Alimatun Nashira*![]() | Anisa U. Rahmah
| Anisa U. Rahmah![]() | Anita Wahyuningsih
| Anita Wahyuningsih![]() | Putri R.N. Azizah
| Putri R.N. Azizah![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Very minimal risk assessment studies focus specifically on wastewater treatment plant (WWTP) operations and none on hospitals WWTP. Hospital waste contains complex chemicals and pathogenic organisms. Thus, any disruption of hospital WWTP operation is potentially very harmful to environmental health and safety. Risk management can prevent any undue effect and minimize operational mishaps, thus becoming even more critical when the amount of hospital waste increases due to the rise in bed occupancy. Hence, this study aims to assess the risk of hospital WWTP operation, with a class B hospital in Indonesia chosen as a case study. A risk register was created using a combination of safety audits, historical data, and semi-structured interviews. Failure mode and effects analysis (FMEA) were used to examine the impacts of each risk, the frequency of occurrence, and the existing detection for each failure. Based on the consequences, the risks were categorized into impacting humans, finance, the environment, or a combination of those three. After considering occurrence, severity, and detection, each risk was assigned a Risk Priority Number (RPN). The evaluation revealed 1 unacceptable risk, 14 undesirable risks, and 19 acceptable risks. Risk management methods were proposed for unacceptable and tolerated risks. The case study provides materials for the hospital management to aid in decision-making regarding the WWTP. It also contributes knowledge for WWTP benchmarking.
risk, risk assessment, wastewater, hospital wastewater treatment plant, failure mode and effects analysis (FMEA), Risk Priority Number (RPN)
Many hazardous materials, including pharmaceutically active substances and pathogenic microorganisms, are in hospital waste. Generally, hospital waste in Indonesia is categorized into three classes: hazardous solid waste, domestic solid waste, and wastewater. According to Indonesia’s regulations, only licensed agencies can treat hazardous waste. However, the wastewater has to be treated on-site until the quality fulfills the standard specified by the government in the ministry regulation [1]. Therefore, hospitals must have a wastewater treatment plant (WWTP) to ensure their effluent meets national quality standards. A deviation from their regular operation might hurt health and the environment due to the poorly treated discharge. Preventing such disruption is part of hospital risk management, which involves protection against risk activation, minimizing risk, and increasing safeguards in the event of operational deviation [2].
Risks can be identified as things that might disrupt the WWTP operation and damage WWTP assets. Some studies have identified several external risks related to WWTP operation, which include terrorism, flood, strong wind, earthquake, cyber security breaches, power outages, and absence of key personnel caused by pandemics [3]. External risks are generally more complex, but combining offensive and defensive strategies could prevent them. Some studies assessed the impact of climate changes on the efficiency of WWTP, where it was concluded that an increase in temperature affects the amount of BOD, COD, and TSS in the effluent [4, 5]. In many studies, internal risks in WWTP often come from aging infrastructure and its subsequent failure. Other common internal risks include moving parts of machinery (conveyors, impeller, screens, rakes, etc.), chemical leakage, unclear or lack of communications, height differences between surfaces, pollution, site lighting, and tripping [3, 6]. Currently, most WWTP equipment worldwide is activated automatically, making the facility's security even more essential. Every facility personnel should be aware of the movement in the area [6]. Internal risks are easier to manage as each hospital WWTP already has standard operational procedures (SOP) that minimize internal risk.
Internal risk reduction in any processing plant depends heavily on implementing the SOP, where better compliance with the work procedure must be reinforced. Operators violating safety procedures still occur now and then [3, 7]. Such a simple act of operators neglecting to secure tanks or ponds properly might result in severe consequences due to personnel falling into the tank or drowning [8]. Handling chemicals (flocculants, disinfectants) without personal protective equipment, including respiratory protection, is also a prevalent and recurring risk. Failure to follow safety procedures will cause direct contact with chemical agents being used or compounds evolved during wastewater treatment processes, such as hydrogen sulfide and methane [9]. Several accidents caused by operator negligence and non-compliance with SOP have been recorded in Malaysia [10] and Indonesia [11, 12]. Another example of internal risk is damaged electrical wires or their covers, which, when activated, can result in electric shock [13]. An employee in the WWTP facility could also be exposed to wastewater or bioaerosols [14]. This particular substance in WWTP can harm the human respiratory system, spread infectious disease, or cause acute toxic effects [15].
The professional worker in hospital WWTP, whether the operator or the supervisor, is an essential asset for the facility. They are responsible for ensuring effective and safe operation, including minimizing the risk involved. This task can be achieved with risk management, which has been proven to increase performance efficiency and contribute to innovation development [16]. In Indonesia, regulations state that every hospital has to organize its occupational health and safety program according to the national standard [17]. According to the decree, the hospital has to appoint personnel committed to managing risks, including preparing the safeguards, guidelines, and SOP for each identified risk, followed by routine monitoring, evaluation, and internal audit. Unfortunately, despite the decree, a report from the Indonesian Ministry of Labor stated that the program needed more attention from the government; thus, the implementation needed to be more timely [18]. The report also underlined that most healthcare workers possess a low understanding and commitment to implementing health and safety programs.
Health and safety programs should always start with risk identification and risk assessment. The assessment result will become the basis for implementing and safeguarding any program. There are several methods of risk assessment. The risk matrix is the most widely used qualitative risk assessment technique, and it is also classified as a semi-quantitative approach in many studies [19]. The risk matrix evaluates risk based on the probability of failure and severity of consequence and presents the risk data in simplified form. While the simplicity is attractive, it is unsuitable for highly uncertain processes and various dependencies. Another alternative to the risk matrix is Failure Method and Effects Analysis (FMEA), which identifies the probable risks that lead to failure. For each risk, three attributes—Occurrence (O), Severity (S), and Detection (D)—are considered and multiplied to form a Risk Priority Number (RPN) [20]. The FMEA method helps identify failure modes with rarer detectability, typically found in less automated and organized facilities. Conventional FMEA assumes equal weight on the 3 attributes, which is not necessarily true in real life [21]. When done comprehensively, a qualitative risk assessment is effective in broad hazard identification and has proven to aid the development of safety policies [22]. Nevertheless, the aforementioned qualitative approach study also advocates further analysis using quantitative approaches such as Fault Tree Analysis (FTA). FTA defines accident or unwanted event as the top event and systematically determines the causes. This method calculates the probability for the top event but does not evaluate the severity of the consequence [23]. Therefore, FTA is usually paired with another quantitative risk analysis technique.
The methods mentioned above have been implemented to assess the risk of WWTP operation in various parts of the world. Tušer and Oulehlová [3] studied the risk of municipal WWTP in Slovakia using the risk matrix method, while Łój-Pilch and Zakrzewska [24] used a risk map for facilities in Poland. Shinta et al. [25] investigated the risk of industrial WWTP in Indonesia using the FMEA method, while Bonab and Osgooei [26] used them in a case study of Iran municipal WWTP. Tabesh et al. [27] assessed municipal WWTP using the Fuzzy FTA method. Piadeh et al. [28] assessed industrial WWTP using the same method combined with event tree analysis. This literature shows that the existing publication focuses on municipal and industrial WWTP operations. Although no doubt every hospital with good management has assessed its WWTP operation risk, minimal work has been published in this field, especially in Indonesia. Most published risk assessments on hospital WWTP focused on health and environmental risks due to the chemicals found in hospital effluent [29]. During the pandemic, Wijaya et al. [30] analyzed the risk of waste handling in a private hospital in Indonesia. However, the research was qualitative descriptive only, by reporting interviews with several hospital personnel. Suparmadja et al. [31] had done a risk assessment on the performance of hospital WWTP using a combination of FTA and risk matrix but only focused on the effluent quality and did not consider risk on WWTP assets.
