Abrar Taha![]() | Inass Abdulah Zgair
| Inass Abdulah Zgair![]() | Ali Abdul Hussein
| Ali Abdul Hussein![]() | Narimann Neamah Hussein
| Narimann Neamah Hussein![]() | Taghreed N. Jamil
| Taghreed N. Jamil![]() | Thualfakar Hayder Hasan
| Thualfakar Hayder Hasan![]() | Kahtan A. Mohammed*
| Kahtan A. Mohammed*![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Radiation impacts living organisms in several ways, and its biological effects vary depending on the type and dose of exposure. It can damage DNA, potentially causing mutations and increasing the risk of cancer. Ionizing radiation can harm the human body through two primary mechanisms. Direct damage occurs when radiation strikes essential biological molecules, such as DNA, breaking or altering their structure. Indirect damage arises when radiation interacts with water molecules—abundant in cells—generating free radicals, which are highly reactive and can harm cellular components. These free radicals can react with DNA and other cellular components, leading to molecular damage. Depending on the radiation dose and exposure rate, the biological effects can range from minor, repairable molecular damage to cell and tissue death. These outcomes may result in acute or chronic health conditions, such as Acute Radiation Syndrome (ARS) and an increased risk of cancer. Additional consequences may include cardiovascular diseases and thermal effects, which can cause localized tissue overheating and damage. Radiation exposure can also suppress the immune system, thereby increasing susceptibility to infections. Negative effects on mental and physical development or birth defects may result from exposure during developmental stages, such as pregnancy. Exposure to radiation in specific situations, like nuclear accidents, can result in mental health issues like depression and anxiety. Proper precautions must be taken when handling radiation sources, as health risks generally increase with higher exposure doses.
radiation, ionizing, non-ionizing, living tissues, biological effects, acute effects, chronic effects
Radiation exposure is defined by the amount of ionization caused in air by radiation and is typically measured as the electrical charge produced by ionizing radiation in a unit volume of air [1]. Exposure to radiation from an external source may affect the entire body, a specific limb, or individual organs or tissues, resulting in an external radiation dose. In contrast, internally deposited radioactive material (RAM) can expose specific tissues, organs, or the entire body to internal radiation [2]. The biological effects of radiation are generally classified into two categories: deterministic effects (e.g., tissue damage) and stochastic effects, including carcinogenic changes. Stochastic effects have no threshold and are considered dose-independent; however, the probability of their occurrence increases with the radiation dose. As a stochastic hazard, radiation-associated malignancies can develop even at low doses, with the probability increasing proportionally with the radiation dose. The stochastic mechanism involves unpredictable and irreversible DNA damage in a small number of viable cells [3]. Depending on a number of variables, including the radiation dose, exposure rate, type, and body part exposed, different tissues are affected by radiation exposure. Localized effects include radiation burns, whereas systemic effects are exemplified by Acute Radiation Syndrome (ARS). Radiation exposure can be classified into "low-risk" and "high-risk" categories for individuals and groups. The time between exposure and the onset of symptoms, as well as the severity of those symptoms, are the first factors used to make the diagnosis [4]. Although ionizing radiation can directly harm proteins, RNA, and DNA, it usually does so indirectly by interacting with intracellular water molecules to produce extremely reactive free radicals. Lower radiation doses may disrupt homeostasis, cellular proliferation, and endogenous molecular repair systems, while higher doses may result in cell death. Atrophy, progressive tissue hypoplasia, and ultimately fibrosis can be caused by damage to these and other cellular constituents. Nevertheless, it is now evident that cell death by itself is insufficient to account for a large number of tissue reactions, as these reactions also rely on intricate processes such as immune, inflammatory, and chronic oxidative reactions, in addition to damage to the extracellular matrix and vasculature [4-9]. This study aims to explore the biological effects of radiation exposure, with a particular focus on medical radiation sources and nuclear waste.
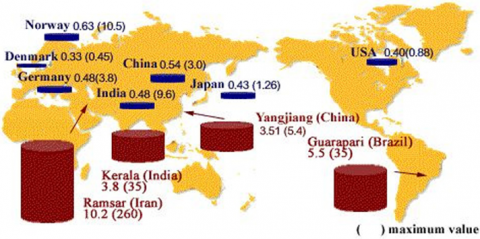
Natural sources account for the majority of ionizing radiation exposures in humans [5-7]. Generally speaking, these exposures are not radiologically dangerous unless they are increased by human activity, like mining, High geomagnetic latitudes, and high altitudes, when exposure to cosmic radiation is increased, or locations with high background radiation areas (HBRA), where the local geology has high amounts of the primordial radioactive elements. There are a lot of HBRAs throughout the world [8, 9]. Figure 1 shows high background radiation areas around the world. There are parts of the Iranian seaside city of Ramsar in the north that have some of the highest natural radiation levels ever recorded. The ICRP-recommended radiation dose limits for radiation workers are a few times lower than the effective dose equivalents in Ramsar's very high background radiation regions (VHBRAs), especially in Talesh Mahalleh [10].
Figure 1. High background radiation areas around the world [10]
Due to the rapid growth of the nuclear power industry, people living near nuclear power plants have become increasingly aware of changes in ambient radiation levels and their potential health effects [11-13], particularly after the 2011 Fukushima Daiichi nuclear power plant accident. In order to do this, a number of countries have put in place surveillance systems for monitoring radioactivity and assessing radiological risk before and after NPP operations [14, 15]. The two primary ways that radiation impacts human health are through internal and external exposure. Drinking water is thought to be a significant source of radiation exposure for humans, per a 2000 study conducted by the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) [16]. One of the main sources of radiation exposure for humans is thought to be water. Long-term exposure to relatively high levels of radioactivity in ambient air and drinking water can cause major health issues, including cancer [17].
