OPEN ACCESS
In hospitals, the requirements relating at comfort thermo-hygrometric, lighting and air quality, play a major role and are related, at the characteristics of the building-plant system, and to the activities that take place in it. The climate control of the environments constitutes a major problem in the hospital field, and it has effects not only in the realization of new facilities, but also in the renovations. The systems must be designed and engineered with a full integration with the global project, which is simple in the case of new construction, more difficult in the event of restructuring, since it is necessary to interact with restrictive constraints conditioning, such a distribution of complex and articulated spaces. In design of the systems of a hospital building, two fundamental aspects must be ensured: total control of the thermo-hygrometric parameters (temperature, humidity and air velocity), and the possibility of the control and adjusting -for the single areas- of flows and air changes within individual rooms. The conditioning systems of the hospitals are supposed to represent the state of arts, in terms of technological research and energy savings, maintaining overall the highest level of welfare, for operators and user. In fact, less than half of modern health facilities are newly built and only 34% have been completed after 1971. In addition, from specific regulatory perspective, for air-conditioning systems in hospital buildings, in Italy there is no real legislative/regulatory corpus. Therefore the legislation is very limited, and for the reasons set out above, in this paper will reported the studies carried out at a hospital in the city of Messina, for evaluating the indoor global comfort conditions through the feedback of appropriate quality indices: temperature, humidity and air velocity, lighting and air quality. For the evaluation of hygrothermal comfort conditions is used the model suggested by the ISO 7730 standard.
thermo-hygrometric comfort, illuminance, IAQ, ISO7730, UNI10339, UNI8199
The Italian hospitals are housed in old buildings, some statistics report refers which they have should be about of fifty years old. Recently new structures were built, but the trend is that over restructure and/or redevelop existing buildings, making by a cost-benefit analysis that supports this choice. The Italian construction industry covers the most part of the national energy requirements, and the hospital have a big energy request because the buildings of different areas with different destinations represent the major demand of the needed energy sector.
Hospitals must observe the same climate conditions, although the average fuel consumption is three times more than the average values of the residential construction sector.
The energy demand in this sector have been used in different way: air conditioning in summer and winter, ventilation, environments lighting, domestic hot water, steam generation for sterilization and humidification, as well as the request by the kitchens, laundries, domestic transport, computers, diagnostic and therapeutic devices, etc.
Furthermore, this demand should be absolutely guaranteed, in particular for the thermal and electrical installations, for everyday of the year.
The complexity of the equipment used and the regulatory compliance in terms of temperature, humidity and air flow, it could lead considerable consumption, increasing the difficulty of management plants.
However, the hospital buildings have a large energy savings potential, which could be achieved improving efficiency of building-plant systems, management of energy.
The air conditioning systems of the hospitalization facility should meet specific technical and functional requirements in order to ensure compliance with the temperature-humidity requirements of itself.
The regulatory and legislative system should pay attention to the standards and the eligibility criteria for these environments, such as the rooms to be used as hospital stays, providing a strategy to obtain higher values of comfort and safety.
The most important legal instrument currently used in Italy is the Presidential Decree 14/01/97 [1] laying down the structural, technological and organizational requirements for the exercise of medical activities either public and private structures [2, 3]
The healthcare facilities comfort varies considerably by depending on the hospitals and the wrong design, compared to the effective use of seasonal conditioning system, which could generate phenomena discomfort quite marked too. Analysis of this particular type of environments, in addition to the overall discomfort, should focus on localized discomfort phenomena. The operating condition systems are sometimes cause of easily predictable situations, but not easily avoidable, such as the risk of air currents, best defined as Draft Risk [4] and the asymmetry by means radiant temperature, which often is aggravated by orientation of the same structure [5-11].
This paper would report the studies carried out at the hospital in the city of Messina, looking forward a real quality temperature and humidity index of the rooms designed to hospitalization.
The experimental campaign for the detection of environmental parameters was conducted at a hospital located in the north of the city of Messina, with its complex and articulated architectural structure.
To perform monitoring has been chosen for each department a "room-type", representative of the whole department that have different exposure and orientation conditions.
Moreover, by studying the external building coating, of our case-study, using thermographic equipment, it was decided to pay attention on two rooms-stay types chosen from those previously analyzed.
We did the energy classification of these environments, and propose some design solutions for the entire hospital, in order to improve the energy efficiency.
