Khamees Khalaf Hasan![]() | Omar A Ibrahim*
| Omar A Ibrahim*![]() | Conrad Bucholtz | Marjorie Skubic
| Conrad Bucholtz | Marjorie Skubic![]() | James M. Keller
| James M. Keller![]() | Mihail Popescu
| Mihail Popescu![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Early detection of health changes is important for the success of an aging population that prefers to live independently. Sleep is crucial for maintaining the cognitive and physical health of older adults. Poor sleep quality is common among the elderly with mild cognitive impairment (MCI), which is a transient state between healthy cognition and dementia. Monitoring sleep quality can provide valuable insights into the health trends of older adults, but current methods are uncomfortable and inconvenient. We instead use Ballistocardiography, an unobtrusive method of capturing time in bed, heart rate, respiration rate, and restlessness. We then propose a sleep quality index (SQI) that uses this data to assess the sleep health of older adults. This sleep index was evaluated on six residents with a total of 1165 days of sensor data. Our results demonstrate the effectiveness of the proposed method in capturing various health conditions, which are illustrated through detailed case studies. A comparative analysis further highlighted the relationship between health conditions and sleep quality, showing that residents with frequent health issues had a significantly lower SQI compared to healthier residents. This significant difference underscores the utility of the SQI as a sensitive measure for detecting and monitoring health-related changes in sleep quality among older adults.
sleep quality, eldercare technology, early disease prediction, Ballistocardiography, remote monitoring, telehealth, cognitive health, preventative care, health monitoring systems
The elderly population aged 65 and older is increasing from 13% in 2010 to 19% in 2030, whereas the population of age 15-65 is decreasing [1]. Since older adults prefer to live independently, many of the health changes go undetected, such as dementia, frailty, and urinary tract infections (UTI) [2]. Detecting health changes early is crucial for promoting health and controlling healthcare costs. On the other hand, late health assessments or unreported problems can lead to poor quality of life [3]. Automatic health monitoring systems are a possible solution to identify and assess problems in their early stages, which provide more time for intervention to address the problems before they become serious. Such systems can be effective in supporting aging-in-place and allowing older citizens to maintain their independent lifestyle for as long as possible.
With the aging population increasing rapidly, the demand for innovative health monitoring solutions is more needed than ever. Sleep quality, in particular, has gained more attention from healthcare professionals. Poor sleep is recognized as a symptom of various health issues and can be the root cause the progression of serious conditions, such as cognitive decline and cardiovascular disease. Hence, integrating sleep quality monitoring into automatic health systems is essential for comprehensive eldercare.
Sleep quality is an important aspect of elderly mental and physical health [4-9]. Sleep is crucial for maintaining the brain and cognitive functions [10-12]. Poor sleep quality is a common factor among older adults with mild cognitive impairment (MCI), which is a transition stage between normal cognition and dementia [13]. More importantly, older adults with MCI are more likely to experience poor sleep than healthy older adults [14], and poor sleep is associated with an increased risk of progression from MCI to dementia [15]. Studies on animal models suggest that chronic poor sleep leads to increased cortical amyloid-beta (Aβ)—a hallmark pathology of Alzheimer's disease [16]. Sleep is therefore a critical aspect through which the brain maintains its cognitive health. When poor sleep becomes chronic, an acceleration of cognitive decline may occur [17].
In addition to the established links between poor sleep and cognitive decline, recent studies emphasize the role of sleep quality in overall health outcomes for older adults. Poor sleep is associated with a higher risk of falls, reduced immune function, and greater susceptibility to chronic conditions such as hypertension and diabetes [18, 19]. Addressing sleep disturbances through reliable monitoring and timely interventions could therefore play a pivotal role in preventing or delaying the onset of these conditions, thereby enhancing the quality of life for older adults. Furthermore, it is important to note that sleep disorders are often underdiagnosed in this population, which underscores the need for more effective monitoring solutions [20].