4.1 Radiation exposure by CT scan
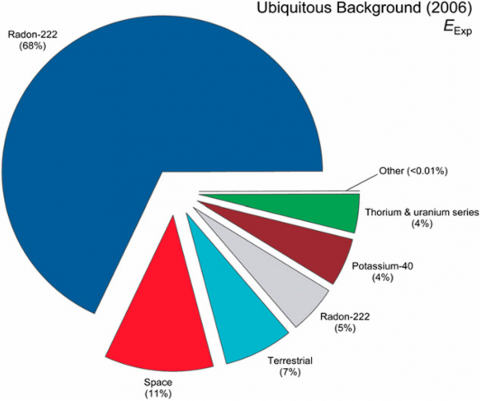
The use of CT scans and radiation doses derived from them has increased along with awareness of the potential for modest doses of X-ray radiation to cause cancer, especially in children. The follow-up period for atomic-bomb survivors, now over 50 years, and the consistency of the risk estimates with those from other large-scale epidemiologic studies have greatly increased our confidence in our understanding of the lifetime cancer risks from low doses of ionizing radiation. These factors imply that the anticipated dangers of CT are not theoretical, meaning they are not predicated on big dosage extrapolations or models. Instead, they are predicated on real cancer rates linked to high radiation exposure levels [18]. CT scans are a leading source of medical radiation exposure. Several cohort studies, including atomic bomb survivors, have established a dose-dependent increase in cancer risk. Figure 2 shows the total amount of background radiation that the American people get from various sources. according to the Environmental Protection Agency, but in general, steep or mountainous terrain is more likely to have a higher risk of radon exposure [19].
Figure 2. The contribution from different sources of background radiation to the United States [19]
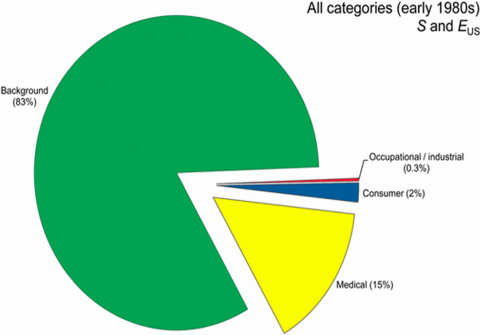
Figure 3 shows the exposure of the United States population in the early 1980s. In contrast, statistics from 2006 indicated a significant rise in medical exposure from 15% to 48%. EUS5 effective dose per individual in the United States; S5 person-Sv [19].
Figure 3. The exposure of the United States population in the early 1980s [19]
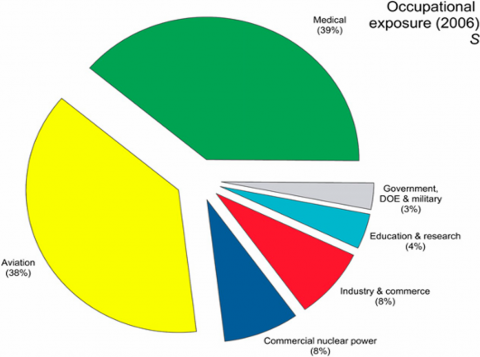
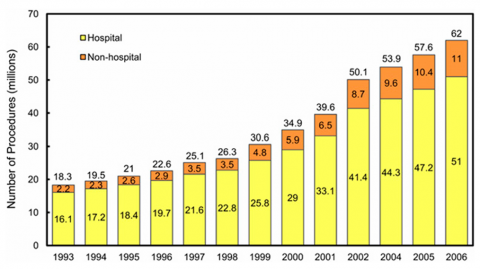
In the United States, the annual number of CT operations increased by almost 239%, from 18.3 million in 1993 to 62 million in 2006. Numerous variables, such as improved technology, throughput, and diagnostic reliability, are responsible for this significant rise. While ever-increasing slice thicknesses (from 16 to 32 to 64 to 128 and even larger) have historically resulted in an ever-increasing dosage of ionizing radiation to the patient, they have also provided an ever-increasing resolution. The public and scientific community have taken CT dose reduction strategies very seriously as a consequence of this exposure, which has eventually caused the slice thickness increases that were seen a few years ago to stabilize (Figure 4 and Figure 5) [19].
Figure 4. The contribution of medical exposure (39%) to occupationally exposed individuals [19]
Figure 5. Chart of the number of CT procedures per year in the United States from 1993 to 2006 [19]
4.2 Healthcare workers and nuclear industry workers
Studies of individuals exposed to radiation at work provide an increasingly important source of information on the effects of prolonged low-dose-rate exposure to external radiation sources. Ingestion of radionuclides such as plutonium has also exposed certain workers to internal radiation sources [20].
Nuclear disaster preparedness and response standards—including recommendations on radiation protection, health management, and community communication—have been studied and used by decision-makers to guide protective measures for residents living near nuclear power plants in the event of an accident [21].
These studies used annual data on reactor construction capacity and the timing of three nuclear accidents rated five or higher on the International Nuclear and Radiological Event Scale. A panel dataset of 31 countries from 1965 to 2009 was employed to examine the impact of nuclear accidents on energy policy. After estimating the magnitude of these accidents' effects across countries, the results indicate that the Chernobyl disaster had a globally negative influence on reactor construction starts, whereas neither the Three Mile Island (TMI) nor the Lucens accidents had a significant effect [22].
