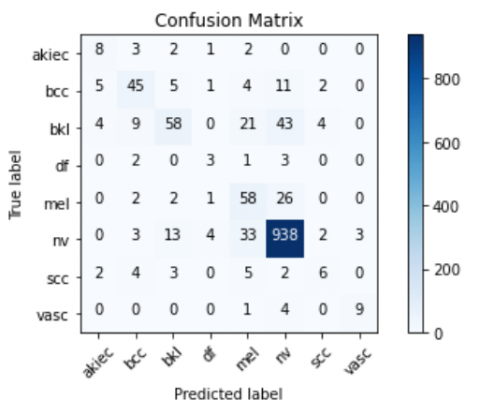
Figure 7 demonstrates the confusion matrix of 8 classes.
Figure 7. Confusion matrix
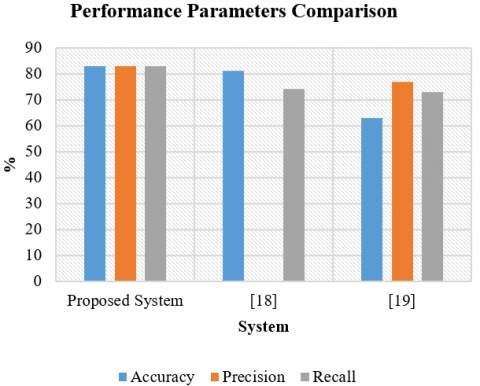
Table 3 demonstrations the precision, recall and F1-Score of each class. NV class shows the highest precision of 0.91 while DF class shows lowest precision as 0.30. Table 4 shows the macro average (mac avg) and weighted average (wtd avg) values of precision, recall and F1 score parameters of each class. Overall Accuracy of MobileNet classification is 0.8. Table 5 Shows the performance parameter comparison of similar system with proposed MobileNet with respect to precision, recall, f-measure, specificity and sensitivity and Figure 8 shows the graphical representation of performance parameters and its comparison with existing is represented in Table 5.
Table 3. Precision, recall and F1-score of each class
|
Class |
Precision |
Recall |
F1-Score |
|
Akiec |
0.42 |
0.50 |
0.46 |
|
Bcc |
0.66 |
0.62 |
0.64 |
|
Bkl |
0.70 |
0.42 |
0.52 |
|
Df |
0.30 |
0.33 |
0.32 |
|
Mel |
0.46 |
0.65 |
0.54 |
|
Nv |
0.91 |
0.94 |
0.93 |
|
Scc |
0.43 |
0.27 |
0.33 |
|
Vasc |
0.75 |
0.64 |
0.69 |
Table 4. Overall precision, recall and F1-score
|
|
Precision |
Recall |
F1-Score |
|
mac avg |
0.58 |
0.55 |
0.55 |
|
wtd avg |
0.83 |
0.83 |
0.82 |
Figure 8. Performance parameters comparison with similar system
Table 5. Comparison with existing system
|
|
Accuracy |
Precision |
Recall |
Specificity |
Sensitivity |
F-Measure |
|
[19] |
63 |
- |
73 |
- |
73 |
- |
|
[20] |
81 |
77 |
74 |
84 |
74 |
- |
|
Proposed Method |
83 |
83 |
83 |
- |
83 |
82 |
We have trained an end-to-end deep learning model in this study without any pre-processing steps or the feature handcrafting. ISIC 2019 dataset was used and we propose an updated MobileNet with a DL model for the classification of skin lesion images into eight forms of skin cancer. Our model achieved 83 percent average accuracy, outperforming dermatologists' accuracy of 81 percent, by reutilizing and adjusting architecture of pre-trained MobileNet model and using training strategies such as focal loss and class-weighted. In contrast to previous models, the outcomes obtained showed that the MobileNet model produced the best results. The MobileNet model demonstrated here is reliable and has stable performance, as well as it has faster and lighter architecture. We have worked on single dataset, further this model can be applied to other publicly available skin cancer datasets. In future work, we would like to investigate the application of our approach on other multimodal dataset.
[1] https://www.who.int/uv/faq/skincancer/en/index1.html, accessed on 5 March 2021.
[2] https://www.who.int/news-room/fact-sheets/detail/cancer, accessed on 15 March 2021.
[3] https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2020.html, accessed on 20 Feb 2021.