The rules and laws for the health care facilities design are numerous and cover various fields of application, for the complexity and importance of the social structure and the situation of their users.
Environmental health conditions are linked to the room conditioning, and can be obtained by monitoring these parameters: temperature, humidity and air velocity and concentration of pollutants (bacteria, medical gases, etc.).
These parameters define the air quality and its control is done indirectly through: the ventilation rates or if it is necessary filtering it, specific conditions of pressure and temperature, eligibility of air recirculation flows inside the room.
Subsequent references to legislation, are therefore limited to these aspects, important for the comfort and for the achievement of the objective in health facility.
The current Italian legislation for thermo-hygrometric comfort in health facilities is based mainly on two reference laws: The Circular of the Ministry of Public Works of 11.22. 1974, n.13011, and the Presidential Decree of 1.14.1997.
The first, which was the only one for many years, consists on a short paper entitled "Physical-Technical requirements for hospital building constructions - Thermal properties, humidity, ventilation and lighting."
The second, is the DPR, set the minimum requirements for the pursuit of health, to fill this regulatory gap, provide detailed technical information necessary for the design of the plant and the building.
Specific technical regulations governing the various sectors: the principal of our interest is the UNI10339, which provides technical data such as result of Circular 13011, about ventilation and devices to ensure good air quality.
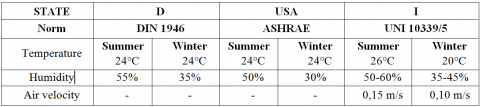
In Tab. 1a below, shows the values indicated by the International and National Standards.
The UNI/TS 11300-2, provides plausible values, requests for domestic hot water, by hospitals, and next methods of primary energy demand calculation.
In the paragraph of the thermo-hygrometric requirements, and room ventilation, the 13011 Circular prescribes that following points:
- During the winter period the temperature of the environments must be equal to 20 °C ±2 °C, in all hospital departments, including services, guaranteed by the heating system;
- In the winter, in patients rooms, in collective rooms and in the corridors, should be guaranteed a relative humidity value of 40% ± 5%;
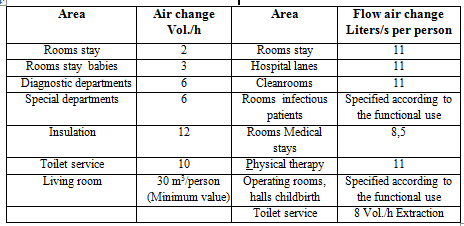
- The values of air changes, reported in Table 1b, must be guaranteed by a system of forced ventilation, where the suitably filtered air, is subsequently introduced in environments at the speeds no more than 0.15 m/s;
- In the operating theaters, labor rooms, intensive care, premature births, infants, intensive care, dialysis center, sterile field and analytical laboratories, the air conditioning system, without recirculation, should ensure either in summer or in winter in all case the values of the UNI 10339.
Table 1a. Values by International and Italian standards
Table 1b. Flow air-exchange, circular 1301 and UNI 10339
The conditioning and ventilation systems of the hospitals facility are designed to control the following parameters:
- Air temperature;
- Absolute humidity or moisture;
- Minimum flow of outdoor air;
- Over-pressure of an environment compared to the outside and/or to neighboring environments;
- Concentration of contaminants as particulate and/or gaseous chemical nature from the outside air and/or products within the environment;
- the evolving viruses and bacteria in the outside air and/or in environments with critical values are generally provided by technical standards and guidelines.
The difficult control of these parameters in HVAC systems to perform the required checks need sometimes inflexible solutions and low efficiency energetic audit. To overcome these problems, the AICARR suggests specific measurement in these cases.
- Inside of hospital facilities, the most critical hygrothermal environments for the air quality, are defined "high care" areas, where demands for process parameter values must fit in well defined fields.
- In these areas the comfort requirements become prevalent, compared to the lower intensity care environments, which are so-called "low care" areas, where patients spend much longer periods.
- In any case, the HVAC systems, has to ensure the safety and health of all users of the hospital and those who work in it.
- In general, therefore, the values of temperature, speed and relative air humidity, and outside air flow rates and recirculation must be defined according to specific needs, based on the aim to use the environment.
- These values must be obtained and maintained by following a "performance" approach mode, using the result who must be achieved more than the methods used to achieve it, and not "prescriptive" mode, by limiting itself to verify compliance with the values of some operation parameters which limit plant.
