Zainab Y. Hussien![]() | Akram Q. Moften*
| Akram Q. Moften*![]() | Mohammed Ali Abdulrehman
| Mohammed Ali Abdulrehman![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Zirconia (ZrO₂) has emerged as a pivotal biomaterial in bone and dental repair due to its exceptional mechanical properties, including high compressive strength, crack resistance via transition toughening, and an optimal elastic modulus, alongside remarkable biocompatibility and corrosion resistance. This review highlights advancements in zirconia processing techniques—such as sintering, CAD/CAM, 3D printing, and powder processing—that enhance its microstructural integrity and mechanical performance. Clinical applications in dental restorations (crowns, bridges), orthopedic implants, and joint replacements are underscored by zirconia’s non-inflammatory, non-allergic nature, ensuring long-term safety in vivo. Despite its strengths, challenges persist in fatigue resistance and wear under cyclic loads. Future directions focus on surface modification strategies and hybrid composites to improve biointegration and durability. By addressing these limitations, zirconia is poised to expand its role in next-generation biomedical implants, balancing innovation with clinical reliability.
zirconia, green machining, sintering mechanical properties, physical properties
One transition metal is zirconium, that possesses enhanced thermal, mechanical, catalytic, and thermal properties, exhibiting significant corrosion resistance [1]. Among the five distinct isotopic forms of zirconium found in nature, 90Zr is the most prevalent, accounting for 51.45% of the total concentration. At normal temperature, zirconium dioxide (ZrO2), which is also referred to as zirconia, has a monoclinic crystal structure. The n-type semiconductor ZrO2 possesses a wide range of fascinating properties, including a high constant of dielectric, high refractive index, low thermal conductivity, ability to exchange ions, high optical transparency, low coefficient of thermal expansion, polymorphic nature, and exceptional optical and chemical properties. ZrO2 is a material of significant technological interest because of its attractive natural color, chemical stability, transformation toughness, and high strength. Additionally, it is a wonderful material that is resistant to corrosion, chemicals, and microbes at the same time [2, 3]. The atomic number of zirconium is 40, and it possesses specific physical and chemical properties that are comparable to those of titanium and other elements [4].
Given zirconia’s favorable properties and its similarity to titanium, it has found use in dentistry. Prefabricated zirconia crowns, for example, offer several advantages: high fracture resistance, low thermal conductivity, reduced technique sensitivity during cementation, and superior aesthetics. However, they also have drawbacks, including inability to be crimped for additional mechanical retention, susceptibility to discoloration, limited adaptability, higher cost, and the need for approximately 20–30% greater tooth structure reduction compared to conventional stainless steel crowns [5].
Beyond these restorative applications, in dental implantology the most commonly used alloy is Ti6Al4V, supported by extensive scientific evidence. However, alternative materials such as zirconia are now employed clinically. Zirconia implants are typically fabricated from yttria-stabilized ZrO2 via a reduction–oxidation process. Some authors report that zirconia offers superior biocompatibility and mechanical properties compared to titanium. Nevertheless, the markedly varied stiffness of zirconia and titanium implies distinct biomechanical interactions with the supporting bone. Finite element analyses have demonstrated variation in load transfer corresponding to the implant material’s modulus of elasticity [6]. Similarly, animal studies have observed varying percentages of of bone-to-implant contact for implants composed of alloys with varying elastic moduli following osseointegration [7].
In addition to dental uses, zirconium oxide is recognized as a non-hazardous, economically viable, and environmentally friendly material with broad applications [8]. Its high strength, chemical stability, and excellent high-temperature performance make ZrO2 a prime candidate for advanced ceramic materials, imparting exceptional fracture strength and toughness. In the 1980s, ZrO2 was initially used in hard tissue surgery, notably for femoral head prostheses. However, because certain ZrO2 ceramics are prone to in vivo deterioration and loss of properties, Zirconia-toughened alumina (ZTA) ceramics are the result of zirconia's current widespread use as a reinforcing phase in an alumina (Al2O3) matrix. The development of ZrO2-based composites is an alternative strategy to exploit zirconia’s outstanding capabilities without the significant drawback of in vivo deterioration [9].
In particular, zirconia’s superior biocompatibility and mechanical strength have made it a sophisticated biomaterial in medical engineering. ZrO2 has seen extensive use in dentistry for all-ceramic crowns, endosseous implants, and implant abutments. Its clinical applications also extend to orthopedics, including knee and hip prostheses, femoral heads, tibial plates, and temporary supports [10]. The microstructure of stabilized zirconia typically contains about 2.5–3.5% yttrium oxide (Y2O3) and is formed by micrometer-scale ZrO2 grains during sintering, resulting in a room temperature metastable tetragonal phase [11].