[4] Bichakjian, C.K., Halpern, A.C., Johnson, T.M. (2011). American academy of dermatology. Guidelines of care for the management of primary cutaneous melanoma. J Am Acad Dermatol, 65(5): 1032-1047. https://doi.org/10.1016/j.jaad.2011.04.031
[5] Apalla, Z., Nashan, D., Weller, R.B., Castellsagué, X. (2017). Skin cancer: Epidemiology, disease burden, pathophysiology, diagnosis, and therapeutic approaches. Dermatology and Therapy, 7(1): 5-19. https://doi.org/10.1007/s13555-016-0165-y
[6] Khan, M.Q., Hussain, A., Rehman, S.U., Khan, U., Maqsood, M., Mehmood, K., Khan, M.A. (2019). Classification of melanoma and nevus in digital images for diagnosis of skin cancer. IEEE Access, 7: 90132-90144. https://doi.org/10.1109/ACCESS.2019.2926837
[7] Abdel-Zaher, A.M., Eldeib, A.M. (2016). Breast cancer classification using deep belief networks. Expert Systems with Applications, 46: 139-144. https://doi.org/10.1016/j.eswa.2015.10.015
[8] Zhou, Q., Shi, Y., Xu, Z., Qu, R., Xu, G. (2020). Classifying melanoma skin lesions using convolutional spiking neural networks with unsupervised STDP learning rule. IEEE Access, 8: 101309-101319. https://doi.org/10.1109/ACCESS.2020.2998098
[9] Ashraf, R., Afzal, S., Rehman, A.U., Gul, S., Baber, J., Bakhtyar, M., Mehmood, I., Song, O.Y., Maqsood, M. (2020). Region-of-interest based transfer learning assisted framework for skin cancer detection. IEEE Access, 8: 147858-147871. https://doi.org/10.1109/ACCESS.2020.3014701
[10] Barata, C., Celebi, M.E., Marques, J.S. (2018). A survey of feature extraction in dermoscopy image analysis of skin cancer. IEEE Journal of Biomedical and Health Informatics, 23(3): 1096-1109. https://doi.org/10.1109/JBHI.2018.2845939
[11] Oliveira, R.B., Pereira, A.S., Tavares, J.M.R. (2019). Computational diagnosis of skin lesions from dermoscopic images using combined features. Neural Computing and Applications, 31(10): 6091-6111. https://doi.org/10.1007/s00521-018-3439-8
[12] Pathan, S., Prabhu, K.G., Siddalingaswamy, P.C. (2018). Techniques and algorithms for computer aided diagnosis of pigmented skin lesions—A review. Biomedical Signal Processing and Control, 39: 237-262. https://doi.org/10.1016/j.bspc.2017.07.010
[13] Patil, R., Bellary, S. (2021). Transfer learning based system for melanoma type detection. Revue d'Intelligence Artificielle, 35(2): 123-130. https://doi.org/10.18280/ria.350203
[14] Bellary, S., Patil Rashmi, R. (2017). Review: Melanoma detection & classification based on thickness using dermascopic images. International Journal of Control Theory and Applications, 10(8).
[15] Patil, R., Bellary, S. (2021). Ensemble learning for detection of types of melanoma. In 2021 International Conference on Computing, Communication and Green Engineering (CCGE), pp. 1-6. https://doi.org/10.1109/CCGE50943.2021.9776373
[16] Patil, R., Bellary, S. (2020). Machine learning approach in melanoma cancer stage detection. Journal of King Saud University-Computer and Information Sciences. https://doi.org/10.1016/j.jksuci.2020.09.002
[17] Patil, R. (2021). Machine learning approach for malignant melanoma classification. International Journal of Science, Technology, Engineering and Management-A VTU Publication, 3(1): 40-46. http://ijesm.vtu.ac.in/index.php/IJESM/article/view/691
[18] Mane, D.T., Kulkarni, U.V. (2018). Visualizing and understanding customized convolutional neural network for recognition of handwritten Marathi numerals. Procedia Computer Science, 132: 1123-1137. https://doi.org/10.1016/j.procs.2018.05.027
[19] Kassem, M.A., Hosny, K.M., Fouad, M.M. (2020). Skin lesions classification into eight classes for ISIC 2019 using deep convolutional neural network and transfer learning. IEEE Access, 8: 114822-114832. https://doi.org/10.1109/ACCESS.2020.3003890
[20] Gessert, N., Nielsen, M., Shaikh, M., Werner, R., Schlaefer, A. (2020). Skin lesion classification using ensembles of multi-resolution EfficientNets with meta data. MethodsX, 7: 100864. https://doi.org/10.1016/j.mex.2020.100864
[21] Tiwari, D., Dixit, M., Gupta, K. (2021). Deep multi-view breast cancer detection: A multi-view concatenated infrared thermal images based breast cancer detection system using deep transfer learning. Traitement du Signal, 38(6): 1699-1711. https://doi.org/10.18280/ts.380613