This proceeding, followed by a lot of country, is able to development and use new technologies "e-sensing" to monitoring the hospitals field, [12-15]: for the detection of main pollutants [16-24], in museums, to study the possible causes of deterioration of works of art, [25-27], allows you to joint either all monitoring parameters and avoid the risk to overcome limits of these parameters.
In the eco-friendly air conditioning significant progress has been achieved and are desirable in the close future to their applications [28-30].
The study case, is represented by the Hospital Papardo, at Messina; Built in the second half of the 90s, the complex architecturally is articulated, as shown in Fig. 1.
The building structure were made by steel elements (IPE) which create the framework, the perimeter walls are made by prefabricated, reinforced concrete and glass fibers, while the internal partitions consist of sandwich panels. The air conditioning and ventilation of the environments use the mixed mode "air-water", provide primary air system and fan-coils, in accordance with the legislation and requirements of the hospital laws. The area shoud be monitored were selected, after a preliminary screening, among those structure intended to the hospitals, and are located in the main part and to the side part of the the Hospital.
The screening led to the selection of areas with energetic problems encountered in the entire complex.
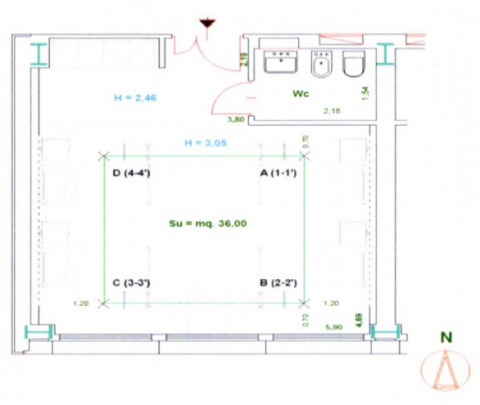
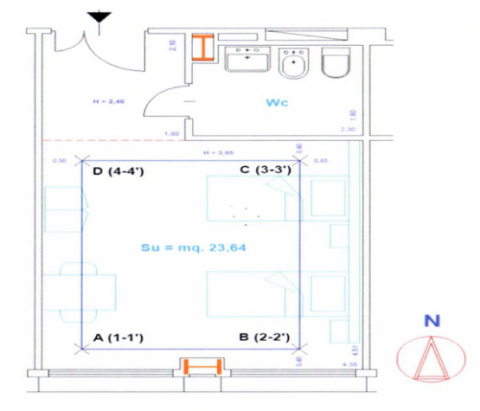
The monitored environments are constituted by patient rooms, with two and four beds, located in several zone of the hospital, - in the Fig. 2 is shown the plants.
In this rooms, are been performed measurements of physical quantities relating monitoring object of the study.
By comparing the value obtained on the different floors of the investigated hospital, it was observed, that just ten environments are enough to measures the microclimatic physical quantities representative of the various combinations for the orientation and the conditions founded in the different floors of the complex. The aim of this study is to assess the current conditions of comfort by temperature and humidity, provided by the HVAC (Heating systems, Ventilation & Air Conditioning) of the complex hospital investigated [6], and at the specific needs represented by environments for the care of patients hospitalization.
Figure 1. The Papardo Hospital in Messina
The first measurements were made in the years 2009-10, and after it the next measurements was performed in the winter campaigns: in November 2013 and January 2014, and in the summer in July 2014.
The observations were performed in the hourly period 10:00÷ 12:00, by keeping turn on the air conditioning system.
Were also detected the external thermo-hygrometric parameters during monitoring, for obtained an average value of the period investigated.
To choose the measuring points we referred to these following rules:
- Do not interpose with the performance of the normal work duties of the doctor and staff, and do not interfere, with the patients during their surveys.
- To allow easy positioning of the instrumentation.
The measurements were conducted by placing the equipment at four points inside the room, according to a survey grid, suggested by ISO7726 A [7].
The thermo-hygrometric parameters were monitored at 1.10 m high from the floor, as indicated by A ISO7726.
the Fig. 2 shows the points, A, B, C, D, where they have been positioned the probes for the detections, of two wards-type, while in Fig. 3 is shown the measuring equipment endeavored during the detection.
The beginning of all measurements occurred after a time interval equal about 10 minutes, to allow at the probes to achieve conditions equilibrium to work in microclimatic conditions of the environment. The detected parameters need to calculate the values of PMV (Predicted Mean Vote) and PPD (Percentage of dissatisfied).