Up to date, no publication has integrated risk assessment and asset management in hospital WWTP, either in Indonesia or other countries. The lack of publication on this topic prevents hospitals from conducting benchmarking and comparative studies without face-to-face visitation. Publication data can also guide choosing and applying the risk evaluation method, making any follow-up investigation or audit easier. Therefore, the specific objective of this study is to identify and evaluate the risks of WWTP operations at a class B hospital in Indonesia and discuss their risk management.
The study included preliminary steps such as observation, document inspection, and semi-structured interviews. Based on those data, a risk assessment was synthesized focusing on the impact on effluent quality, human injury, and WWTP assets. The risk assessment results provide recommendations for undesirable and unacceptable risks to the hospital management as the basis for improving their WWTP safety and reliability.
The following section discusses the methodology applied in this case study. Defining the scope of the risk assessment is very important to ensure the risks are addressed comprehensively.
2.1 The case study background and scope
The method of this research was a case study. A risk assessment had been conducted on the operated WWTP at a class B hospital in Indonesia. Indonesian hospitals are classified as class A, B, C, and D, with criteria specified in Table 1. Higher-class hospitals are generally larger than the lower-class ones, thus having a larger number of inpatients daily. The WWTP in this study includes mechanical and biological processes, treating, on average, 160 m3 of wastewater per day in 2022-2023. The hospital had around 348 beds but exceeded them with emergency beds during the pandemic. The bed occupancy rate during 2017-2021 was 60-70%. The WWTP was operated under the sanitation unit, which manages water treatment facilities and solid waste handling.
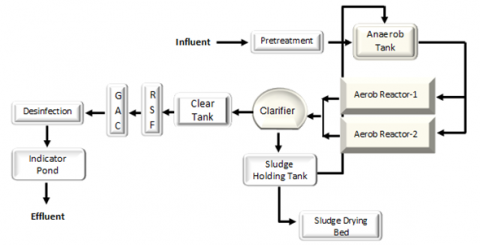
The process flow diagram for the hospital WWTP is shown in Figure 1. The treatment started from the collecting tanks, which then went to a pretreatment (equalization tank). The treatment process includes an anaerobic tank reactor, aerobic reactors, clarifier, filtration unit, and disinfecting unit. Before discharge, the water was circulated in the fish pond, a biological indicator for effluent quality. Some discharged effluent was used for watering plants, and the rest were released into a river near the hospital.
The scope of the assessment was the operation of the WWTP from the transport of influent until discharge. This included the piping and operating machinery, the activity of personnel on site, and the electrical system being used. The impact or consequence of the risk in this context was anything damaging the assets, including endangering the health and safety of humans in the immediate area of WWTP. The ecological risk was not assessed due to the complexity of ecosystem interactions and the quantification of environmental losses. Recommendations on risk management based on the risk assessment were also provided, but the actual implementation of said recommendations and their evaluation were not part of the scope.
2.2 Procedure of the risk assessment
The 3 steps in conducting risk assessment according to ISO 31000 were risk identification, risk analysis, and risk evaluation [16]. Those three were followed accordingly in this study, with the procedure displayed in Figure 2.
2.2.1 Risk identification
The risk identification was an iterative operation, meaning the risk register was reviewed and revised several times. The first step is site visitation, which was done 2 times. A WWTP operator accompanied both walkthroughs to explain every detail of the process, including operating procedure, operating condition, and equipment specification. The team also observed the operators doing their routine duties during these visits and their working conditions. The visitations gave a complete description of the process, which enabled the team to prepare the initial risk register.
The next step was the semi-structured interviews with the hospital employees whose work was related to WWTP operation and management, as shown in Table 2. The interviews provide the team with more knowledge on WWTP asset management. The team was also able to discern the concern of the WWTP workers and management regarding the risks in their workplace. Several sample questions for the interview are shown in the Appendix.
Figure 1. The process flow diagram of the hospital WWTP
Table 1. Classification of hospitals in Indonesia according to ministry of health regulation
|
Class |
Minimum Specialist Medical Service |
Number of Beds |
Minimum Supporting Facilities |
|
D |
At least 2 basic specialist medical services (2 out of internal disease, pediatric, surgery, and obstetrics-gynecology) |
At least 50 |
Laboratory, radiology, high care unit, instrument sterilization, nutrition, and pharmacy |
|
C |
Internal disease, pediatric, surgery, obstetrics-gynecology, and at least one specialist dentistry |
At least 100 |
All of the above, with anesthesiology, medical rehabilitation, clinical pathology, and intensive care unit |
|
B |
All of the above, added with at least 8 out of 13: Ophthalmology, ENT, neurology, cardiology, dermatology, pulmonology, orthopedic, urology, psychiatrist, neurosurgery, plastic surgery, and forensic medicine |
At least 200 |
All of the above |
|
A |
All of the above, 13 out of 13 specialists mentioned, and all specialist dentistry |
At least 400 |
All of the above |
Figure 2. Risk assessment as part of the risk management in WWTP, adapted from Tušer and Oulehlová [3] with modification
After the interview, the team inspected any available internal documents regarding the WWTP operation, which included characteristics of influent and effluent of wastewater, standards observed by the WWTP, accident reports, maintenance records, and previous inspection results. The previous inspection result was the internal audit performed when the WWTP failed to meet effluent criteria in 2020. The information from interviews and document inspection was used to update the risk register, where some risks were removed and some were added. The updated risk registers were then brought to the WWTP management for discussion. The management confirmed the findings and corrected any misconceptions, thus finalizing the risk register.
Table 2. Data collection activities and the informants
|
Activity |
Informant(s) |
|
Process and operational review |
Head of Sanitation Unit, WWTP operator |
|
Interview regarding health and safety in WWTP |
Head of Sanitation Unit, WWTP operator |
|
Interview regarding maintenance |
Head of Maintenance Unit |
|
Interview regarding health and safety program and risk management |
Secretary of Health and Safety Committee |
2.2.2 Risk analysis
Failure Mode and Effect Analysis (FMEA) was used to assess the registered risks. For each risk, the scenario of risk activation was prepared. Scenario is how the sequence of events unfolds, from the possible causes to how the assets were impacted. Each scenario would have 3 parameters analyzed: occurrence, severity, and detection. Occurrence (O) is the frequency of each scenario, estimated based on previous accident and equipment maintenance reports. The accident and maintenance reports were available digitally in the hospital system. Some of the occurrence values were estimated from the interview because not all events were well-documented. Severity (S) is how bad the possible consequence of each scenario. In analyzing the possible consequences, the vulnerability and value of each asset were considered. Accounts of previous accidents from the reports and interviews were used as guidance. Detection (D) is traditionally defined as the rate of failure detection, which in this work is interpreted as the availability of detection measures for each risk activation. WWTP detection measures are about risk monitoring, mentioned in the standard operating procedures and work checklist. They were crosschecked with the actual practice during the visitations.
Based on interviews with workers and safety officers, records examinations, and observations, five-level descriptors for O, D, and S were developed. Dividing the parameter into five-level descriptors is the most common practice in risk assessment in the existing literature [32, 33]. Since most risk parameter-level descriptors are qualitative, the most suitable descriptor would be developed for this study.
2.2.3 Risk evaluation
The risk evaluation was done by comparing the risk analysis results with the established risk criteria to decide the appropriate action. Risks were classified into 3 categories (acceptable, undesirable, and unacceptable) according to their Risk Priority number (RPN). The RPN was calculated using the following formula [20].