Zirconium is a transition metal with beneficial mechanical, thermal, and catalytic properties, and it is highly resistant to corrosion [1]. Among its naturally occurring isotopes, ^90Zr is the most abundant, comprising 51.45% of natural zirconium. At ambient conditions, ZrO₂ has a monoclinic crystal structure. Zirconia, an n-type semiconductor, exhibits a wide range of remarkable properties, including a high dielectric constant, optical transparency, high refractive index, ionic conductivity, low thermal conductivity, low coefficient of thermal expansion, exceptional chemical stability, and polymorphism. These features make ZrO₂ technologically significant. Zirconia is also known for its attractive natural white color, high strength, and transformation toughening behavior. It is highly resistant to corrosion, chemical attack, and microbial colonization [2, 3]. Zirconium (atomic number 40) has chemical and physical properties similar to those of titanium and other biocompatible metals [4]. Given Zirconia’s favorable properties and its similarity to titanium, it has found applications in dentistry. Prefabricated zirconia crowns, for example, offer advantages such as high fracture resistance, low thermal conductivity, reduced sensitivity to cementation technique, and superior esthetics. However, they also have drawbacks, including their inability to be crimped for additional mechanical retention, susceptibility to discoloration, limited adaptability, higher cost, and the need to remove about 20–30% more tooth structure compared to conventional stainless-steel crowns [5]. Beyond restorative dentistry, the Ti-6Al-4V alloy is the most popular material for dental implants, supported by extensive clinical evidence. However, zirconia is increasingly used as an implant material. Zirconia implants are typically made from yttria-stabilized ZrO₂ via redox processing. Some studies report that Zirconia offers superior biocompatibility and mechanical properties compared to titanium. However, the much higher stiffness (Young’s modulus) of zirconia leads to different biomechanical interactions with bone. Finite element analyses have shown differences in load transfer related to the implant’s modulus [6], and animal studies have observed variations in bone-to-implant contact after osseointegration for implants of different elastic moduli [7]. In addition to dental applications, zirconia is recognized as non-hazardous, cost-effective, and environmentally friendly [8]. Its high strength, chemical stability, and excellent high-temperature performance make ZrO₂ a prime candidate for advanced ceramic materials with exceptional fracture strength and toughness. Zirconia was first utilize in hard-tissue surgery in the 1980s, notably for femoral head prostheses. However, because some zirconia ceramics can degrade in vivo and lose their properties, zirconia is now mainly used as a reinforcing phase in an alumina (Al₂O₃) matrix, forming zirconia-toughened alumina (ZTA) composites. Developing ZrO₂-based composites is an alternative strategy to exploit zirconia’s capabilities while avoiding it’s in vivo degradation [9]. Zirconia’s superior biocompatibility and mechanical strength have established it as a valuable biomaterial in medical engineering. Zirconia is extensively used in dentistry for implant abutments, endosseous implants, and all-ceramic crowns. Its applications also extend to orthopedics, such as knee and hip prostheses, femoral heads, tibial plates, and temporary supports [10]. The microstructure of stabilized zirconia typically contains about 2.5–3.5% yttrium oxide (Y₂O₃) and is composed of micrometer-scale ZrO₂ grains formed during sintering, resulting in a metastable tetragonal phase at room temperature [11].
2.1 Physical characteristics
Zirconia is an exceptionally reliable restorative ceramic. Zirconia for dentistry resists acid erosion in the oral environment, although highly aggressive agents can affect its surface roughness. Zirconia has a coefficient of thermal expansion around 10×10−6 /℃ and very low thermal conductivity. This expansion coefficient is largely independent of the yttria content [12], because no phase transitions occur in the oral temperature range and the atomic bonding dominates thermal expansion. The bulk density of zirconia is approximately 6 g/cm³, with negligible dependence on yttria content [13].
2.2 Mechanical properties
Zirconia is the hardest material among dental ceramics, with unmatched hardness and flexural strength. For example, the biaxial flexural strength of conventional (3Y-TZP) zirconia is significantly higher than that of high-translucency (5Y-TZP) zirconia. The fracture toughness of 5Y-TZP, which contains more cubic phase, is roughly half that of 3Y-TZP [14]. The design, composition, and preparation of an implant abutment also influence zirconia’s fracture strength [15, 16]. Mechanically, zirconia behaves similarly to stainless steel, with tensile strength on the order of 900–1200 MPa and compressive strength around 2000 Mpa [17].
2.2.1 Fracture toughness and resistance to cracking
Factors such as sintering conditions, phase composition, grain size, and surface defects strongly influence zirconia’s fracture toughness. Grain-boundary engineering, Transformation toughening, and stress-induced phase transformations can increase zirconia’s resistance to crack initiation and propagation. Surface modifications (grinding, polishing, glazing) may also alter an implant’s fracture toughness and crack resistance. Indentation-based testing and standardized protocols are commonly used to evaluate these properties in zirconia biomaterials. High fracture toughness and crack resistance are critical for preventing implant failure and ensuring long-term stability in clinical applications [17].
2.2.2 Fatigue behavior and longevity
The fatigue resistance of zirconia implants depends on surface finish, implant design, material properties, and loading conditions. Cyclic loading can induce microcracks, stress concentrations, and phase transformations that contribute to fatigue failure. Aging and degradation processes (e.g., low-temperature degradation), as well as environmental factors (temperature, humidity) and surface treatments, further influence zirconia’s long-term durability. Understanding and improving the fatigue behavior of zirconia implants are essential for ensuring their long-term performance in dental applications [14].
Due to its exceptional properties and biocompatibility, zirconia has become a leading material in dental and medical applications [18]. The methods used to manufacture zirconia biomaterials significantly influence their performance in these applications.
3.1 Conventional and powder-based processing
Conventional powder processing of zirconia involves solidifying and densifying raw zirconia powder through successive steps. Usually, these procedures consist of post-sintering treatments, green machining, sintering, and powder shaping. Control of zirconia powder particle size, shape, and homogeneity during processing greatly affects the final microstructure and properties of the material [19].