Figure 2. Plan of the "Room type patients” 2 and 4 beds
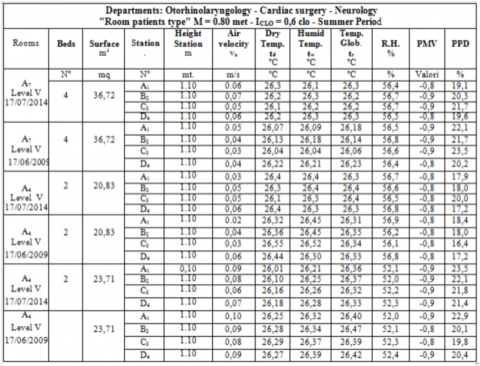
To obtain these indices, it has been set a predetermined value of the metabolic level equal to 0.8 Met and a value of the thermal resistance of clothing of 0.8 Clo, for the winter period and 0.6 Clo for the summer, with the same conditions of hospitalized patients.
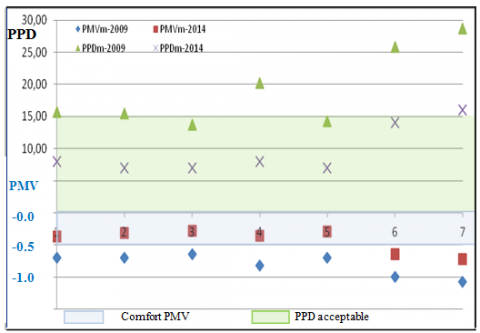
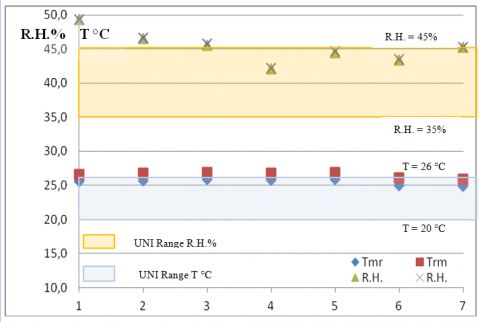
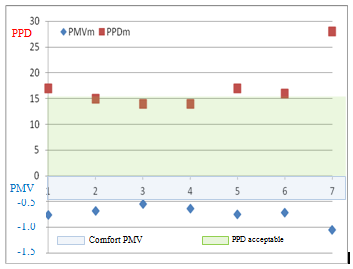
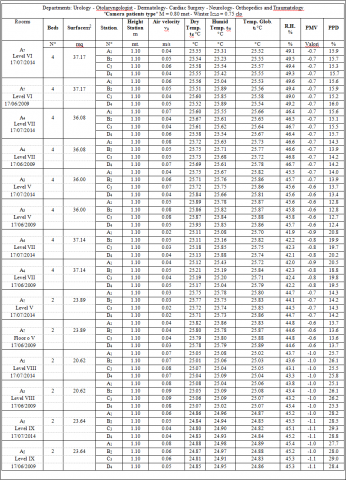
The most significant results of the values measured parameters, are reported in the Table 2 and Table 3, while in the graphs of Fig. 4, and Fig.6 are shown the values of the PMV and PPD calculated in the rooms monitored in winter and summer period, even if the values by mean radiant temperature Tmr and average relative humidity inside of the investigated rooms.
As you can see the average values of the measured parameters, PMVm and PPDM are out of range of comfort PMV <-0.5, and PPD> 15%.
Figure 3. Instrumentation used for the relief
Table 2. Values of parameters determined during summertime
Figure 4. Values of PMVm and PPDm wintertime
Figure 5. Temperature values, Tmr and humidity, R.H
Figure 6. Values of PMVm and PPDm Summertime
Table 3. Values of parameters
Afterwards the above data, detected by the measuring campaigns carried out, it was considered appropriate to deepen the study, in two type-chambers of the ten rooms analyzed, characterized by the placed on the same vertical, exposition to the South and different floors (These chambers are named: VIII and IX).
The rooms selected are:
- "room-hospitalization type for the Department of Pediatrics”, body A5, floor VIII;
- "room-hospitalization type” for the Plastic Surgery", body A5 department, ninth floor,
The room located on the ninth floor, is the last of the section placed on the same vertical with a flat roof covered by solar plate.
From results previously reported, it is shown for the above two bedrooms, values of PMV (Average Expected) and PPD (percentage of dissatisfied), over the legal range expected for the quality classes of the overall comfort.