Clinical professionals and patients exposed to ionizing radiation are becoming more aware of the dangers associated with using this radiation for diagnostic purposes. The necessity for doctors to understand the hazards and reduce radiation exposure for patients has been brought to light by the revisions to the laws controlling the use of ionizing radiation [23].
Fluoroscopic imaging is now often used in fields including neurosurgery, vascular surgery, orthopedics, and urology. Staff members are exposed to radiation by dispersed radiation from the primary radiation beam's contact with the patient and the operating table. When medical professionals stand near a C-arm fluoroscopic unit, their upper and lower extremities will be exposed to scatter radiation from all directions. The operating surgeon must wear thyroid shields and 0.35 mm lead aprons in accordance with conventional radiation protection protocols, and other staff members must wear 0.25 mm lead aprons [23].
Additionally, Humans are exposed to radiation from sources outside of their bodies while they live and/or work outdoors or within structures; these sources mostly include cosmic rays and gamma ray emitters found in building walls and soils. Humans also unintentionally introduce radionuclides into their bodies via the consumption of food and drink, as well as by breathing in air. Emissions of low penetrating a and b particles irradiate the body's confined areas. The primary sources of this internal radiation are 40K, a crucial component that is closely homeostatically regulated in the body, and radon (222Rn) and its decay products [24].
Radiation exposure has a wide range of immediate and long-term health impacts. Shortly after high-dose exposures, acute consequences like radiation sickness or Acute Radiation Syndrome (ARS) may appear. These symptoms may include nausea, vomiting, diarrhea, and bone marrow suppression [25]. Chronic or cumulative exposure to lower amounts of radiation over a protracted period of time may result in long-term consequences, including cancer induction, hereditary effects, and cataract development [26]. Because of their diverse cellular makeups and physiological roles, several organs and tissues—like the thyroid, lungs, and bone marrow—show variable susceptibilities to radiation-induced damage. Modern medicine relies heavily on radiation, which is a potent tool for research, diagnosis, and treatment. The viewing of interior anatomical structures and the very sensitive and precise identification of pathological anomalies are made possible by diagnostic imaging modalities, including X-rays, Computed Tomography (CT), and nuclear medicine techniques [27].
In the twenty-first century, hazards to public health and the environment from nuclear accidents, the disposal of radioactive waste, and industrial discharges of radioactive elements continue to be major issues. Radiation emergencies have far-reaching effects, including population displacement, long-term health effects, and socioeconomic disruptions, as demonstrated by such events as the Fukushima Daiichi accident in 2011 and the Chernobyl disaster in 1986 [28, 29].
7.1 Cancer
Cancer starts at the cellular level when a cell divides uncontrolled due to a sequence of mutations. Numerous things, such as inherited genetic abnormalities or DNA damage from environmental pollutants, may result in these mutations. Disease formation is sometimes broken down into three stages: commencement, when the initial mutation takes place; promotion, where cells start to proliferate uncontrolled; and progression, where the disease becomes more aggressive [30]. Higher radiation dosages and tissues like the thyroid and breast that are highly susceptible to ionizing radiation are more likely to have negative aftereffects. An estimated 0.6% of all malignancies diagnosed in the UK in 2004 were thought to be caused by radiation from X-rays [31]. To distinguish tumor cells from healthy ones, the immune system may use a variety of antigens generated by the numerous genetic and epigenetic alterations common to all malignancies. Balance between the co-stimulants' signals, even the immune control points, defines the final amplitude and the cell quality, which is caused by the cell recognition [32, 33]. To protect, immune checkpoints are required [34]. Table 1 shows some studies about the relationship between cancer with radiation (2016-2025) [34-39].
Table 1. Some studies about the relationship between cancer with radiation (2016-2025)
|
Year |
Author |
Key Finding |
|
2025 |
Gupte et al. [34] |
This is particularly crucial in the Indian context, given the rising demand for cancer treatment and persistent problems like limited accessibility and a lack of radiation facilities. |
|
2025 |
Zhang et al. [35] |
Therefore, when an external beam PBI technique is selected to treat a patient with low-risk early breast cancer on the Chinese mainland, this somewhat hypofractionated regimen offers an alluring alternative. However, we acknowledge that the schedule is very lengthy and that the results were based on a relatively small number of patients with a shorter follow-up period. |
|
2024 |
Jagsi et al. [36] |
aimed to assess whether, in addition to traditional selection parameters, a genetic test may be used to treat younger postmenopausal women without radiation treatment. |
|
2018 |
Goodhead [37] |
The unique characteristics of space radiation, which result in particle tracks of enormous complexity and variety, are especially taken into consideration in the NASA cancer risk prediction model. |
|
2018 |
Nasiri and Acosta-Tamayo [38] |
The first step in this work is to introduce and extract a set of longitudinally connected lung tumor characteristics. Then, to develop predictors for each patient attribute, a non-linear mixed-effect modeling technique is proposed. |
|
2016 |
Miyazaki et al. [39] |
They examined how important Hh/GLI signaling is for maintaining the stemness-related characteristics of pancreatic CSCs. We suggested and illustrated a new combination therapy utilizing the Hh/GLI inhibitor GANT61 in conjunction with mTOR inhibition in light of this significant molecule's discovery. This combination will enhance the therapy choices for this devastating illness and provide an effective method of controlling CSCs in pancreatic cancer. |
7.2 Genetic mutations
A mutation occurs when a small segment of a genome's nucleotide sequence changes (Figure 6) [40]. Hugo de Yeries first used the word "mutation" in 1900, when Mendel's concepts were rediscovery. It encompasses the structural change of a gene or chromosome as well as the result of that change [41]. Although most mutations are harmful, a significant percentage are thought to be "silent" and do not appear to affect the individual. Rarely, a mutation may even be advantageous, and it has the tendency to spread quickly across a population; harmful mutations often perish along with the organism that carries them [42].