3.2 Powder shaping
Powder shaping techniques, such as uniaxial and isostatic pressing, are used to form a green body from zirconia powder. In isostatic pressing, equal pressure is applied in all directions, whereas uniaxial pressing compresses the powder in one direction. These pressing methods (and other techniques like freeze granulation) influence powder compaction, green body density, and the initial microstructure. Optimizing these shaping processes is critical, since they determine the starting characteristics of zirconia (density, homogeneity, grain structure) and affect subsequent processing steps [20].
3.3 Green machining
Unfired (“green”) zirconia bodies can be machined to precise dimensions. Green machining (using CNC milling and grinding on pre-sintered zirconia blanks) enables fabrication of complex implant geometries with fine tolerance. Machining the softer green material before sintering reduces tool wear and allows intricate shapes that would be difficult to achieve after full sintering [20].
3.4 Sintering
Sintering is a critical step that strongly influences zirconia’s density and mechanical properties. Green bodies are heated to high temperatures during sintering, which results in particle diffusion and neck development. that densify the material and strengthen it. Both conventional sintering and advanced methods (spark plasma sintering, microwave sintering, and pressure less sintering) can be applied to zirconia, each affecting grain growth, porosity, and mechanical performance [21].
3.5 Post-sintering enhancements
After sintering, further treatments, such as glazing, polishing, or surface modifications may be implemented to enhance the aesthetics and optimize the material's biocompatibility [21].
3.6 Innovative Computer-Aided Design (CAD) and Computer-Aided Manufacturing (CAM) techniques
In CAD/CAM dentistry, zirconia is fabricated primarily via milling: Soft machining (pre-sintered milling): Pre-sintered zirconia blanks (sintered to a “green” state) are milled to final shape. These blanks are made by cold isostatic pressing of zirconia powder with binders and oxides, which burn out in a low-temperature pre-sintering.
Soft machining ensures high material uniformity, shorter milling time, reduced porosity (20–30 nm pores), and less tool wear. However, the design must compensate for sintering shrinkage (typically 25%) to achieve dimensional accuracy for intricate shapes.
Hard machining (fully sintered milling): Fully sintered zirconia (often prepared by hot isostatic pressing at 1400–1500℃) is milled to shape. Hard machining eliminates post-sintering shrinkage but requires longer machining time, higher cost, and increased tool wear due to the material’s hardness. The mechanical forces and heat from hard milling can induce undesirable surface transformations (e.g., formation of monoclinic phase).
Throughout these processes, controlling the zirconia grain size is crucial. Grains larger than 1 µm can promote excessive phase transformation and cracking, while grains smaller than 0.2 µm lose transformation toughening. Therefore, precise control of sintering and processing parameters is needed to achieve optimal mechanical strength and stability. Coloring can be introduced by adding metal oxides to the zirconia powder or by infiltrating milled parts with dye solutions. Multilayered zirconia blanks (with gradient coloring) are also available for esthetic dentistry. Usually, coloring has no effect on tetragonal zirconia mechanical properties, although its effect on cubic-phase zirconia is not fully understood. Zirconia dental restorations can be monolithic or veneered. Monolithic zirconia (no veneering ceramic) is more durable but less translucent than feldspathic porcelain. Layered zirconia offers superior aesthetics but is more susceptible to chipping — a common failure mode in veneered restorations [22].
Biocompatibility is the material ability to perform its intended function without eliciting adverse biological responses (inflammatory, allergic, toxic, etc.) in the host. Zirconia’s biocompatibility has been extensively studied, with evidence showing it is well tolerated by both soft and hard tissues [23, 24]. No adverse changes in the health of tissues surrounding zirconia restorations have been observed. Zirconia does not cause pseudotumor formation or teratogenesis, and it tends to promote a thin fibrous capsule similar to alumina when implanted in soft tissue. Zirconia wear particles have shown no cytotoxic effects on soft tissues. In vivo studies (e.g., implanting zirconia pellets with 6% Y₂O₃ into monkey femurs) confirm compatibility of zirconia with bone [18, 25].
Zirconia exhibits polymorphism, existing in three crystalline phases: cubic (stable above 2370 ℃), tetragonal (1170–2370℃), and monoclinic (below 1170 ℃) [26]. Partially yttria-stabilized zirconia (Y-TZP) is commonly used in orthopedic and dental applications. Under mechanical or thermal stress, metastable tetragonal grains can transform to the monoclinic phase. There is a 4-5% increase in volume along with this phase transformation [27, 28]. The resulting compressive stresses around the transformed grains impede crack growth a phenomenon known as phase transformation toughening (PTT). PTT thus provides a form of crack shielding or “self-toughening”: microcracks that would ordinarily propagate are arrested by the expanding transformed grains. However, this transformation is irreversible at ambient temperature; once a region transforms to monoclinic, it cannot further resist crack propagation at that site [29].
Low-temperature degradation (LTD), or aging, is a detrimental process closely related to PTT. In the moisture presence and at relatively low temperatures (e.g., body temperature), zirconia can gradually transform from the tetragonal to the monoclinic phase even without applied stress. This causes deterioration of mechanical properties and can eventually lead to cracking [30, 31]. LTD is influenced by factors such as surface defects, temperature, grain size , processing methods, stabilizer content, mechanical stress, and humidity (the latter two greatly accelerate aging). While aging is a potential risk for mechanical failure, a direct correlation between LTD and clinical zirconia failures has not been conclusively established. Nevertheless, LTD is known to degrade zirconia by initiating microcracks, reducing toughness, increasing surface wear and roughness, and altering optical properties [5].