R=O × D × S
where, Occurrence (O), Severity (S), and Detection (D) in this study each have a 1-5 scale.
3.1 Risk identification and risk analysis
The risk identification stage finished with 34 risks listed in the risk register. After that, the level descriptors for occurrence, severity, and detection were developed as part of the risk analysis. This was done to obtain a descriptor best suited for the identified risks. Some risk assessment work builds their level descriptor before the risk register is finalized [22, 23], and others do that after [3, 24]. The level descriptor for occurrence, severity, and detection can be seen in Tables 3, 4, and 5, respectively. Vulnerability, monetary value, and the critical role of the impacted asset were considered while developing the impact scale. Since different risks might affect different assets in various ways, a verbal descriptor was used to describe the severity of the impact. Describing impact with verbal descriptors is common in risk assessment, especially where the consequence varies and is too complex to quantify, such as environmental loss [3]. Quantifying the impact on operator health would be significantly different than quantifying the impact on the effluent quality or impact on the operability of the equipment. Therefore, the verbal descriptor was prepared for 3 types of risk, as shown in Table 4.
While the risk matrix might be the most popular semi-quantitative risk analysis tool, only consequence and probability are assessed with this method [34]. Consequence is equivalent to severity, while probability is equivalent to occurrence within the FMEA method applied in this study. The FMEA method had another consideration: the detection (D) component. Detection (D) is the level of detection measure used to anticipate failure and risk activation. The additional component here was important because, in some small-scale setups with less automated technology, a failure could happen without the operator’s knowledge. Thus, the events occurred without documentation. This is especially true for facilities operating on tight budgets in developing countries [35, 36]. With appropriate detection measures, intervention can be done immediately, minimizing the consequence if not preventing the failure altogether. For example, the risk of overfilling an anaerobic tank can be detected with a level sensor, which, coupled with an automatic pump, would pass the wastewater into the aerobic reactor, thus avoiding flooding. While reducing space-time inside an anaerobic tank might affect the effluent quality, the consequence would be less severe than flooding the hospital ground with largely untreated wastewater. The verbal descriptor and index for detection (D) are displayed in Table 5. Better detection tools would have a low index since it means minimizing the risk.
Table 3. Occurrence probability level (O)
|
Occurrence Descriptor |
Level |
|
Once every few days or more often |
5 |
|
Once or several times a month |
4 |
|
Once or several times a year |
3 |
|
Once every few years |
2 |
|
Never but theoretically possible in several years |
1 |
Table 4. Consequence severity level (S)
|
Impact on Humans (Human Risk=H) |
Impact on Equipment or Physical Assets (Financial Risk=F) |
Impact on Effluent Quality and Discharge (Environmental Risk=E) |
|||
|
Consequence |
Score |
Consequence |
Score |
Consequence |
Score |
|
Death or Permanent Disability |
5 |
Assets need full replacement, which cannot be done immediately |
5 |
Effluent far exceeds the permittable standard, or large amounts of untreated wastewater enter the WWTP workplace |
5 |
|
Injuries resulting in weeks of lost day |
4 |
Assets need full replacement but can be done immediately (substitute available) |
4 |
Effluent slightly exceeds the permittable standard, some untreated wastewater entering the WWTP workplace, or a large amount of odorous gas discharge |
4 |
|
Injuries but less than a week lost day |
3 |
Assets need major repair |
3 |
Effluent possibly exceeds, or at the edge of the permittable standard, a small amount of wastewater enters the WWTP workplace or a small amount of odorous gas discharge |
3 |
|
Injuries impede work slightly but do not result in a lost day |
2 |
Assets need minor repair, which can be done immediately |
2 |
Effluent quality decreases but does not exceed the permittable standard, or a small amount of treated wastewater enters the WWTP workplace |
2 |
|
No impediment to work resulted |
1 |
Assets require more frequent maintenance |
1 |
Effluent quality unchanged |
1 |
Table 5. Detection level (D)
|
Detection Measure |
Level |
|
There is no detection measure at all |
5 |
|
It can be detected manually, checked once every few months |
4 |
|
It can be detected manually, checked once every few days |
3 |
|
It can be detected manually and checked daily |
2 |
|
Automatically detected |
1 |
Risk estimation was performed by determining the Risk Priority Number (RPN), which combined the occurrence value, severity, and detection. The RPN value could be anywhere from 1 to 125. The research team decided on 3 levels of risk within that interval, as displayed in Table 6. Each grouping differs in the risk mitigation required. While theoretically, the maximum value of RPN was 125, the researcher classified RPN larger than 30 as an unacceptable risk. This is because, in a more conventional risk matrix, which assumes every failure was immediately detected (or D=1), the maximum value is 25. Scores of 15 and above usually were categorized as unacceptable risk [3, 7]. In this case study, the team decided that, ideally, the score of the detection measure should be no larger than 2. Detection scores larger than 2 means failure would not be documented on that day, thus skewing the occurrence score, and by the time the impact was registered, it would be more severe. The example in this case is the risk of a larger than normal content of disinfecting substance from the hospital laundry waste (R7). Since there is no routine detection of specific substances in the influent, they can only be detected after the consequence. Some of the bacteria in the aerobic reactor would die, making the effluent quality fall below government standards. While in the hospital records, this event only happened once in 2015 before they installed a better environmentally friendly laundry system, there was a high possibility for another undocumented occurrence before the hospital found out from their monthly effluent check. Therefore, the researchers determined 30 (15 multiplied by 2) as the cut-off between undesirable and unacceptable risk scores.
3.2 Risk evaluation result
In this study, based on the RPN value, the risk was classified into 3 levels, which are acceptable, undesirable, and unacceptable (Table 6). Dividing the risk into 3 or 4 levels is common in WWTP risk assessment [3, 24, 32, 33]. Not all WWTP risk assessments categorized the risk into 3 or 4 levels; some only ranked them in a priority list [25, 26]. Another type of assessment is a probability assessment, which calculates the probability of a hazardous event based on available statistical data [27]. Previously published article has their own risk labels [3, 24, 33], with the highest level generally characterized by the need for immediate action. Table 7 lists other WWTP risk assessment methods and the main findings in the last 5 years.
This study revealed that 1 risk is unacceptable, 14 risks are undesirable, and 19 risks are acceptable. Corresponding with the definition in Table 6, the operator was recommended to take action to remove the unacceptable risk and reduce the undesirable risk. For acceptable risk, the operator was suggested to monitor the risk while maintaining their established practice routinely. Several acceptable risks would be discussed as benchmarks for other hospital WWTPs, especially if the risk had high consequences.
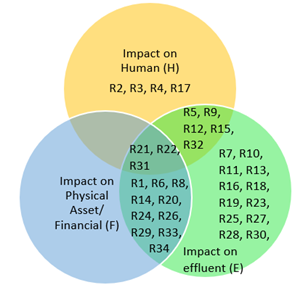
Aside from risk levels, the risks were also classified based on the impact category, as mentioned in Table 4. Some risks only affect environmental quality, physical assets, or human health, but others affect both the environment and physical assets. In a study by Łój-Pilch and Zawrezka, risks were classified into several types based on their impact: qualitative, operational, ecological, and financial [24]. A risk that fell into more types was assumed to cause more losses and, thus, would be on a higher hierarchy than a single-type risk. Meanwhile, in our study case, we still use RPN for risk ranking but observed how the impact category overlaps to determine the risk sensitivity. Figure 3 shows that most risks identified in this study impact effluent quality and discharge and thus were categorized into environmental risks. This finding agreed with Trávníček’s work, where risk analysis using an accident database found that most municipal WWTP accidents in Europe (58%) damaged the environment [37]. Four risks in this study only affect humans, which was common for occupational risks such as falls, shock, and improper PPE use. Interestingly, no found risk only affects physical assets, for every risk causing equipment damage must also impact effluent discharge and/or human health.