Therefore other targeted studies are needed, with acquisition of additional elements to get solutions more appropriate projects.
It was still made a thermographic investigation on the building façade of the hospital, in the same side of the two type rooms, with the Thermal-CAM E320 of "FLIR Systems" (see Fig. 7), with the aim to verify the problems relating to the building thermal quality and their aspects (outer casing).
Below are proposed some design solutions which vary the building facade, relatively to the glass components. While for the opaque surfaces to direct contact with the outside it has been suggested a system to "coat traditional" (sandwich walls).
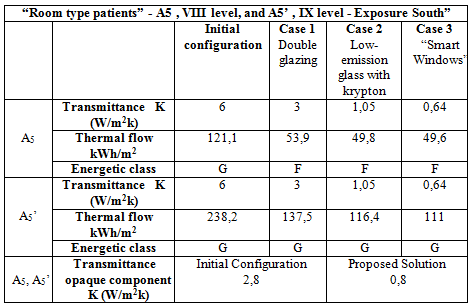
With regard to the glass surfaces, has been performed a simulation, which give to us the relative energy classification of these three design solutions listed below:
- substitution of the frame of the windows, with fixtures in aluminum thermal break and double glasses having transmittance K = 3.0 W/m2K;
- substitution of the frame current, with aluminum frames with thermal break and "low-emissivity glasses" having transmittance K = 1.05 W/m2K;
- substitution of the frame current, with window frames with in aluminum at thermal break, surfaces and active windows of the type "smart windows" having average transmittance equal k = 0.64W /m2k [31-34].
In the Table 4 and Table 5 are reported the values W/m2K) determined for the environment designed, to vary the component of the type of glazing applied.
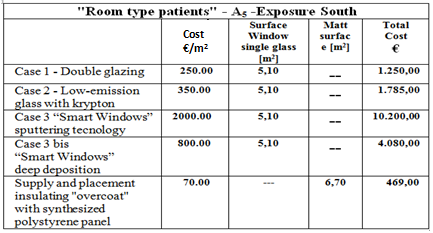
It has been carried out a thorough market survey on the sector and on the workers who apply insulating panels for the realization of isolations to "coat" and on the perimeter interior walls, identifying the following square meter costs and the overall costs for room-type reported in Table 5.
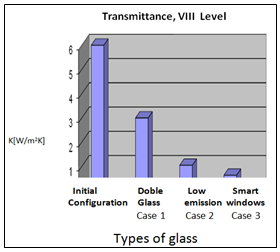
Undoubtedly it can be inferred that the best solution currently feasible is the third solution, "Smart Windows" as shown in the following charts reported in Table 5.
The analysis described in this article is the first part of a project aimed to study the thermo-hygrometric comfort and the indoor air quality and a more conscious use of energy in hospitals, for use, in environments hospital, based on the evaluation of the comfort indices in patient rooms.
Currently the investigated hospital, shows a framework microclimatic, with of clear discomfort aspects, in both seasons.
Indeed, the of the calculated thermal sensation values indices of the rooms where are been the measurements carried out, fall within the ranges -2<PMV<-0.5 and PPD>15%, and thus in the discomfort zone.
By examining the Table 2 and Table 3, and graphs shown in Fig. 4, and Fig. 6, related to the winter and summer monitoring, the values of the PMVm, result at minimum of the acceptability limit. With values within 15%, with percentage of dissatisfied of 20%.
To reduce the range of the inacceptable values are thus necessary the proposed corrective actions, to which a further measure campaign will be performed.
Table 4. Transmittance, walls opaque and glass
Figure 7. "Thermal-CAM"-Frontal views of hospital rooms type
The reported values show how the environment require es suitable technical interventions, evidently presenting constructive problems and not adequate distributions in many equipment of the plant.
The measures of the thermo-hygrometric values of the comfort indices, has also permitted to carry out a first characterization of the operation of the hospital conditioning with regard to the monitored environment and we lead to believe that are necessary interventions to the best control of the system.
By an analysis of the costs related to the three design solutions, we believe that the solution n ° 3 and precisely the f "Smart windows" solution, which was realized with "deep-coating" deposition technique, is the most suitable to solve the comfort problems in the hospital stays, in according to the quality-price.