Zirconia’s chemical stability and corrosion resistance are critical for implants exposed to bodily fluids. Zirconia maintains its structural integrity under physiological conditions, reducing the likelihood of adverse tissue reactions. For example, anodizing zirconium in phosphoric acid produces protective ZrO₂ films (monoclinic) that significantly lower corrosion rates compared to untreated zirconium [32]. These properties make zirconia a promising bioinert material capable of withstanding harsh biological environments [33]. Chemical resilience is therefore essential for reliability of implants and long-term durability and other medical devices.
Understanding the zirconia thermal characteristics is crucial for biomedical applications, particularly in orthopedic and dental implants subjected to temperature fluctuations. The superior thermal insulation of zirconia preserves the integrity of adjacent tissues throughout the procedure, directly influencing the biocompatibility and longevity of the implants. Research has demonstrated that thermal conductivity is affected by preparation techniques, including sol-gel processing, which modifies the particle size and morphology. Regulating these properties enhances the significance of zirconia in biomedical applications, where temperature management is essential for implant integration and performance. Enhancing these properties can markedly improve the performance of zirconia in medical applications [34].
Within the realm of biomedical applications, the aesthetic features and translucency of zirconia are of utmost importance. This is especially true in the field of dentistry, where its ability to imitate tooth enamel makes it an ideal material for orthodontic restoration. Because of their larger grain size, multilayer zirconia offers variable translucency, which promotes light transmission. Its natural translucency contributes to the enhancement of aesthetic outcomes. In contrast, monolithic zirconia has lower translucency, which is controlled by its mechanical strength and microstructural characteristics [35]. Because of these variations, careful material selection is required to strike a balance between utility and aesthetics, which will ultimately result in improved patient satisfaction and clinical outcomes.
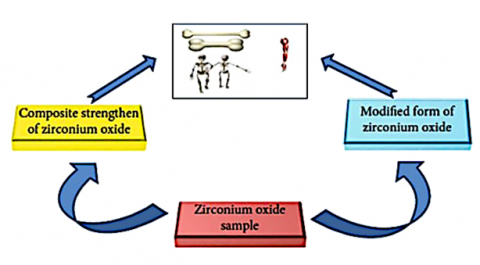
Zirconia’s inertness and mechanical strength have led to its use in various biomedical fields. Early research (1970s) focused on applications of orthopedic, such as femoral heads for total hip arthroplasty. Zirconia and zirconia-based composites are used as bone cements, bone graft substitutes, and as components in dental implants and prostheses [36]. Figure 1. Developing zirconium oxide methods for use in biological contexts. This schematic shows strategies related to orthopedic implants, hip prostheses, and bone tissue engineering [37].
Figure 1 provides a schematic representation of problem-solving strategies related to orthopedic implants, bone tissue engineering, and hip prosthesis [36].
Since the 1970s, zirconia has garnered significant attention as a biomedical material owing to its chemical and biological inertness and exceptional characteristics. Initial research on zirconia-based biomaterials focused on their orthopedic applications, particularly as femoral heads in complete hip replacements. Zirconia has since been incorporated into composites for use as bone graft substitutes, prostheses, and in dental implants and bone cements [37].
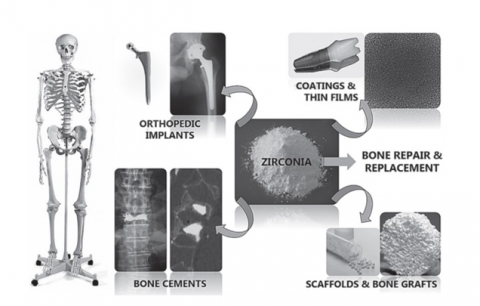
Figure 2 encompasses the utilization of zirconia bio ceramics as orthopedic implants, thin films and coatings on metallic implants, porous bone scaffolds and alternative materials, and bone cements [37].
Figure 1. Developing zirconium oxide methods for use in biological contexts
Figure 2. Biomedical applications of zirconia ceramics in contemporary bone replacement and repair procedures
Owing to the cytotoxicity and allergic reactions caused by specific metals and the growing interest in aesthetics, scientists and dentists have attempted to develop a restorative material that does not contain any metals (Figure 3). In restorative dentistry, zirconia has multiple applications, including implants, abutments, posts, cores, whole and partial crowns, bridges, inlays, onlays, and veneers [38].
Figure 3. Aesthetic rehabilitation using zirconia [38]
A paradigm shift is occurring in prosthetic dentistry, with an emphasis on all-ceramic prostheses and a departure from metal-ceramic restorations. The main motivation behind this change is the need to make prosthetic dental equipment that is more aesthetically pleasing and biocompatible. Ceramics are an important consideration for implant applications because they are more resistant to biological deterioration than metals [39, 40]. Other clinical applications of zirconia include arthroplasty and spinal fusion. Zirconia and yttria-stabilized zirconia have a variety of orthopedic applications, including dental crowns, prosthetic hips and knees, temporary supports for the hip joint, and tibial plates [41]. When ball-heads for total hip prostheses were launched in 1986, one of the main uses of yttria-stabilized zirconia began. In this field, ball-heads with yttria-stabilized zirconia bases are no longer relevant. Composite ceramics have become increasingly important. However, yttria-stabilized zirconia ceramics are widely used in dental implants and prostheses [42]. Over the last decade, 3D printing has found widespread use in many areas of dentistry, from patient treatment to dental education to research. Additionally, prosthodontics, oral implants, and oral maxillofacial surgery are among the experimental sectors that use 3D printed zirconia. Implants, abutments, scaffolds, crowns, bridges, copes, and ultra-thin occlusal veneers are a few examples. This section details the most current advancements in the use of zirconia materials for 3D printing in dentistry (Figure 4) [43].