Figure 6. Mutation [40]
A phenotypic shift is a discernible alteration in the organism caused by a gene mutation that alters the gene's output. "A mutant" is an organism whose phenotype has changed as a result of mutation, while "a wild-type" is an organism that displays the typical phenotype for that species [43, 44]. Ionizing radiation and mutagenic radiation are examples of environmental variables (mutagens) that may accelerate the naturally occurring rate of gene mutation, which is typically quite low [45].
The health consequences of ionizing radiation can be categorized into three main types: somatic effects, genetic effects, and teratogenic effects. Somatic effects are physical impacts that occur in the individual who has been exposed to radiation. These effects can be further classified based on the time of onset into early (acute) and delayed (chronic) effects. Genetic effects refer to heritable abnormalities that may appear in the offspring of exposed individuals (either the father or the mother). These mutations are passed on to future generations through the germline. Teratogenic effects are developmental abnormalities that occur in unborn children exposed to radiation in utero, particularly during the embryonic or fetal stages of development. Although these are developmental effects, they are often classified as a subset of somatic effects because they manifest in the individual affected, not in future generations [46].
More than eight years have passed since the 9.0 magnitude Great East Japan Earthquake on March 11, 2011, which resulted in a tsunami and the Fukushima Daiichi Nuclear Power Station (FDNPS), operated by the Tokyo Electric Power Company. Numerous radionuclides released into the atmosphere by the FDNPS eventually found their way into the surrounding terrestrial and marine environments [47]. Between 100 and 500 petabecquerels (PBq) of iodine-131 (131I) and 6 to 20 PBq of cesium-137 (137Cs) are thought to have been released overall [2]. On the other hand, the FDNPS anticipated 131I and 137Cs discharges that were roughly 10% and 20% of the expected discharges from the Chernobyl incident, respectively [48].
Numerous research studies have been conducted on plants after exposure to ionizing radiation, and specialized publications have focused on plant radiobiology. Most of the research has focused on exposure to external radiation, woody species, and (agricultural) field crops. FRED's plant references are drawn from more than 329 published works, many of which were first published in Russian before being translated into English. While most of the data comes from laboratory studies, several coniferous and deciduous woods have been intensively investigated through controlled field trials. There are few studies on long-term radiation exposures. Some were carried out in the wake of the Eastern Ukraine and Chernobyl disasters [48].
Events in Russia's contaminated regions are significantly influenced by long-range fallout (EURT: East Urals Radioactive Trial). Of the 208 references in the database pertaining to acute exposures, 23 percent discuss the umbrella end-points of morbidity, mortality, mutation, and reproductive capability, respectively. Roughly 15% of the articles were first published in English, while the remaining 85% were first published in Russian. Of the 121 references in the database that address chronic exposures, 41%, 5%, 26%, and 28%, respectively, address the umbrella end-points of morbidity, mortality, mutation, and reproductive capacity. Ninety-two percent of the studies deal with morbidity end-points, and about 32 percent of the papers were first published in English (Western literature). About 24% have to do with radiation from the Chernobyl accident [49].
8.1 Depleted uranium (DU)
Generally regarded as an emerging pollutant, depleted uranium (DU) was first widely released into the environment in Iraq during the military campaign known as "Desert Storm" in the early 1990s. According to some theories, DU poses a risk to both the troops who are exposed to it and the people who live in the contaminated regions of combat zones [50].
The fissile isotope uranium-235 (²³⁵U) is present in much lower quantities in depleted uranium (DU) compared to natural uranium. DU typically has an isotopic composition of about 99.977% 0.0008976% uranium-234 (²³⁴U), 0.2% ²³⁵U, and uranium-238 (²³⁸U). It can be created by reprocessing spent nuclear fuel and is the byproduct that remains after uranium enrichment [51].
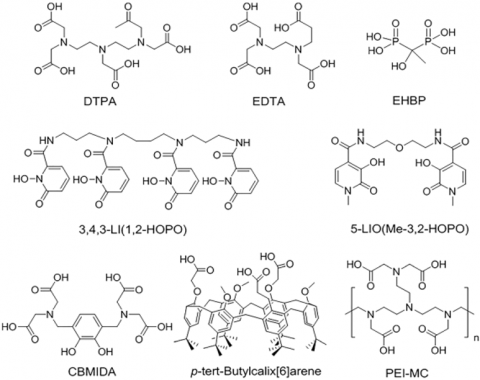
DU is known to be toxic both chemically and radioactively. It has about 60% of the radioactivity of natural uranium while maintaining very similar chemical characteristics, as shown in Figure 7. DU is frequently used in both military and civilian applications because of its low cost, superior penetrability, and pyrophoric properties. It can penetrate and destroy fortified structures and armored vehicles at high temperatures [52].