Figure 8. Values transmittance rooms
Table 5. Cost of proposed design solutions
[1] ISPESL. (2009). Dipartimento Igiene del Lavoro, Linee iguida per la definizione degli standard di sicurezza e di igiene ambientale dei reparti operatori, (In Italian) http://www.ispesl.it/.
[2] Raffellini G., Cellai G.F., Carletti C. (1997). Air quality in a hospital environment: Analysis and control of air conditioning systems, Proceedings National Congres AICARR, Milano, ISBN: 9788895620183.
[3] Martinazzoli G. (1995). Gli Impianti Ospedalieri. Guida Alla Progettazione Integrate, Carocci, ISBN: 9788843003037.
[4] ISO 14644-1. (2005). Cleanrooms and associated controller environments. Part 1. Classification of air cleanliness, International Organization for Standardization Technical Committee.
[5] ISO 7730. (1993). Moderate thermal environments-determination of the PMV and PPD indices and specification of the conditions for thermal comfort, Geneva, International Standards Organization.
[6] ANSI/ASHRAE-170. (2008). Ventilation of health care facilities, ASHRAE Standards Committee, the ASHRAE American National Standards Institute, USA.
[7] IUNI EN ISO 14644-1 2006. (2006). Clean rooms and associated controlled environments. Part 1: Classification of air cleanliness.
[8] Cannistraro G., Cannistraro M., Restivo R. (2015). Some observations on the radiative exchanges influence on thermal comfort in rectangular open-space environments, IJHT, Vol. 33, pp. 79-84. DOI: 10.18280/ijht.330213
[9] Cannistraro G., Cannistraro M., Restivo R. (2015). The local media radiant temperature for the calculation of comfort in areas characterized by radiant surfaces, IJHT, Vol. 33, pp. 115-122. DOI: 10.18280/ijht.330116
[10] Fanger P.O. (1970). Thermal Comfort, McGraw-Hill, N.Y.
[11] Olesen B.W. (1984). How many sites are necessary to estimate a mean skin temperature? Thermal Physiology, Raven Press, New York, pp. 34-38.
[12] Cannistraro G., Cannistraro M. (2016). Hypothermia risk, monitoring and environment control in operating rooms, IJHT, Vol. 34, No. 2, pp. 165-171. DOI: 10.18280/ijht.340202
[13] Cannistraro M., Leonardi S.G., Aloisio D., Patti E., Pace C., Khalaf W., Donato N., Neri G. (2013). Development of electronic-nose technologies for biomedical applications, Intern. Congress XVII Annual Conference AISEM, Brescia.
[14] Cannistraro M., Lorenzini E. (2016). The applications of the new technologies “E-Sensing” in hospitals, Vol. 34, No. 4, pp. 551-557. DOI: 10.18280/ijht.34040
[15] Cannistraro G., Cannistraro M., Galvagno A., Trovato G. (2017). Analysis and measures for energy savings in operating theaters, IJHT, Vol. 35, No. Sp. 1. To be republished.
[16] Salata F., Golasi I., Petitti D., de Lieto Vollaro E., Coppi M., de Lieto Vollaro A. (2017). Relating microclimate, human thermal comfort and health during heat waves: An analysis of heat island mitigation strategies through a case study in an urban outdoor environment, Sustainable Cities and Society, Vol. 30, pp. 79-96. DOI: 10.1016/j.scs.2017.01.006
[17] Cannistraro G., Cannistraro A., Cannistraro M., Galvagno A., Trovato G. (2016). Analysis of the air pollution in the urban center of four Sicilian cities, IJHT, Vol. 34, No. S.I.2, pp. S219-225. DOI: 10.18280/ijht.34S205
[18] Cannistraro G., Cannistraro M., Cannistraro A. (2016). Evaluation of the sound emissions and climate acoustic in proximity of one railway station, IJHT, Vol. 34, No. S.I.2, pp. S589-596. DOI: 10.18280/ijht.34S255
[19] D'Orazio A., Fontana L., Salata F. (2011). Experimental study of a semi-passive ventilation grille with a feedback control system, Review of Scientific Instruments, Vol. 82, No. 8, Art. No. 085107. DOI: 10.1063/1.3626793
[20] Intini F., Rospi G., Cardinale N., Köhtz S., Dassisti M. (2016). Life cycle assessment of Italian residential windows: Sensitivity of analysis, IJHT, Vol. 34, pp. S235-S241. DOI: 10.18280/ijht.34S207
[21] Marino C., Nucara A., Pietrafesa M. (2015). Mapping of the indoor comfort conditions considering the effect of solar radiation, Sol. Energy, Vol. 113, pp. 63-77. DOI: 10.1016/j.solener.2014.12.020
[22] Marino C., Nucara A., Pietrafesa M. (2017). Thermal comfort in indoor environment: Effect of the solar radiation on the radiant temperature asymmetry, Sol. Energy, Vol. 144, pp. 295-309. DOI: 10.1016/j.solener.2017.01.014
[23] Cardinale N., Stefanizzi P., Rospi G., Augenti V. (2010). Thermal performance of a mobile home with light envelope, Building Simulation, Vol. 3, pp. 331-338. DOI: 10.1007/s12273-010-0017-0
[24] Salata F., Alippi C., Tarsitano A., Golasi I., Coppi M. (2015). A first approach to natural thermoventilation of residential buildings through ventilation chimneys supplied by solar ponds, Sustainability (Switzerland), Vol. 7, No. 7, pp. 9649-9663. DOI: 10.3390/su7079649
[25] Cannistraro M., Cannistraro G., Piccolo A., Restivo R. (2013). Potential and limits of oxidative photocatalyses and possible applications in the field of cultural heritage, Advanced Materials Research, Vol. 787, pp. 111-117.