Figure 4. Application of 3D printed zirconia materials in the field of dentistry [43]
The white hue of ZrO₂ improves aesthetics by inhibiting stains and gum discoloration, whereas its non-metallic appearance renders it suitable for patients desiring metal-free implants. ZrO₂ abutments are a favored option among implants, especially for individuals with thin gingival soft tissue [44].
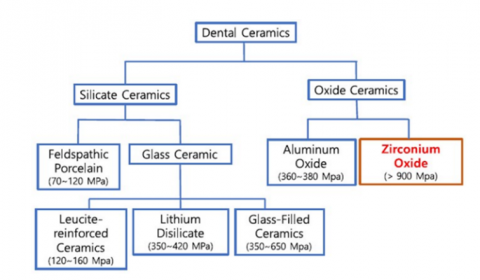
Prevalent dental ceramic systems include:
• Silica-based ceramics (SiO₂): Superb aesthetics; used for veneers and anterior crowns.
• Leucite-based ceramics KAl2[AlSi3O10](OH)2 have improved strength and resilience, making them suitable for small repairs.
• Lithium disilicate ceramics (Li₂O5Si₂): Exceptional strength and aesthetics, suitable for anterior and posterior restorations.
• Alumina-based ceramics (Al₂O₃) have high strength and wear resistance; however, they have inferior aesthetics.
• Zirconia-based ceramics (ZrO₂) exhibit exceptional strength and toughness, making them suitable for crowns, bridges, and implants. Classification of dental ceramics can be seen in Figure 5 [45].
Zirconium (Zr), discovered in 1789 by Martin Klaproth, does not occur in its elemental state but within crystals such as zircon (ZrO2・SiO2) or as a free oxide, known as zirconia (ZrO2) or baddeleyite. Zirconium oxide powder is created through meticulous processing and can subsequently be molded into zirconia blocks for many uses, including dental restorations (Figure 6) [46].
Tables 1, 2, and 3 present a summary of previous studies related to Orthopedic, Dental, and other applications relevant to this research.
Figure 5. Classification of dental ceramics with fracture strength [45]
Figure 6. The evolution of zirconia-based materials from left to right: natural zircon mineral, processed zirconium oxide powder, and final zirconia dental restorations [45]
Table 1. Research on Zirconia for industrial and other applications
|
Author |
Main Focus |
Findings |
Ref. |
|
Jose |
Investigate characteristics and applications of zirconia in diverse sectors. |
Zirconia is used in aerospace, automotive, and healthcare sectors. |
[47] |
|
Aliqba et al. |
Research biocompatibility and antenna design for biomedical devices. |
Zirconia enhances antenna performance in biomedical applications. |
[48] |
|
Takada et al. |
Improve zirconia ceramics using laser-created surface structures. |
Refined laser parameters enhance surface properties for medical devices. |
[49] |
|
Shearer et al. |
Compile research on glass-ceramics containing zirconia. |
Adding zirconia improves glass-ceramic characteristics, expanding their possibilities. |
[50] |
Table 2. Research on Zirconia for orthopedic and biomedical applications
|
Author |
Main Focus |
Findings |
Ref. |
|
Oblak et al. |
Research zirconia bioceramics' characteristics and potential medical applications. |
Y-TZP ceramics have medicinal uses due to biocompatibility and strength. |
[51] |
|
Bannunah |
Discuss medical uses of zirconia nanoparticles. |
Zirconia nanoparticles have promising uses in tissue engineering, antimicrobials, and cancer therapy. |
[3] |
Table 3. Research on Zirconia for dental applications
|
Author |
Main Focus |
Findings |
Ref. |
|
Tchinda et al. |
Develop and test a dental implant coating made of bioactive Ca-SZ on titanium. |
Dental implant uses may benefit from the Ca-SZ coating's enhanced biocompatibility. |
[52] |
|
Biju et al. |
Research dental implant materials containing spray-dried yttria stabilized zirconia. |
Uniform zirconia powders ideal for dental applications achieved by spray drying. |
[53] |
|
Gautam et al. |
Review dental ceramics made of zirconia and their uses. |
Zirconia is perfect for use in dental and orthopedic prosthetics due to biocompatibility and strength. |
[54] |
|
Manicone et al. |
Investigate zirconia’s biological characteristics and potential benefits in dental implants. |
Zirconia shows high clinical success in dental restorations with remarkable biocompatibility. |
[55] |
|
Silva et al. |
Determine zirconia’s promise for dental implants. |
These composites show promise for use in dental and orthopedic implants. |
[56] |
|
Al-Moziek et al. |
Explore the longevity and success levels of zirconia implants. |
Zirconia implants have lower success and survival rates compared to titanium implants. |
[57] |
Zirconia (ZrO₂) continues to demonstrate outstanding potential in biomedical applications due to its superior mechanical strength, corrosion resistance, and excellent biocompatibility. This review outlined the evolution of advanced manufacturing techniques—including powder processing, CAD/CAM technologies, and additive manufacturing—that have significantly improved zirconia's performance in dental and orthopedic fields. However, persistent limitations such as low-temperature degradation, limited translucency, and surface aging effects suggest areas for further research.