To effectively prevent and mitigate the toxic effects of depleted uranium (DU), it is essential to comprehend how DU is absorbed and distributed within the body. The solubility, physicochemical form, and route of entry of DU into the body are some of the complex factors that affect its absorption and bioavailability. In bodily fluids, more soluble forms, like uranyl nitrate and ammonium uranyl carbonate, can diffuse more easily. On the other hand, less soluble forms, such as UO₂, uranyl acetate, and ammonium diuranate, have a tendency to build up in particular organs and cause localized toxicity [53].
Uranium can be found in surface water as free metal ions, complexes with organic materials like humic materials, or inorganic ligands like phosphates and carbonates. Interactions between various uranium species are also possible. Although organisms normally have access to the forms UO₂²⁺ and UO₂OH⁺, the presence of humic substances and inorganic ligands can reduce the activity of these forms, thereby decreasing their bioavailability [54].
Figure 7. The chemical structure for DU chelating agents [55]
Since World War II, uranium, a radioactive heavy metal, has been known to pose a threat to human health in at least two ways. Like other heavy metals like chromium, lead, nickel, and mercury, uranium is chemically toxic to the kidneys, heart, liver, muscles, and nervous system. Furthermore, because of their radioactivity, all uranium isotopes emit radiation, a known carcinogen. Because of its lengthy residence periods in the lungs and potential to cause lung cancer, uranium was considered a major worry when it was absorbed as dust or aerosols. This implies that the highest levels of uranium that are soluble uranium compounds, particularly in the kidney, and the highest doses of uranium radiation exposures to the lung via insoluble uranium particles are the two ways that radiation protection and chemical regulatory bodies in the United States, which arguably has the most extensive uranium regulations, limit uranium exposures [56]. The chemical toxicity effects of uranium often manifest at lower concentrations than the radiation effects [57].
The few human studies that have looked at DU's carcinogenic risk are encouraging. Increases in micronuclei production in persons from the Bosnia/Herzegovina area [58] and reports of a rise in cervical carcinomas in Yugoslavia [59, 60] are examples of evidence of possible carcinogenic consequences. Moreover, chromosomal abnormalities in a German research group [61] and hypoxanthine-guanine phosphoribosyl transferase (HPRT) mutations in some Gulf War veterans [62] have been reported. In workers exposed to DU, two investigations have shown probable chromosomal abnormalities [63, 64].
8.2 Nuclear waste
"Nuclear Waste" and "Radioactive Waste" are occasionally used interchangeably in relation to waste management and safety. Nuclear waste has radiation levels above clearance standards, which is the primary difference between it and non-nuclear waste that produces a complex and extremely high radioactivity level [65].
Every stage of the nuclear fuel cycle generates high-level waste (HLW), intermediate-level waste (ILW), and low-level waste (LLW), in addition to the non-nuclear sector, research facilities, and hospitals. The nuclear fuel cycle generates gaseous, solid, and liquid waste products. Furthermore, spent nuclear fuel (SNF) is viewed as a source of U and Pu for reuse or as radioactive waste [66].
Wastes that contain or are contaminated with radionuclides at activity concentrations below the clearance values are traditionally classified as non-radioactive. The basic tenet is that there are background amounts of radioactivity in all materials and the environment around us, and that only substances and activities that substantially surpass these levels are regulated. In contrast, substances containing radionuclides and background levels of radiation, which are typically naturally occurring, do not pose any threat to the environment or to people (if not the opposite). Therefore, nuclear-related regulatory bodies do not have authority over the use of typically non-radioactive materials, albeit, depending on the circumstances, it may be subject to a variety of other rules and restrictions. Accordingly, trash generated by operations involving [67].
When living things are exposed to radiation, whether it be "Biological effect of radiation" refers to the effects of both ionizing and non-ionizing radiation, effects of determination, it is widely accepted that excessive radiation exposure causes deterministic and predictable side effects, including skin burns and acute radiation sickness. The severity of these effects increases as the dose increases and exceeds a particular threshold. Stochastic consequences, it is also well accepted that radiation exposure raises the chance of genetic alterations and cancer, among other stochastic consequences. Although the extent of the risk at low doses is still being investigated, it is generally believed that the risk of adverse effects rises with increasing exposure, even at low levels. The type of radiation, dose, and length of exposure are some of the variables that affect how different organisms react to radiation. Radiation biology research is now being conducted in the following areas: Low-Dose Long-Term Exposure's impact on health. This field focuses on comprehending the possible health hazards that can arise from long-term exposure to low radiation levels, such as those that might arise in the workplace or the environment. Finding biomarkers for early effects and researching the biological processes impacted by these dosages are part of this. The study of depleted uranium contamination focuses on the toxicity of the radioactive and chemical elements as well as how they affect soil, water, and living things. Impact of Radiation on the Immune System. Scientists are investigating the effects of radiation exposure, even at low levels, on the immune system's capacity to combat infection and other illnesses. Radiation's medical applications include creating novel radiation therapy methods for cancers, enhancing the efficacy of existing therapies, and lessening their adverse effects. It also covers the use of radiation in diagnostics and imaging in medicine. Cellular and Molecular Reactions to Radiation. Scientists investigate the cellular and molecular reactions of cells to radiation, such as apoptosis, DNA repair, and signaling pathway activation. Gaining an understanding of these processes can aid in the development of radiation protection plans and improve damage healing. Research in radiation biology is moving toward exciting fields such as biological radiation protection, in vivo radiation imaging, aluminum application in radiation monitoring, and artificial intelligence in radiation biology. Data analysis, using machine learning and artificial intelligence methods to examine vast volumes of data produced by radiobiology research in order to find new trends and connections and create more precise prediction models.