Every risk classified into more than one impact type had been examined more closely during the investigation. Three risks (R21, R22, R31) were classified as human, financial, and environmental. Therefore, these three risks were the most sensitive since any change would affect those 3 aspects. R21 and R22 were the fire risk and toxicity from the ozone disinfecting system. Those are new risks since the system has only been implemented for the past year to reduce another risk in the disinfecting unit. They will be addressed in-depth in the section about risk management. Meanwhile, R31 was the risk of electrical equipment short-circuiting, which has been categorized as acceptable due to the very good safeguard implemented. This will be addressed in the section about acceptable risk.
Figure 3. Risk mapping based on the impact category
Table 6. Risk ranking
|
Risk Level |
RPN |
Risk Level Descriptor |
|
Acceptable |
1-15 |
The existing risk management is sufficient to handle them and will continue to do so in the foreseeable future. No additional action is necessary. |
|
Undesirable |
16-30 |
While the current management has enough measures to handle them to minimize their impacts on assets and performance, they will probably not be enough in the future. Recommendations on risk management were provided. |
|
Unacceptable |
>30 |
Require immediate action to mitigate them. Recommendation on risk management was provided. |
Table 7. Comparison with other WWTP risk assessments in the literature
|
Object |
Method |
Risk Levels/Ranking |
Key Findings |
Ref. |
|
Municipal WWTP in Slovakia |
5×5 Risk matrix |
Negligible, Acceptable, Undesirable, Unacceptable |
|
[3] |
|
Municipal WWTP in Poland |
Risk map |
Acceptable, Tolerable, Unacceptable |
|
[24] |
|
Industrial WWTP in Indonesia |
FMEA maximum scale of 5 for Severity, Occurrence, and Detection |
Handling priority (no level classification) |
|
[25] |
|
Municipal WWTP in Iran |
Conventional FMEA method and FMEA based on Pythagorean fuzzy multiple-criteria decision-making |
Handling priority (no level classification) |
|
[26] |
|
Municipal WWTP in Iran |
Fuzzy Fault Tree Analysis and Monte Carlo Simulation |
No level classification, the result is the failure probability of the top event (inappropriate water quality and quantity) |
|
[27] |
|
Organized industrial zone WWTP in Turkey |
5x5 Risk matrix and Fuzzy risk matrix |
Low, Medium, Medium-High, High |
|
[32] |
|
Municipal WWTP based on constructed wetlands |
Three-dimensional risk matrix |
Low, Moderate, High, Very high |
|
[33] |
|
Municipal WWTPs in Europe from accident database |
Root cause analysis, Consequence analysis |
No level classification |
|
[37] |
|
Hospital WWTP in Indonesia |
FMEA maximum scale of 5 for Severity, Occurrence, and Detection |
Acceptable, Undesirable, Unacceptable |
|
This study |
3.2.1 Unacceptable risk
Unacceptable risk is the risk that requires immediate mitigation. Additional measures must be implemented since the current one is lacking. This definition is similar to other works with unacceptable risks in their ranking [3, 24]. In this study, the absence of daily parameter measurement (R28) is the only risk classified into the unacceptable category. The operator does not carry out the daily measurement because they believe it unnecessary to obtain good effluent quality. However, Indonesia’s regulation specified the obligation of each WWTP to measure the daily flow rate, pH, and temperature of the wastewater [1]. Theoretically, not complying with this law could result in the hospital permit operation being revoked or suspended after warning. In addition, there is always the potential for fluctuation in wastewater quality and quantity. Without early detection from the daily inlet measurement, the inlet will be treated as the average wastewater, resulting in inadequate processing. Unfortunately, this thinking is not `unusual for small WWTP operators due to the lack of budget or expertise [36].
This finding aligns with Shinta’s work on industrial WWTP, which stated that without daily parameter recording, it would be difficult to observe the WWTP operation continuously and might cause operational failure [25]. In the studied hospital, the importance of daily preliminary measurement was highlighted during an incident several years ago. A change in the hospital laundry department, specifically in the type of detergent and dosage, resulted in different profiles of laundry waste. The operator did not realize this until the next effluent quality measurement showed that the quality was below standard. Since effluent quality was only measured once a month—as required by government regulation—and the measurement result was received after about 2 weeks, the plant could have released this poor-quality effluent for several weeks before the laundry department was notified. This could be prevented by daily pH measurements in the pre-treatment tank for laundry waste since alteration of detergent and disinfectant dose will generally affect acidity. Enforcing daily pH measurements, temperature, and flow rate is the only solution to mitigate this risk.
3.2.2 Undesirable risk
Undesirable risks are risks that currently have existing measures to handle but still can be improved, especially because those measures might not be enough in the future. Implementing additional action will require consideration of cost-benefit evaluation [24]. The undesirable risks found in this study are listed in Table 8.
Table 8. Undesirable risks in hospital WWTP operation
|
Code |
Risk |
Cause |
Consequence |
Type |
S |
O |
D |
RPN |
|
R01 |
Operator late in doing their job |
Understaffing and overburden |
Delay in operational and handling, possible additional work required to mitigate the lateness |
E, F |
3 |
3 |
3 |
27 |
|
R04 |
Operator disregarding proper PPE use |
Lack of supervision and no sanction for the rules |
Higher exposure to wastewater and its fume, possible health consequence |
H |
2 |
5 |
3 |
30 |
|
R07 |
Too much disinfecting agent in laundry waste |
Change in the laundry unit not being consulted to WWTP |
Aerobic reactors become less effective, and effluent quality falls below the standard |
E |
5 |
2 |
3 |
30 |
|
R13 |
Ineffectiveness of bacteria in the pre-treatment tank and aerobic tank |
Bacteria was never checked nor given restarter |
Ineffective treatment, a slight drop in pollutant removal efficacy |
E |
3 |
2 |
5 |
30 |
|
R14 |
Broken or non-functional sampling port |
No sampling ports are built in closed-lid equipment such as reactors and tanks. |
Each unit cannot be evaluated separately, and troubleshooting is difficult and more costly if a problem arises |
E, F |
3 |
5 |
2 |
30 |
|
R18 |
Overloading of clarifier |
Hydraulic overloading due to higher influent or solid overloading due to high solid concentration |
The low efficiency of solid separation causes solids to carry over. The filter might be quickly saturated, and the discharge quality may decrease |
E |
3 |
3 |
2 |
18 |
|
R21 |
Fire risk in ozone disinfecting station |
Contact with flammable substances such as H2S, methane, ethanol, NH3 |
Fire damages equipment, causing process failure and harming humans in nearby areas |
H, E, F |
5 |
2 |
2 |
20 |
|
R22 |
Ozone leakage in the disinfecting station |
The contact chamber is not sealed properly. Broken piping |
Respiratory problem for personnel working at WWTP. Ozone could also harm plant life nearby and damage equipment due to its corrosive nature |
H, E, F |
4 |
1 |
5 |
20 |
|
R25 |
Late receiving the result of the effluent quality check |
Long queue in the laboratory, sending samples out of town |
Poor quality discharge went undetected |
E |
2 |
5 |
3 |
30 |
|
R26 |
Clogging of the pump in the anaerobic tank |
Larger solid waste, such as plastic, slipped away from the strainer |
Pump malfunction, anaerobic tank overfilling |
E, F |
4 |
1 |
5 |
20 |
|
R27 |
Flow meter failure |
Sludge and other debris in wastewater damage the flow meter or disturb the measurement |
The flow of wastewater cannot be measured, and dosage for chemical agents might not be accurate, causing a decrease in effluent quality |
E |
3 |
5 |
1 |
15 |
|
R29 |
Blower failure |
Ageing equipment |
Bacteria growth is not optimal, which causes a decrease in effluent quality. The blower is replaced with the spare (already available in the WWTP) |
E, F |
4 |
2 |
2 |
16 |
|
R33 |
The pump controller system malfunction |
Debris or insects disturb the sensor (without cover) or electrical current instability. |
Tank overfilling (the controller is to activate the pump when the level inside the tank reaches a certain level), discharge of untreated wastewater into the WWTP workplace |
E, F |
3 |
2 |
5 |
30 |
|
R34 |
Filtration media is being carried over |
Ageing materials and equipment, large debit of wastewater |
Filtration unit failure and decrease in effluent quality. Clogging in the next pump (to disinfecting unit) |
E, F |
4 |
2 |
2 |
16 |
Risk type based on impact categories: H (human), F (financial), E (environmental).