To enhance the clinical longevity and functionality of zirconia-based implants, future studies should explore the development of nano-engineered coatings aimed at improving surface bioactivity and wear resistance. Additionally, research into hybrid zirconia composites incorporating secondary reinforcements, such as carbon nanotubes or graphene oxide, may offer promising pathways for enhancing mechanical resilience and fatigue behavior. Moreover, the integration of functionally graded structures can provide better stress distribution and reduce the mismatch between implant and bone tissue. By addressing these aspects, the next generation of zirconia biomaterials can better meet the complex demands of biomedical environments.
All researchers involved in this article thank Mustansiriyah University and the Material Engineering Department for their support.
[1] Kaushal, S., Kumari, V., Singh, P.P. (2023). Sunlight-driven photocatalytic degradation of ciprofloxacin and organic dyes by biosynthesized rGO–ZrO2 nanocomposites. Environmental Science and Pollution Research, 30(24): 65602-65617. https://doi.org/10.1007/s11356-023-27000-6
[2] Malode, S.J., Shetti, N.P. (2022). ZrO2 in biomedical applications. In Metal Oxides for Biomedical and Biosensor Applications. Elsevier, pp. 471-501. https://doi.org/10.1016/B978-0-12-823033-6.00016-8
[3] Bannunah, A.M. (2023). Biomedical applications of zirconia-based nanomaterials: Challenges and future perspectives. Molecules, 28(14): 5428. https://doi.org/10.3390/molecules28145428
[4] Schulze, R. (2022). CBCT artefact-burden of zirconia-based as compared to titanium implants for different beam energies: An analytical approach. Scientific Reports, 12(1): 15276. https://doi.org/10.1038/s41598-022-19379-y
[5] Sabbah, A., Rady, M.A.A. (2023). Parental satisfaction, cost effectiveness and longevity of prefabricated zircon crowns versus stainless steel crowns: (A cross sectional study). Egyptian Dental Journal, 69(2): 869-876.
[6] Wille, S., Zumstrull, P., Kaidas, V., Jessen, L.K., Kern, M. (2018). Low temperature degradation of single layers of multilayered zirconia in comparison to conventional unshaded zirconia: Phase transformation and flexural strength. Journal of the Mechanical Behavior of Biomedical Materials, 77: 171-175. https://doi.org/10.1016/j.jmbbm.2017.09.010
[7] Arlucea, N., Brizuela-Velasco, A., Dieguez-Pereira, M., Punset, M., Molmeneu, M., Sánchez Lasheras, F., deLlanos-Lanchares, H., Álvarez-Arenal, Á. (2021). Zirconia vs. Titanium dental implants: Primary stability in-vitro analysis. Materials, 14(24): 7886. https://doi.org/10.3390/ma14247886
[8] Alagarsamy, A., Chandrasekaran, S., Manikandan, A. (2022). Green synthesis and characterization studies of biogenic zirconium oxide (ZrO2) nanoparticles for adsorptive removal of methylene blue dye. Journal of Molecular Structure, 1247: 131275. https://doi.org/10.1016/j.molstruc.2021.131275
[9] Palmero, P. (2019). Zirconia-based composites for biomedical applications. Bioceramics and Biocomposites: From Research to Clinical Practice, 57-85. https://doi.org/10.1002/9781119372097.ch4
[10] Heng, L., Kim, J.S., Tu, J.F., Mun, S.D. (2020). Fabrication of precision meso-scale diameter ZrO2 ceramic bars using new magnetic pole designs in ultra-precision magnetic abrasive finishing. Ceramics International, 46(11): 17335-17346. https://doi.org/10.1016/j.ceramint.2020.04.022
[11] Denry, I., Kelly, J.R. (2008). State of the art of zirconia for dental applications. Dental Materials, 24(3): 299-307. https://doi.org/10.1016/j.dental.2007.05.007
[12] Mohan, P., Yuan, B., Patterson, T., Desai, V.H., Sohn, Y.H. (2007). Degradation of yttria-stabilized zirconia thermal barrier coatings by vanadium pentoxide, phosphorous pentoxide, and sodium sulfate. Journal of the American Ceramic Society, 90(11): 3601-3607. https://doi.org/10.1111/j.1551-2916.2007.01941.x
[13] Ban, S. (2021). Classification and properties of dental zirconia as implant fixtures and superstructures. Materials, 14(17): 4879. https://doi.org/10.3390/ma14174879
[14] Kongkiatkamon, S., Rokaya, D., Kengtanyakich, S., Peampring, C. (2023). Current classification of zirconia in dentistry: An updated review. PeerJ, 11: e15669. https://doi.org/10.7717/peerj.15669
[15] Bapat, R.A., Yang, H.J., Chaubal, T.V., Dharmadhikari, S., Abdulla, A.M., Arora, S., Rawal, S., Kesharwani, P. (2022). Review on synthesis, properties and multifarious therapeutic applications of nanostructured zirconia in dentistry. RSC Advances, 12(20): 12773-12793. https://doi.org/10.1039/D2RA00006G
[16] Bethke, A., Pieralli, S., Kohal, R.J., Burkhardt, F., von Stein-Lausnitz, M., Vach, K., Spies, B.C. (2020). Fracture resistance of zirconia oral implants in vitro: A systematic review and meta-analysis. Materials, 13(3): 562. https://doi.org/10.3390/ma13030562
[17] Manicone, P.F., Iommetti, P.R., Raffaelli, L. (2007). An overview of zirconia ceramics: Basic properties and clinical applications. Journal of Dentistry, 35(11): 819-826. https://doi.org/10.1016/j.jdent.2007.07.008
[18] Singh, P.V., Reche, A., Paul, P., Agarwal, S. (2023). Zirconia facts and perspectives for biomaterials in dental implantology. Cureus, 15(10): e46828. https://doi.org/10.7759/cureus.46828
[19] Deville, S., Chevalier, J., Fantozzi, G., Bartolomé, J.F., Requena, J., Moya, J.S., Torrecillas, R., Dı́az, L.A. (2003). Low-temperature ageing of zirconia-toughened alumina ceramics and its implication in biomedical implants. Journal of the European Ceramic Society, 23(15): 2975-2982. https://doi.org/10.1016/S0955-2219(03)00313-3
[20] Grech, J., Antunes, E. (2019). Zirconia in dental prosthetics: A literature review. Journal of Materials Research and Technology, 8(5): 4956-4964. https://doi.org/10.1016/j.jmrt.2019.06.043
[21] Saridag, S., Tak, O., Alniacik, G. (2013). Basic properties and types of zirconia: An overview. World Journal of Stomatology, 2(3): 40-47.