[1] Thrall, D.E., Widmer, W.R. (2018). Radiation protection and physics of diagnostic radiology. In Textbook of Veterinary Diagnostic Radiology, pp. 2-22. https://doi.org/10.1016/B978-0-323-48247-9.00013-9
[2] Sheetz, M. (2015). Radiological hazards and lasers. In Research Regulatory Compliance, pp. 113-157. https://doi.org/10.1016/B978-0-12-420058-6.00005-8
[3] Issa, Z.F., Miller, J.M., Zipes, D.P. (2009). Clinical Arrhythmology and Electrophysiology: A Companion to Braunwald's Heart Disease. Elsevier Health Sciences.
[4] Bushberg, J.T. (2025). Radiation exposure and contamination. Merck Manuals.
[5] United Nations Scientific Committee on the Effects of Atomic Radiation. (2011). Sources and effects of ionizing radiation. https://hprevot.fr/Chernobyl%20Report%20UNSCEAR%202011.pdf.
[6] Azzam, E.I., Jay-Gerin, J.P., Pain, D. (2011). Ionizing radiation-induced metabolic oxidative stress and prolonged cell injury. Cancer Letters, 327(1-2):48-60. https://doi.org/10.1016/j.canlet.2011.12.012
[7] United Nations Scientific Committee on the Effects of Atomic Radiation. (1993). Sources and Effects of Ionizing Radiation. https://www.unscear.org/unscear/en/publications/1993.html.
[8] Caswell, P.V., Baker, B.H. (1953). Geology of the Mombasa-Kwale Area. https://s3-eu-west-1.amazonaws.com/samsamwater1/maps/kenya/geology/Geology+of+the+Mombasa+Kwale+area.pdf.
[9] Sohrabi, M. (1993). Recent radiological studies of high level natural radiation areas of Ramsar. In Proceedings of International Conference on High Levels of Natural Radiations, Ramsar, Iran, pp. 39-47.
[10] Mortazavi, S.J. (2002). High background radiation areas of Ramsar, Iran. Kyoto (Japan): Kyoto University.
[11] Pidgeon, N.F., Lorenzoni, I., Poortinga, W. (2008). Climate change or nuclear power—No thanks! A quantitative study of public perceptions and risk framing in Britain. Global Environmental Change, 18(1): 69-85. https://doi.org/10.1016/j.gloenvcha.2007.09.005
[12] Cardis, E., Hatch, M. (2011). The Chernobyl accident—An epidemiological perspective. Clinical Oncology, 23(4): 251-260. https://doi.org/10.1016/j.clon.2011.01.510
[13] Tuo, F., Xu, C., Zhang, J., Zhou, Q., et al. (2013). Radioactivity analysis following the Fukushima Dai-Ichi nuclear accident. Applied Radiation and Isotopes, 78: 77-81. https://doi.org/10.1016/j.apradiso.2013.04.002
[14] Cao, J.Z., Yeung, M.R., Wong, S.K., Ehrhardt, J., Yu, K.N. (2000). Adaptation of COSYMA and assessment of accident consequences for Daya Bay nuclear power plant in China. Journal of Environmental Radioactivity, 48(3): 265-277. https://doi.org/10.1016/S0265-931X(99)00077-6
[15] Man, C.K., Kwok, Y.H. (2001). Assessment of risk to Hong Kong due to accidental releases of radionuclides from a nearby nuclear power plant. Journal of Radioanalytical and Nuclear Chemistry, 250(3): 485-490. https://doi.org/10.1023/a:1017949105942
[16] Hamlat, S., Thompson, P., Rinker, M., St-Amant, N., et al. (2018). Independent environmental monitoring and public dose assessment around the Canadian nuclear power plants. Journal of Radioanalytical and Nuclear Chemistry, 317: 325-335. https://doi.org/10.1007/s10967-018-5903-4
[17] Brenner, D.J., Hall, E.J. (2007). Computed tomography—An increasing source of radiation exposure. New England Journal of Medicine, 357(22): 2277-2284. https://doi.org/10.1056/NEJMra072149
[18] Wakeford, R. (2009). Radiation in the workplace—A review of studies of the risks of occupational exposure toionising radiation. Journal of Radiological Protection, 29(2A): A61. https://doi.org/10.1088/0952-4746/29/2A/S05
[19] National Council on Radiation Protection and Measurements. (2015). NCRP report No. 160, ionizing radiation exposure of the population of the United States. https://ncrponline.org/publications/reports/ncrp-report-160/.
[20] Ohba, T., Tanigawa, K., Liutsko, L. (2021). Evacuation after a nuclear accident: Critical reviews of past nuclear accidents and proposal for future planning. Environment International, 148: 106379. https://doi.org/10.1016/j.envint.2021.106379
[21] Csereklyei, Z. (2014). Measuring the impact of nuclear accidents on energy policy. Ecological Economics, 99: 121-129. https://doi.org/10.1016/j.ecolecon.2014.01.010
[22] Harris, L., Evans, C. (2003). Medical and dental guidance notes. A good practice guide on all aspects of ionising radiation protection in the clinical environment: By IPEM, York, 2002. Price: £ 20.00. Clinical Radiology, 58(4): 338. https://doi.org/10.1016/S0009-9260(02)00519-6
[23] Council, N.R. (2006). BEIR VII: Health risks from exposure to low levels of ionizing radiation: Report in brief. https://nap.nationalacademies.org/resource/11340/beir_vii_final.pdf.