One of the undesirable risks was the clogging of the pump in the anaerobic tank (R26). Unwanted debris being pumped into the plant and causing equipment problems is common in water and wastewater treatment and often leads to high maintenance costs [38]. Pumping systems and pipelines are the main factors that determine the reliability of wastewater handling [39]. Hence, R26 was identified as not only environmental risk but also financial risk. Notably, this risk was initially categorized as unacceptable when the first and second risk register was drafted in late 2022. However, in 2023 the WWTP replaced the solid waste strainer in the pre-treatment tank with one stronger and finer, thus preventing the solid waste from being sucked into the pump. The previous strainer was prone to rupture and letting plastic and straw through, subsequently blocking the pump and even, on one occasion, causing the pump to short circuit. While the risk of a similar occurrence still exists, the possibility is very low; thus, the risk was deemed undesirable but not unacceptable. The pump and strainer required regular but less frequent monitoring since even the strongest strainer could be broken as the material weakened with age, prolonged exposure to wastewater, and improper handling [40, 41]. This finding is similar to the results of Tušer and Oulehlová’s [3] work, albeit, in theirs, the risks of malfunction in the pumping station were considered unacceptable. Other risk assessments on Iran municipal WWTP also stated that inappropriate pump maintenance was one of the main threats to the quality of wastewater discharge [27].
In this study, 2 other risks were found with no mitigating control. Those risks are R13 and R14. The ineffectiveness of bacteria in the pre-treatment tank and aerobic reactor (R13) was due to the inaccurate assumption that the bacteria are self-sustaining and, thus, do not require any checking and maintenance. Although with proper condition and nutrients, bacteria colonies are indeed self-sustaining, the sudden change in hospital wastewater could upset the bacteria, causing a decrease in population and effectiveness. Every WWTP that employs living microorganisms possesses this risk, with the risk level depending on the action to check and maintain the condition of the colonies. This result differs from Shinta et al.’s [25] work, where the risk of upset in the bacteria colony was deemed acceptable since the bacteria was monitored weekly in the onsite laboratory facility. The only other work that specifically mentions bacteria anomaly was Łój-Pilch and Zakrzewska’s [24], where undesired bacteria’s growth caused the upset rather than the lack of cultivated bacteria. While this differs, both papers implied the importance of monitoring bacteria’s growth.
R13 is related to lacking a functional sampling port (R14). No sampling mean there was no information on when the bacteria would require an additional restarter. For the anaerobic tank, the WWTP operator tried to circumvent this problem by recirculating part of the sludge holding tank into the anaerobic tank. The activated sludge still contains active bacteria, which can be reused to decompose organic materials in the wastewater. While some activated sludge was carried over to aerobic tanks, the total absence of monitoring and mitigation makes the risk still categorized as undesirable.
Another 2 risks (R4, R25) in the undesirable category occurred very frequently (O=5), indicating intervention in risk management was necessary. Operator disregarding proper PPE use (R4) happened almost daily due to the lax rule enforcement in the plant. During daily work, personnel only wore covered shoes and masks, while full protective equipment was worn during repair work. Several studies also reported the same risk as a recurring problem [10, 36]. Some risk assessments of WWTP operation classified this risk as unacceptable [3, 25]. They differ from this study because their establishments treat wastewater with more severe characteristics or have significantly larger capacities. Hence, the consequences of human-related accidents would be more severe.
The long waiting period to receive the effluent quality check result (R25) could harm the environment since the WWTP continuously discharges effluent while waiting. The hospital usually sends the effluent sample monthly to an external laboratory, and the results are sent back after 22-40 days. The actual measurement itself did not take that long, but more often than not, the sample had to be sent out of town, and the processing queue was very long. Another testing facility near the hospital existed, but they charged rather expensive rates. Since the national regulation itself only demanded the hospital to have monthly measurements, there was no incentive for any hospital to improve any aspect of their water testing system. This means that if the effluent does not satisfy the quality standard on some days of the month, it might be detected very late or undetected. The case is very different with industrial regulation, where many industries are equipped with on-site laboratory facilities, enabling their WWTP to monitor the effluent quality more regularly and with less waiting time, thus minimizing the risk of poor-quality discharge. However, for municipal WWTP, only the newest and largest one has an on-site laboratory [42], while no report is available on hospital WWTP.
Another undesirable risk similar to other findings is the overloading of the clarifier (R18), which was caused by a high solid concentration. The accumulation of suspended solids was considered a very high risk in Pérez et al.’s [33] work, which assessed WWTP based on constructed wetlands. This shows that the difference in WWTP technology significantly affects the severity and occurrence of similar risks. Meanwhile, conventional WWTPs with similar technology always pose the risk of equipment and infrastructure failure, which was the number one cause of accidents in European municipal WWTPs [37]. This aligns with the results of this study, where half of the undesirable risks were some types of equipment failure.
3.2.3 Acceptable risk
Acceptable risk does not require additional handling measures because the existing practice is deemed sufficient. Monitoring the risk while still maintaining current practice is still necessary. Most of the risks found in this study were classified as acceptable risk. Two of these risks (R30, R31) carried a high severity score, which could be disastrous if activated. Therefore, to be classified as acceptable implies a very good risk-handling system, which might serve as a reference in risk management for other facilities. Power outage (R30) is still a persisting risk in Indonesia's electricity grid. Despite recent improvements, the System Average Interruption Frequency Index (SAIFI) was below the national standard at an average of 5.62 times per customer per year [43]. The hospital owned several generators with enough power to cover the whole facility and circumvent this issue. During the audit, the team experienced a power outage themselves, where the WWTP generator took less than 5 seconds to power up fully, thus rendering the impact of the power outage negligible. A plant that treats a larger influx of sewage and has more electricity-driven equipment would be more affected by the lack of electricity supply. This is why, in Łój-Pilch and Zakrzewska’s [24] work, the power outage was classified as an undesirable risk.
Another example of acceptable risk was short-circuiting in the pumping system (R31), which could result in a power outage and fire. The risk was deemed acceptable despite the disastrous possible impact because the facility had a good fuse and circuit breaker. Spare equipment was also readily available if one was damaged and suspected to cause short-circuit. Based on the audit, this risk happened only once. This underlined the importance of a good electrical system in a wastewater treatment plant. This study’s result differs from Erdem’s [32] work, where all electricity-related risks were considered high. Meanwhile, Tušer and Oulehlová’s [3] study also found several electricity-related risks, with electrical shock classified as unacceptable. This difference is due to the probability or occurrence value assigned to the risk. In their study, the probability of electricity-related problems such as shock and short-circuit was high; in this study, such a thing only happened once.