[22] Zarone, F., Di Mauro, M.I., Ausiello, P., Ruggiero, G., Sorrentino, R. (2019). Current status on lithium disilicate and zirconia: a narrative review. BMC Oral Health, 19: 1-14. https://doi.org/10.1186/s12903-019-0838-x
[23] Alwade, F.H., Ismail, I.J., Ibrahim, F.J. (2019). Zirconia in dental and other biomedical applications: An overview. International Journal of Medical Research & Health Sciences, 8(6): 30-37.
[24] Yigit, B.S., Al-Akkad, M., Mounajjed, R. (2024). Zirconia ceramics. Acta Medica, 67(2): 39-45. https://doi.org/10.14712/18059694.2024.18
[25] Sharanraj, V., Ramesha, C.M., Kavya, K., Kumar, V., Sadashiva, M., Chandan, B.R., Naveen Kumar, M. (2021). Zirconia: As a biocompatible biomaterial used in dental implants. Advances in Applied Ceramics, 120(2): 63-68. https://doi.org/10.1080/17436753.2020.1865094
[26] Miyazaki, T., Nakamura, T., Matsumura, H., Ban, S., Kobayashi, T. (2013). Current status of zirconia restoration. Journal of Prosthodontic Research, 57(4): 236-261. https://doi.org/10.1016/j.jpor.2013.09.001
[27] Zarone, F., Russo, S., Sorrentino, R. (2011). From porcelain-fused-to-metal to zirconia: Clinical and experimental considerations. Dental Materials, 27(1): 83-96. https://doi.org/10.1016/j.dental.2010.10.024
[28] Sorrentino, R., Navarra, C.O., Di Lenarda, R., Breschi, L., Zarone, F., Cadenaro, M., Spagnuolo, G. (2019). Effects of finish line design and fatigue cyclic loading on phase transformation of zirconia dental ceramics: A qualitative micro-raman spectroscopic analysis. Materials, 12(6): 863. https://doi.org/10.3390/ma12060863
[29] Camposilvan, E., Leone, R., Gremillard, L., Sorrentino, R., Zarone, F., Ferrari, M., Chevalier, J. (2018). Aging resistance, mechanical properties and translucency of different yttria-stabilized zirconia ceramics for monolithic dental crown applications. Dental Materials, 34(6): 879-890. https://doi.org/10.1016/j.dental.2018.03.006
[30] Ferrari, M., Vichi, A., Zarone, F. (2015). Zirconia abutments and restorations: From laboratory to clinical investigations. Dental Materials, 31(3): e63-e76. https://doi.org/10.1016/j.dental.2014.11.015
[31] Mota, Y.A., Cotes, C., Carvalho, R.F., Machado, J.P., Leite, F.P., Souza, R.O., Özcan, M. (2017). Monoclinic phase transformation and mechanical durability of zirconia ceramic after fatigue and autoclave aging. Journal of Biomedical Materials Research Part B: Applied Biomaterials, 105(7): 1972-1977. https://doi.org/10.1002/jbm.b.33720
[32] Romonti, D.E., Sanchez, A.V.G., Milošev, I., Demetrescu, I., Ceré, S. (2016). Effect of anodization on the surface characteristics and electrochemical behaviour of zirconium in artificial saliva. Materials Science and Engineering: C, 62: 458-466. https://doi.org/10.1016/j.msec.2016.01.079
[33] Valiulis, A.V. (2007). The advanced structural materials for living beings implants. Journal of Vibroengineering, 9(4): 64-72.
[34] Masrol, S.R., Ibrahim, M.H.I., Adnan, S., Amir Shah, M.S.S., Main, N.M., Esa, M.F., Othman, M.H. (2015). Effect of beating process to soda anthraquinone pulp of oil palm male flower spikes fibre. Applied Mechanics and Materials, 773: 158-162. https://doi.org/10.4028/www.scientific.net/AMM.773-774.158
[35] Suleiman, M.M.A. (2022). Effect of glazes on mechanical and physical properties of various full contour zirconia materials subjected to low temperature degradation. Master's thesis, Boston University.