[24] Mustapha, A.O., Patel, J.P., Rathore, I.V.S. (1999). Assessment of human exposures to natural sources of radiation in Kenya. Radiation Protection Dosimetry, 82(4): 285-292. https://doi.org/10.1093/oxfordjournals.rpd.a032637
[25] United Nations Scientific Committee on the Effects of Atomic Radiation. (2011). UNSCEAR, health effects due to radiation from the Chernobyl accident. UNSCEAR, Vienna.
[26] Valentin, J. (2000). Avoidance of radiation injuries from medical interventional procedures, ICRP Publication 85. Annals of the ICRP, 30(2): 7. https://doi.org/10.1016/S0146-6453(01)00004-5
[27] Hall, E.J., Giaccia, A.J. (2018). Radiobiology for the Radiologist. Wolters Kluwer.
[28] Linton, O. W., Mettler Jr, F. A. (2003). National conference on dose reduction in CT, with an emphasis on pediatric patients. American Journal of Roentgenology, 181(2): 321-329.
[29] Vogelstein, B., Papadopoulos, N., Velculescu, V.E., Zhou, S., Diaz Jr, L.A., Kinzler, K.W. (2013). Cancer genome landscapes. Science, 339(6127): 1546-1558. https://doi.org/10.1126/science.1235122
[30] de Berrington, G.A. (2004). Risk of cancer from diagnostic X-rays. The Lancet, 363(9406): 345-351.
[31] Greenwald, R.J., Freeman, G.J., Sharpe, A.H. (2005). The B7 family revisited. Annual Review of Immunology, 23(1): 515-548. https://doi.org/10.1146/annurev.immunol.23.021704.115611
[32] Zou, W., Chen, L. (2008). Inhibitory B7-family molecules in the tumour microenvironment. Nature Reviews Immunology, 8(6): 467-477. https://doi.org/10.1038/nri2326
[33] Pardoll, D.M. (2012). The blockade of immune checkpoints in cancer immunotherapy. Nature Reviews Cancer, 12(4): 252-264. https://doi.org/10.1038/nrc3239
[34] Gupte, A., Dandekar, P. R., Kadam, R., Dhoundiyal, M., et al. (2025). Acute toxicity and dosimetric analysis of ultra-hypofractionated radiation therapy for breast cancer. Turkish Journal of Oncology, 10(1): 1-10. https://doi.org/10.5505/tjo.2024.4423
[35] Zhang, X., Wang, X., Xu, Z., Chu, Y., et al. (2025). Hypofractionated partial breast irradiation after breast-conserving surgery for patients with early stage breast cancer in China Mainland: A single-arm prospective trial. Scientific Reports, 15(1): 3869. https://doi.org/10.1038/s41598-025-88600-5
[36] Jagsi, R., Griffith, K.A., Harris, E.E., Wright, J.L., et al. (2024). Omission of radiotherapy after breast-conserving surgery for women with breast cancer with low clinical and genomic risk: 5-year outcomes of IDEA. Journal of Clinical Oncology, 42(4): 390-398. https://doi.org/10.1200/JCO.23.02270
[37] Goodhead, D.T. (2018). Track structure and the quality factor for space radiation cancer risk (REID). https://three.jsc.nasa.gov/articles/Track_QF_Goodhead.pdf.
[38] Nasiri, F., Acosta-Tamayo, O. (2018). Mixed-effect modeling for longitudinal prediction of cancer tumor. arXiv preprint arXiv:1804.04590. https://doi.org/10.48550/arXiv.1804.04590
[39] Miyazaki, Y., Matsubara, S., Ding, Q., Tsukasa, K., Yoshimitsu, M., Kosai, K.I., Takao, S. (2016). Efficient elimination of pancreatic cancer stem cells by hedgehog/GLI inhibitor GANT61 in combination with mTOR inhibition. Molecular Cancer, 15: 49. https://doi.org/10.1186/s12943-016-0534-2
[40] Understanding Evolution. UC Museum of Paleontology Understanding Evolution. https://evolution.berkeley.edu/evolution-101/mechanisms-the-processes-of-evolution/the-causes-of-mutations/.
[41] Snustad, D.P., Simmons, M.J., Jenkins, J.B. (2003). Principles of Genetics John Wiley & Sons. Hoboken, NJ.
[42] Allan, R., Bainbridge-Smith, L., Greenwood, T., Shepherd, L. (2008). Advanced Biology A2: Student resource and activity manual. Biozone International Limited.
[43] Banoon, S.R., Salih, T.S., Ghasemian, A. (2022). Genetic mutations and major human disorders: A review. Egyptian Journal of Chemistry, 65(2): 571-589. https://doi.org/10.21608/EJCHEM.2021.98178.4575
[44] Lara-Reyna, S., Holbrook, J., Jarosz-Griffiths, H.H., Peckham, D., McDermott, M.F. (2020). Dysregulated signalling pathways in innate immune cells with cystic fibrosis mutations. Cellular and Molecular Life Sciences, 77(22): 4485-4503. https://doi.org/10.1007/s00018-020-03540-9
[45] McVey Ward, D., Griffiths, G.M., Stinchcombe, J.C., Kaplan, J. (2000). Analysis of the lysosomal storage disease Chediak-Higashi syndrome. Traffic, 1(11): 816-822. https://doi.org/10.1034/j.1600-0854.2000.011102.x
[46] Fuller, J.L., Simmel, E.C. (2021). Behavior Genetics: Principles and Applications. Taylor & Francis.