3.3 Risk treatment and risk management
Part of the acceptable risks in this study (R16, R20) were a recent addition. They previously had higher RPN until modifications in 2023 successfully reduced the risk level. The best achievement in the 2023 change was the full elimination of 2 unacceptable risks related to the disinfecting process. Table 9 shows risk treatment done by the hospital in 2023 and how they reduced or eliminated the risks.
Table 9. Risk treatment that had been implemented by the hospital WWTP in 2023
|
Risk |
S |
O |
D |
RPN |
Modification |
S |
O |
D |
RPN |
|
Lamellae in the clarifier break |
4 |
2 |
2 |
16 |
Replaced with new lamellae, installed with proper inclination |
4 |
1 |
2 |
8 |
|
Clogging due to fouling in the disinfecting hose |
4 |
3 |
3 |
36 |
Replaced with ozone disinfecting system, risk of ignition |
5 |
2 |
2 |
20 |
|
Insufficient disinfecting solution in the holding tank |
5 |
3 |
3 |
45 |
Replaced with ozone disinfecting system, risk of toxicity |
5 |
1 |
4 |
20 |
|
Clogging of the pump in the anaerobic tank |
4 |
3 |
5 |
60 |
The strainer in pre-treatment was replaced with a finer and stronger one |
4 |
1 |
5 |
20 |
Table 10. Recommended safety measures to manage unacceptable and undesirable risk
|
Risk Code |
Verbal Description of the Risk |
Recommended Safety Measure |
|
R01 |
Operator late in doing their job |
Add one more personnel if the lateness is due to the overburden of work in another division, stricter adherence to operational procedure. |
|
R04 |
Operator disregarding proper PPE use |
Establishing a daily PPE checklist, which was reported to the Health and Safety Committee. Enforce sanctions or disciplinary warnings for non-compliance with the rule. Add signs to remind operators and visitors to wear PPE. |
|
R07 |
Too much disinfecting agent in laundry waste |
Daily pH measurement in each pre-treatment tank. Establish a systematic and integrated hospital logbook. |
|
R08 |
Overfilling of the anaerobic tank with sludge |
Regular inspection of sludge deposit height. Regular cleaning schedule. |
|
R13 |
Ineffectiveness of bacteria in the pre-treatment tank and aerobic tank |
Regular inspection of bacteria. Scheduling the addition of bacteria starter every few months. |
|
R14 |
Broken or non-functional sampling port |
Installation of sampling port in anaerobic and aerobic tank output pipe. |
|
R18 |
Saturation in clarifier |
Monitoring influent flow rate. Adjust operation parameters when solid contents in influent are high. Establishing a log book for the check, a log book for cleaning and maintenance, enforcing stricter record keeping. |
|
R21 |
Fire risk in ozone disinfecting station |
Sign warning of the oxidizing hazard of ozone. Put a fire extinguisher near the station. |
|
R22 |
Ozone leakage in the disinfecting station |
Sign warning of the toxicity of ozone. Wear a mask inside the area. Install an ozone detector. Ensure the chamber and pipe joints are sealed properly. Use stainless steel materials for disinfecting stations to avoid being damaged by ozone. |
|
R25 |
Late receiving the result of the effluent quality check |
Use the nearest laboratory from the hospital. Partnering with an academic institution. If possible, build an on-site laboratory. |
|
R26 |
Clogging of the pump in the anaerobic tank |
Regular inspection, cleaning, and maintenance of strainer and pump, and stricter record keeping are enforced. |
|
R28 |
Absence or incomplete daily parameter measurement |
Providing portable pH meter and calibration solution. Establishing a daily logbook, if possible, the logbook should be integrated into the computer system. Enforcing stricter record-keeping. |
|
R33 |
The pump controller system malfunction |
Regular inspection. A cover must be installed to protect the sensor and the controller from the environment. |
|
R34 |
Filtration media being carried over |
Regular inspection. Replacement of filtration media every 2 years. |
The risk treatment for the disinfecting station was to change the disinfectant from chlorine to ozone. According to the literature, ozone was more effective at killing microorganisms, required less contact time for the treatment, and did not leave behind residue that caused fouling in the hose or pipe [44]. Aside from frequent fouling, the previous disinfecting station also had the risk of running out of chlorine solution because the solution was not prepared automatically. Sometimes, the operator miscalculated the disinfectant requirement or forgot to refill the holding tank and only realized the lack of disinfecting solution during the daily check. The facility had owned ozone generator equipment for several years already but tended to opt for chlorine due to the higher cost of the ozone system. Ozone disinfecting stations still had undesirable risks due to the possibility of fire, irritant properties, and toxic effects [45]. Proper and routine maintenance of the ozone equipment was required to handle these two risks. During one of the visitations, the team observed a spark formed when the disinfecting tank was opened, indicating the presence of combustible gas inside the disinfecting tank. Fortunately, the spark died without igniting anything else on fire then. However, the incident shows that even after the modification, the disinfecting station still has undesirable risks from ozone ignition (R21) and ozone toxicity (R22). Based on the observation from implementing the ozone system for a year, the RPN was lower than that of the chlorine disinfecting system. Therefore, the modification was sufficient until better safeguards could be implemented in the future.
Another intervention was made for the lamella in the clarifying tank, which was replaced in 2023. Unlike the previous one, the new lamella was installed with the correct degree of inclination, thus improving its effectiveness. This action also reduced the likelihood of broken or clogged lamella (R20) since new equipment was typically longer-lasting.
The hospital's risk handling and interview results showed that the WWTP personnel understand the process and the risks involved. The Health and Safety program was partially implemented at the hospital in general and the WWTP in particular. In this study, the authors proposed several measures listed in Table 10 to mitigate unacceptable and undesirable risks that had not been addressed.
While the solution mostly came down to better recordkeeping and regular inspection, the implementation of these measures was inhibited by some barriers. The largest one was the lack of WWTP personnel and their overload of responsibilities. Currently, the WWTP only has two permanent staff members, but one of these two is often required to perform other duties at the hospital water treatment plant. The hospital management had already realized the human resource problem and formally stated it during the 2020 internal audit. The hospital did not regularly carry out an internal audit on its WWTP. They performed audits only when a severe accident occurred, or the monthly effluent quality measurement did not fulfill the standard criterion twice in a row. Root cause analysis was performed, and two main causes of the problem were indicated. The first was the overburden of human resources, as mentioned before, while the other was the filter malfunction, which also caused the pump to be blocked. After the audit, the filtration unit was replaced with another material, and the interviewees claimed that no incident had been observed in the filtration unit since then. Meanwhile, no change has been made to address the human resource problem. While having additional staff to lessen the personnel’s burden would certainly increase the WWTP's resilience to the operational disturbance, it was not deemed urgent enough.
Several studies with the aim of enhancing a WWTP's resilience have been published [46, 47]. WWTPs worldwide utilized different technologies, although some common equipment was often found, such as sedimentation tanks, biological reactors, and pumping systems. Aside from the technology used, technological risk also depends on the operating procedure, equipment age, maintenance, and failure rate. Appropriate selection of technology and compliance with standard operation and maintenance could reduce technological risk significantly and improve WWTP’s resilience [48]. In Poland and Slovakia, modernizing existing facilities is more common than building new ones, and the modification should be based on risk analysis [24].