[36] Arshad, H.M., Shahzad, A., Shahid, S., Ali, S., Rauf, A., Sharif, S., Ullah, M.E., Ullah, M.I., Ali, M., Ahmad, H.I. (2022). [Retracted] Synthesis and biomedical applications of zirconium nanoparticles: Advanced leaps and bounds in the recent past. BioMed Research International, 2022(1): 4910777. https://doi.org/10.1155/2022/4910777
[37] Afzal, A. (2014). Implantable zirconia bioceramics for bone repair and replacement: A chronological review. Materials Express, 4(1): 1-12. https://doi.org/10.1166/mex.2014.1148
[38] Luo, F., Hong, G., Wan, Q. (2021). Artificial intelligence in biomedical applications of zirconia. Frontiers in Dental Medicine, 2: 689288. https://doi.org/10.3389/fdmed.2021.689288
[39] Denry, I.K.J.R., Kelly, J.R. (2014). Emerging ceramic-based materials for dentistry. Journal of Dental Research, 93(12): 1235-1242. https://doi.org/10.1177/0022034514553627
[40] Vijan, K. (2024). Emerging trends and clinical recommendations for zirconia ceramic crowns: A concise review. British Dental Journal, 237(1): 28-32. https://doi.org/10.1038/s41415-024-7616-0
[41] Thakare, V. (2012). Progress in synthesis and applications of zirconia. International Journal of Engineering Research and Development, 5(1): 25-28.
[42] Burger, W., Kiefer, G. (2021). Alumina, zirconia and their composite ceramics with properties tailored for medical applications. Journal of Composites Science, 5(11): 306. https://doi.org/10.3390/jcs5110306
[43] Su, G., Zhang, Y., Jin, C., Zhang, Q., Lu, J., Liu, Z., Wang, Q., Zhang, X., Ma, J. (2023). 3D printed zirconia used as dental materials: A critical review. Journal of Biological Engineering, 17(1): 78. https://doi.org/10.1186/s13036-023-00396-y
[44] Lin, H., Yin, C., Mo, A. (2021). Zirconia based dental biomaterials: Structure, mechanical properties, biocompatibility, surface modification, and applications as implant. Frontiers in Dental Medicine, 2: 689198. https://doi.org/10.3389/fdmed.2021.689198
[45] Han, M.K. (2024). Advances and challenges in zirconia-based materials for dental applications. Journal of the Korean Ceramic Society, 61(5): 783-799. https://doi.org/10.1007/s43207-024-00416-7
[46] Zhang, Y., Chen, H. X., Duan, L., Fan, J.B., Ni, L., Ji, V. (2018). A comparison study of the structural and mechanical properties of cubic, tetragonal, monoclinic, and three orthorhombic phases of ZrO2. Journal of Alloys and Compounds, 749: 283-292. https://doi.org/10.1016/j.jallcom.2018.03.253
[47] Jose, M. (2023). Zirconia: A versatile ceramic material revolutionizing industries. Bioceramics Development and Applications, 13(2): 236.
[48] Aliqab, K., Nadeem, I., Khan, S.R. (2023). A comprehensive review of in-body biomedical antennas: Design, challenges and applications. Micromachines, 14(7): 1472. https://doi.org/10.3390/mi14071472
[49] Takada, H., Narazaki, A., Yoshitomi, D., Torizuka, K., Kobayashi, Y. (2021). Optimization of laser-induced periodic surface structures formation on zirconia ceramic by ultrashort pulsed laser. Laser Applications in Microelectronic and Optoelectronic Manufacturing (LAMOM) XXVI, 11673: 116730V. https://doi.org/10.1117/12.2583379
[50] Shearer, A., Montazerian, M., Deng, B., Sly, J.J., Mauro, J.C. (2024). Zirconia-containing glass-ceramics: From nucleating agent to primary crystalline phase. International Journal of Ceramic Engineering & Science, 6(2): e10200. https://doi.org/10.1002/ces2.10200
[51] Oblak, Č., Jevnikar, P., Kosmač, T. (2013). Properties and clinical application of zirconia bioceramics in medicine. Zdravniški Vestnik, 82(12): 825-836.
[52] Tchinda, A., Didelot, A., Choquet, P., Lerebours, A., Kouitat-Njiwa, R., Bravetti, P. (2024). Innovative bioactive Ca-SZ coating on titanium dental implants: A multidimensional structural and elemental analysis. Journal of Functional Biomaterials, 15(6): 155. https://doi.org/10.3390/jfb15060155
[53] Biju, S., Sanjai, S.G., Ramaswamy, P. (2020). Study on spray-dried yttria stabilized zirconia dental implants. IOP Conference Series: Materials Science and Engineering, 988(1): 012053. https://doi.org/10.1088/1757-899X/988/1/012053
[54] Gautam, C., Joyner, J., Gautam, A., Rao, J., Vajtai, R. (2016). Zirconia based dental ceramics: Structure, mechanical properties, biocompatibility and applications. Dalton Transactions, 45(48): 19194-19215. https://doi.org/10.1039/C6DT03484E
[55] Manicone, P.F., Iommetti, P.R., Raffaelli, L., Paolantonio, M., Rossi, G., Berardi, D., Perfetti, G. (2007). Biological considerations on the use of zirconia for dental devices. International Journal of Immunopathology and Pharmacology, 20(1_suppl): 9-12. https://doi.org/10.1177/039463200702001s03
[56] Silva, V.V., Lameiras, F.S., Lobato, Z.I. (2002). Biological reactivity of zirconia–hydroxyapatite composites. Journal of Biomedical Materials Research, 63(5): 583-590. https://doi.org/10.1002/jbm.10308
[57] Al-Moziek, M.Y.A.S., AlKhouri, I., Mozayek, R.S. (2023). Success and survival rates of immediate anatomic zirconia implants: A prospective clinical and radiographic evaluation. Brazilian Journal of Oral Sciences, 22: e239183. https://doi.org/10.20396/bjos.v22i00.8669183