[47] Strom, D.J. (2003). Health impacts from acute radiation exposure. Pacific Northwest National Lab. (PNNL): Richland, WA (United States). https://doi.org/10.2172/15020969
[48] International Atomic Energy Agency. (2015). The Fukushima Daiichi accident. https://www-pub.iaea.org/MTCD/Publications/PDF/AdditionalVolumes/P1710/Pub1710-TV1-Web.pdf.
[49] United Nations Scientific Committee on the Effects of Atomic Radiation. (2013). UNSCEAR 2013 report volume I: Sources, effects and risks of ionizing radiation. https://www.unscear.org/unscear/en/publications/2013_1.html
[50] Real, A., Sundell-Bergman, S., Knowles, J.F., Woodhead, D.S., Zinger, I. (2004). Effects of ionising radiation exposure on plants, fish and mammals: Relevant data forenvironmental radiation protection. Journal of Radiological Protection, 24(4A): A123. https://doi.org/10.1088/0952-4746/24/4A/008
[51] Faa, A., Gerosa, C., Fanni, D., Floris, G., Eyken, P.V., Lachowicz, J.I., Nurchi, V.M. (2018). Depleted uranium and human health. Current Medicinal Chemistry, 25(1): 49-64. https://doi.org/10.2174/0929867324666170426102343
[52] Al Kaddissi, S., Frelon, S., Elia, A.C., Legeay, A., et al. (2012). Are antioxidant and transcriptional responses useful for discriminating between chemo-and radiotoxicity of uranium in the crayfish Procambarus clarkii? Ecotoxicology and Environmental Safety, 80: 266-272. https://doi.org/10.1016/j.ecoenv.2012.03.010
[53] Miller, A.C., Rivas, R., Tesoro, L., Kovalenko, G., Kovaric, N., Pavlovic, P., Brenner, D. (2017). Radiation exposure from depleted uranium: The radiation bystander effect. Toxicology and Applied Pharmacology, 331: 135-141. https://doi.org/10.1016/j.taap.2017.06.004
[54] Fattal, E., Tsapis, N., Phan, G. (2015). Novel drug delivery systems for actinides (uranium and plutonium) decontamination agents. Advanced Drug Delivery Reviews, 90: 40-54. https://doi.org/10.1016/j.addr.2015.06.009
[55] Markich, S.J. (2002). Uranium speciation and bioavailability in aquatic systems: An overview. The Scientific World Journal, 2(1): 707-729. https://doi.org/10.1100/tsw.2002.130
[56] Yue, Y.C., Li, M.H., Wang, H.B., Zhang, B.L., He, W. (2018). The toxicological mechanisms and detoxification of depleted uranium exposure. Environmental Health and Preventive Medicine, 23: 18. https://doi.org/10.1186/s12199-018-0706-3
[57] Craig, D.K. (2001). Chemical and radiological toxicity of uranium and its compounds. https://sti.srs.gov/fulltext/tr2001331/tr2001331.html.
[58] Hartmann, H.M., Monette, F.A., Avci, H.I. (2000). Overview of toxicity data and risk assessment methods for evaluating the chemical effects of depleted uranium compounds. Human and Ecological Risk Assessment, 6(5): 851-874. https://doi.org/10.1080/10807030091124239
[59] Papathanasiou, K., Gianoulis, C., Tolikas, A., Dovas, D., Koutsos, J., Fragkedakis, N., Papathanasiou, N. (2005). Effect of depleted uranium weapons used in the Balkan war on the incidence of cervical intraepithelial neoplasia (CIN) and invasive cancer of the cervix in Greece. Clinical and Experimental Obstetrics & Gynecology, 32(1): 58-60.
[60] Obralić, N., Gavrankapetanović, F., Dizdarević, Z., Durić, O., et al. (2004). The number of malignant neoplasm in Sarajevo region during the period 1998-2002. Medicinski Arhiv, 58(5): 275-278.
[61] Ibrulj, S., Krunic-Haveric, A., Haveric, S., Pojskic, N., Hadziselimovic, R. (2004). Micronuclei occurrence in population exposed to depleted uranium and control human group in correlation with sex, age and smoking habit. Medicinski Arhiv, 58(6): 335-338.
[62] Schroeder, H., Heimers, A., Frentzel-Beyme, R., Schott, A., Hoffmann, W. (2003). Chromosome aberration analysis in peripheral lymphocytes of Gulf War and Balkans War veterans. Radiation Protection Dosimetry, 103(3): 211-220. https://doi.org/10.1093/oxfordjournals.rpd.a006135
[63] McDiarmid, M.A., Keogh, J.P., Hooper, F.J., McPhaul, K., et al. (2000). Health effects of depleted uranium on exposed Gulf War veterans. Environmental Research, 82(2): 168-180. https://doi.org/10.1006/enrs.1999.4012
[64] Milacic, S. (2008). Health investigations of depleted-uranium clean-up workers. La Medicina del Lavoro, 99(5): 366-370.
[65] IAEA Safety Standards. (2014). Radiation protection and safety of radiation sources: International basic safety standards. https://www-pub.iaea.org/MTCD/Publications/PDF/Pub1578_web-57265295.pdf.
[66] Johnson, L.H. (1988). Spent fuel. https://inis.iaea.org/records/tqscd-f7384.
[67] Ojovan, M.I., Steinmetz, H.J. (2022). Approaches to disposal of nuclear waste. Energies, 15(20): 7804. https://doi.org/10.3390/en15207804