The risk assessment in this case study revealed a significant share of undesirable risks. The underlying reason is the lack of detection measures due to infrequent inspection, bad record-keeping, or the absence of a sampling port and laboratory facility. These results provide materials for the hospital and WWTP management to aid decision-making regarding the facility. The hospital might increase its capacity in the future, requiring the WWTP to be more resilient. The risks evaluated as undesirable in this study might become unacceptable if the hospital capacity increases while nothing is changed in the WWTP.
The case study contributed to raising awareness of the safety and sustainability of hospital WWTP operation and presented recommendations to increase health and safety in the hospital. While insufficient data made quantitative risk assessment in this field difficult, it could be done several years in the future if consistent monitoring and detailed recordkeeping were implemented in the hospital WWTP. With more accessible data, further study incorporating simulations to evaluate risk quantitively is also open, refining the risk assessment even more.
FMEA has been implemented to analyze the identified risks, producing three risk levels: acceptable, undesirable, and unacceptable. The risk with the highest priority is the lack of daily parameter measurement. Most risk lies on acceptable level (19 risks), followed by undesirable (14 risks). This shows that the hospital has reliable risk management practices. The hospital WWTP does not require new infrastructure. Several modifications are required to mitigate the undesirable risks, including adding sampling ports, installing a cover for the sensor and controller, installing a fire extinguisher, and changing some work procedures. The assessment found that the root cause for most unacceptable and undesirable risks is a lack of record-keeping and routine monitoring. Implementing better record-keeping and monitoring practices is difficult without additional personnel or lessening the current personnel’s burden. The hospital’s safety audit result also confirmed the latter finding. The complete risk assessment results were presented to the WWTP operator and the hospital’s health and safety committee for further use, including recommendations for handling unacceptable and undesirable risks. The results of this study could also serve as a benchmark in risk assessment and management for other hospital WWTPs.
This work is supported by the grant scheme Hibah Integrasi Tridharma No. 234 /A.3-III/FT/VI/2022 from the Faculty of Engineering Universitas Muhammadiyah Surakarta.
Example of semi-structured interview questions:
1. Is the WWTP operator required to have specific training or certification?
2. What are the hazards that WWTP operators are most concerned about?
3. Is the WWTP operator required to use personal protective equipment (PPE)? Is there any disciplinary action for not using proper PPE?
4. Is there any control to ensure work instructions and SOP are followed?
5. How was any incident or accident reported and documented?
6. What device experienced the most failure or required frequent maintenance?
7. What is the procedure in the event of device failure?
[1] Menteri Lingkungan Hidup dan Kehutanan Republik Indonesia. (2016). Peraturan Menteri Lingkungan Hidup dan Kehutanan Republik Indonesia Nomor: P.68/Menlhk-Setjen/2016 Tentang Baku Mutu Air Limbah Domestik.
[2] McGowan, J., Wojahn, A., Nicolini, J.R. (2023). Risk Management Event Evaluation and Responsibilities. StatPearls Publishing, Treasure Island.
[3] Tušer, I., Oulehlová, A. (2021). Risk assessment and sustainability of wastewater treatment plant operation. Sustainability, 13: 5120. https://doi.org/10.3390/su13095120
[4] Abdulla, F., Farahat, S. (2020). Impact of climate change on the performance of wastewater treatment plant: Case study central irbid WWTP (Jordan). Procedia Manufacturing, 44: 205-212. https://doi.org/10.1016/j.promfg.2020.02.223
[5] Zouboulis, A., Tolkou, A. (2014). Effect of climate change in wastewater treatment plants: Reviewing the problems and solutions. In Managing water resources under climate uncertainty: Examples from Asia, Europe, Latin America, and Australia, pp. 197-220. https://doi.org/10.1007/978-3-319-10467-6_10
[6] Falakh, F., Setiani, O. (2018). Hazard identification and risk assessment in water treatment plant considering environmental health and safety practice. E3S Web of Conferences, 31: 06011. https://doi.org/10.1051/e3sconf/20183106011
[7] Junaidi, S., Fatoni, R., Fatimah, S. (2020). The analysis of occupational safety and health of the batik industry. Advance Sustainable Science, Engineering and Technology, 2(1): 0200101. https://doi.org/https://doi.org/10.26877/asset.v2i1.6016
[8] Hauser, A., Sathrugnan, K., Roedler, F. (2015). Managing risks in advanced wastewater treatment plants. Water Practice and Technology, 10(2): 305-311. https://doi.org/10.2166/wpt.2015.036
[9] Corrao, C.R.N., Mazzotta, A., La Torre, G., De Giusti, M. (2012). Biological risk and occupational health. Industrial Health, 50: 326-337. https://doi.org/10.2486/indhealth.MS1324
[10] DOSH. (2023). Fatal accident case. Malaysia Department of Occupational Safety and Health. https://www.dosh.gov.my/index.php/component/content/article/352-oshinfo/accident-case/955-accident-case, accessed on Oct. 6, 2023.
[11] Tanjung, I., Utomo, A.P. (2023). Jatuh ke Dalam Kontainer Limbah di PT Pertamina Hulu Rokan, 3 Pekerja Tewas. Kompas, Pekanbaru. https://regional.kompas.com/read/2023/02/25/092730078/jatuh-ke-dalam-kontainer-limbah-di-pt-pertamina-hulu-rokan-3-pekerja-tewas, accessed on Oct. 6, 2023.
[12] Flora, M. (2017). 7 Jasad Pekerja Korban Limbah Beracun Berhasil Dievakuasi. Liputan 6. https://www.liputan6.com/news/read/3113938/7-jasad-pekerja-korban-limbah-beracun-berhasil-dievakuasi, accessed on Oct. 6, 2023.
[13] Łój-Pilch, M., Zakrzewska, A., Zielewicz, E. (2018). Impact of human factors on threats in sewage treatment plants. Safety and Reliability – Safe Societies in a Changing World, CRC Press, London, 1933-1938. https://doi.org/10.1201/9781351174664-242
[14] Verani, M., Federigi, I., Donzelli, G., Cioni, L., Carducci, A. (2019). Human adenoviruses as waterborne index pathogens and their use for quantitative microbial risk assessment. Science of The Total Environment, 651: 1469-1475. https://doi.org/10.1016/j.scitotenv.2018.09.295
[15] Mao, K., Zhang, K., Du, W., Ali, W., Feng, X., Zhang, H. (2020). The potential of wastewater-based epidemiology as surveillance and early warning of infectious disease outbreaks. Current Opinion in Environmental Science & Health, 17: 1-7. https://doi.org/10.1016/j.coesh.2020.04.006
[16] International Organization for Standardization. (2018). Risk Management - Guidelines. ISO Standard No. 31000:2018.
[17] Menteri Kesehatan, RI (2016). Peraturan Menteri Kesehatan Republik Indonesia Nomor 66 Tahun 2016 Tentang Keselamatan dan Kesehatan Kerja Rumah Sakit. Kementerian Kesehatan Republik Indonesia.
[18] Kementerian Ketenagakerjaan RI. (2022). Profil Keselamatan dan Kesehatan Kerja Nasional Indonesia Tahun 2022.