[26] Cannistraro G., Cannistraro M., Restivo R. (2013). Messina’s historical buildings after the earthquake of 1908: Energy and environmental analysis through a global screening methodology, IJHT, Vol. 31, No. 2, pp. 155-158. DOI: 10.18280/ijht.310221
[27] Cardinale T., Rospi G., Cardinale N. (2014). The influence of indoor microclimate on thermal comfort and conservation of artworks: the case study of the Cathedral of Matera (South Italy), Energy Procedia, Vol. 59, pp. 425-432. DOI: 10.1016/j.egypro.2014.10.398
[28] Cannistraro G., Cannistraro M., Cannistraro A., Galvagno A., Trovato G. (2015). Evaluation of the convenience of a citizen service district heating for residential use. A new scenario introduced by high efficiency energy system, IJHT, Vol. 33, No. 4, pp. 167-172. DOI: 10.18280/ijht.330421
[29] Cannistraro G., Cannistraro M., Galvagno A., Trovato G. (2016). Evaluation technical and economic the integrations of co-trigeneration systems in the dairy industry, IJHT, Vol. 34, No. S.I.2, pp. 332-336. DOI: 10.18280/ijht.34S220
[30] Cucumo M., Ferraro V., Kaliakatsos D., Mele M., Barci G. (2016). Performance of a fields of geothermal probes to support the air conditioning plant of a public building powered by water/water heat pumps, IJHT, Vol. 34, S.I.2, pp. S535-S544. DOI: 10.18280/ijht.34S248
[31] Cucumo M., Ferraro V., Kaliakatsos D., Mele M., Nicoletti F. (2016). Calculation model using finite difference method for energy analysis in a concentrating solar plant with linear Fresnel reflectors, IJHT, Vol. 34, No. S.I.2. DOI: 10.18280/ijht.34S221
[32] Kaliakatsos D., Cucumo M., Ferraro V., Mele M., Cucumo S., Miele A. (2017). Performance of dishstirling CSP system with dislocated engine, Internat. Journal of Energy and Envir. Eng., Vol. 8, No. 1, pp. 65-80. DOI: 10.1007/s40095-015-0183-z
[33] GermanòD., Cannistraro G., Castelluccio M.E., Piccolo A. (2007). Computazione dell’efficienza energetica di Smart windows elettrocromiche negli edifici: Un caso studio, Pubblicato agli atti del “62° Congresso Nazionale ATI” Salerno 11-14/09/2007”.
[34] Piccolo A., Germanò D., Ponterio L., Simone F. (2007). Energy performance of an electromagnetic smart window prototype for controlling solar gain and visual comfort in buildings, Proceedings “62° Nationla Congres ATI Salerno.
[35] Germanò D., Piccolo A., Plutino D., Rizzo G. (2007). Development and charaterization of two electrochromic devices based on the sol-gel deposition technique, 62° National ATI Salerno.
[36] Piccolo A., Siclari R., Rando F., Cannistraro M. (2017). Comparative performance of thermoacoustic heat exchangers with different pore geometries in oscillatory flow. implementation of experimental techniques, Applied Science, Vol. 7, p. 784. DOI: 10.3390/app7080784