[19] Khan, F.I., Amyotte, P.R., Amin, M.T. (2020). Advanced methods of risk assessment and management: An overview. Methods in Chemical Process Safety, 4: 1-34. https://doi.org/10.1016/bs.mcps.2020.03.002
[20] Sharma, R.K., Kumar, D., Kumar, P. (2005). Systematic failure mode effect analysis (FMEA) using fuzzy linguistic modelling. International Journal of Quality & Reliability Management, 22: 986-1004. https://doi.org/10.1108/02656710510625248
[21] Bhattacharjee, P., Dey, V., Mandal, U.K. (2020). Risk assessment by failure mode and effects analysis (FMEA) using an interval number based logistic regression model. Safety Science, 132: 104967. https://doi.org/10.1016/j.ssci.2020.104967
[22] Rbeht, D., El-Ali Al-Waqfi, M.S., Al-Jarrah, J. (2023). Qualitative risk assessment in water bottling production: A case study of Maan Nestlé Pure Life Factory. International Journal of Safety and Security Engineering, 13: 1025-1038. https://doi.org/10.18280/ijsse.130605
[23] Kumar, M. (2023). An α-cut interval-based similarity aggregation method to evaluate fault tree events for system safety under fuzzy environment. In Engineering Reliability and Risk Assessment, 185-200. https://doi.org/10.1016/B978-0-323-91943-2.00002-2
[24] Łój-Pilch, M., Zakrzewska, A. (2020). Analysis of risk assessment in a municipal wastewater treatment plant located in upper Silesia. Water, 12(1): 23. https://doi.org/10.3390/w12010023
[25] Shinta, F.R., Karnaningroem, N., Mardyanto, M.A. (2019). Risk management of wastewater treatment in the wastewater treatment plant of PT. X. IPTEK Journal of Proceedings Series, (5): 140-149. https://doi.org/10.12962/j23546026.y2019i5.6292
[26] Bonab, S.R., Osgooei, E. (2022). Environment risk assessment of wastewater treatment using FMEA method based on Pythagorean fuzzy multiple-criteria decision-making. Environment, Development and Sustainability, 1-31. https://doi.org/10.1007/s10668-022-02555-5
[27] Tabesh, M., Roozbahani, A., Hadigol, F., Ghaemi, E. (2022). Risk assessment of water treatment plants using fuzzy fault tree analysis and Monte Carlo simulation. Iranian Journal of Science and Technology, Transactions of Civil Engineering, 46: 643-658. https://doi.org/10.1007/s40996-020-00498-3
[28] Piadeh, F., Ahmadi, M., Behzadian, K. (2018). Reliability assessment for hybrid systems of advanced treatment units of industrial wastewater reuse using combined event tree and fuzzy fault tree analyses. Journal of Cleaner Production, 201: 958-973. https://doi.org/10.1016/j.jclepro.2018.08.052
[29] Parida, V.K., Sikarwar, D., Majumder, A., Gupta, A.K. (2022). An assessment of hospital wastewater and biomedical waste generation, existing legislations, risk assessment, treatment processes, and scenario during COVID-19. Journal of Environmental Management, 308: 114609. https://doi.org/10.1016/j.jenvman.2022.114609
[30] Wijaya, H., Alwi, M.K., Baharuddin, A. (2021). Analisis risiko keselamatan dan kesehatan kerja (K3) kalam pengelolaan limbah medis rumah sakit Islam hasanah muhammadiyah mojokerto di masa pandemi COVID-19. Journal of Muslim Community Health, 2(1): 36-51. https://doi.org/10.52103/jmch.v2i1.487
[31] Suparmadja, A., Karnaningroem, N. (2015). Analisis risiko dan optimasi kinerja ipal rumah sakit menggunakan metode fault tree analysis (FTA). Institut Teknologi Sepuluh Nopember.
[32] Erdem, F. (2022). Risk assessment with the fuzzy logic method for Ankara OIZ environmental waste water treatment plant. Turkish Journal of Engineering, 6: 268-275. https://doi.org/10.31127/tuje.975623
[33] Pérez, Y., García-Cortes, D., Torres-Valle, A., Jáuregui-Haza, U. (2023). Risk assessment of domestic wastewater treatment system based on constructed wetlands. Sustainability, 15: 15850. https://doi.org/10.3390/su152215850
[34] Vatanpour, S., Hrudey, S., Dinu, I. (2015). Can public health risk assessment using risk matrices be misleading? International Journal of Environmental Research and Public Health, 12: 9575-9588. https://doi.org/10.3390/ijerph120809575
[35] Patel, J. (2019). Difficulties of recording and notification of accidents and diseases in developing countries. https://www.ilo.org/resource/difficulties-recording-and-notification-accidents-and-diseases-developing.
[36] Cossio, C., McConville, J., Rauch, S., Wilén, B.M., Dalahmeh, S., Mercado, A., Romero, A.M. (2018). Wastewater management in small towns – understanding the failure of small treatment plants in Bolivia. Environmental Technology, 39(11): 1393-1403. https://doi.org/10.1080/09593330.2017.1330364
[37] Trávníček, P., Junga, P., Kotek, L., Vítěz, T. (2022). Analysis of accidents at municipal wastewater treatment plants in Europe. Journal of Loss Prevention in the Process Industries, 74: 104634. https://doi.org/10.1016/j.jlp.2021.104634
[38] Nadya, A., Faieza, A.A., Norzima, Z., Ismail, H. (2015). Design and development of new debris strainer in water treatment plant. Procedia Computer Science, 76: 209-216. https://doi.org/10.1016/j.procs.2015.12.344
[39] Skibo, D.V, Kunitsyn, A.G., Chupin, V.R. (2021). Analysis of the wastewater treatment device for the damper tank of sewage pumping stations. IOP Conference Series: Earth and Environmental Science, 751: 012124. https://doi.org/10.1088/1755-1315/751/1/012124
[40] Rajani, B., Kleiner, Y. (2001). Comprehensive review of structural deterioration of water mains: physically based models. Urban Water, 3: 151-164. https://doi.org/10.1016/S1462-0758(01)00032-2
[41] Shamsudin, S.R., Harun, M., Mohd Salleh, M.A.A., Yazid, H., Mazlee, M.N. (2013). Failure investigation on rusty mesh strainer of petrochemical plant. Advanced Materials Research, 795: 488-391. https://doi.org/10.4028/www.scientific.net/AMR.795.488
[42] Ferráns, L., Caucci, S., Cifuentes, J., Avellán, T., Dornack, C., Hettiarachchi, H. (2018). Wastewater management in the basin of lake Atitlan: A background study. Dresden. https://doi.org/10.53325/HNHV6581
[43] PT PLN Persero. (2022). Lampaui Target, PLN Sukses Turunkan Gangguan Listrik Lebih dari 25 Persen di 2022.
[44] Tripathi, S., Hussain, T. (2022). Water and wastewater treatment through ozone-based technologies. In Development in Wastewater Treatment Research and Processes, 139-172. https://doi.org/10.1016/B978-0-323-85583-9.00015-6
[45] U.S. EPA. (1999). Wastewater Technology Fact Sheet: Ozone Disinfection [Fact sheet]. EPA 832-F-99-063.
[46] Pamidimukkala, A., Kermanshachi, S., Adepu, N., Safapour, E. (2021). Resilience in water infrastructures: A review of challenges and adoption strategies. Sustainability, 13(23): 12986. https://doi.org/10.3390/su132312986
[47] Ba-Alawi, A.H., Ifaei, P., Li, Q., Nam, K., Djeddou, M., Yoo, C. (2020). Process assessment of a full-scale wastewater treatment plant using reliability, resilience, and econo-socio-environmental analyses (R2ESE). Process Safety and Environmental Protection, 133: 259-74. https://doi.org/10.1016/j.psep.2019.11.018
[48] Butler, D., Ward, S., Sweetapple, C., Astaraie‐Imani, M., Diao, K., Farmani, R., Fu, G. (2017). Reliable, resilient and sustainable water management: the Safe & SuRe approach. Global Challenges, 1(1): 63-77. https://doi.org/10.1002/gch2.1010