Sleep quality can be measured subjectively through questionnaires [21, 22] such as the Pittsburgh sleep quality index (PSQI) [23]. Questionnaire-based methods are not practical for long-term monitoring of older adults due to the burden of self-reporting. There are multiple quantitative ways to monitor sleep quality. Polysomnography is one way to compute sleep quality through a comprehensive recording of physiological changes that occur during sleep [24]. It requires multiple sensors to be placed on the patient's body, which makes it unsuitable for long-term sleep monitoring in the home. Actigraphy is another method to monitor sleep using nonobtrusive acceleration sensors that capture body movement data [25]. Wearable devices may have an accelerometer and heart rate monitoring, which may report sleep stages. The main drawback of these devices is the requirement to remember to charge them and wear them during sleep, which increases the burden on older adults who may have memory problems. Comfort is also a factor. Thus, the method is a sub-optimal solution for eldercare monitoring applications. The last technique is Ballistocardiography (BCG), which is an unobtrusive method for measuring heart rate, heart rate variability, respiration rate, and relative blood stroke volume based on the body movement induced by blood flow through the cardiovascular system, due to the heart's pumping mechanism [26]. BCG sensors are usually installed on the bed or under the mattress, which makes them more suitable for longitudinal monitoring of older adults.
While subjective measures like questionnaires provide valuable insights, they are not practical for continuous monitoring due to the reliance on self-reporting, which can be burdensome and less reliable in older adults. Objective methods, such as polysomnography, although comprehensive, are not suited for long-term use in home settings due to their invasive nature. On the other hand, actigraphy offers a less invasive alternative but still involves wearing devices that may not be ideal for older individuals who might find them uncomfortable or forget to use them. In contrast, BCG technology offers a promising solution by providing a non-intrusive, reliable way to monitor sleep patterns over time. Recent advancements in BCG have improved its accuracy and reliability, making it an even more viable option for eldercare settings [27, 28].
In this paper, we investigate a sleep quality measure that uses BCG but does not require sleep stages because these are often not accurate for older adults with noisy cardiac signals due to reduced stroke volume and increased stiffness in the vessels. We also avoid wearable devices due to the reasons mentioned above. Hence, we introduce a sleep quality metric from a bed sensor that is placed under the mattress and captures heart rate, respiration rate, and restlessness.
The contributions of this paper are: 1) a new sleep index that relies on a simple hydraulic-based bed sensor and does not require heart rate variability or sleep stages; 2) a penalty is applied to the sleep index if older adults do not meet the recommended sleep hours; and 3) a sleep normality score is introduced and incorporated to take into account unusual periods of sleep.
The paper is organized as follows. In section 2, we describe the eldercare monitoring system architecture. Section 3 describes the method, and Section 4 explains the sleep normality metric. Section 5 shows the dataset used in the study. Experimental results are displayed in section 6, and case studies are in section 7. Finally, section 8 provides conclusions.
TigerPlace is an eldercare facility that promotes aging-in-place located in Columbia, Missouri [29]. Sensor technology is applied to help older adult residents manage their illness and stay as healthy and independent as possible. After focus groups with TigerPlace residents and other older adults in 2004, a decision was made to use only non-wearable sensors in the monitoring process because they are unobtrusive and more acceptable to older adults [30, 31]. With the University of Missouri IRB approval, our monitoring system has been installed in over 200 TigerPlace apartments and assisted living apartments starting in 2005.
The residents selected in this study are from TigerPlace and other Americare assisted living apartments that use the same monitoring technique. The monitoring sensor network contains various types of sensors mounted in the resident's apartment including motion, bed, and depth-based sensors. Health alerts are automatically generated and sent to clinical staff [32]. In this study, we use bed sensor data which includes pulse, respiration rate, and restlessness.
A sleep measure is needed for tracking the sleep health of older adult residents. Our sleep quality index (SQI) consists of three parts: sleep efficiency, time in bed, and sleep normality. Sleep efficiency is defined as the ratio between sleep time and total time in bed (TiB). As shown in Eq. (1), sleep efficiency is computed by taking the total amount of time spent in bed (in minutes) and subtracting the number of minutes it took to fall asleep plus the minutes spent awake.
$\begin{gathered} { sleep \ efficiency }=\frac{\text { total TiB (minutes) }}{\text { total TiB (minutes) }} -\frac{(\text { minutes to fall asleep }+ \text { minutes awake })}{\text { total TiB (minutes) }}\end{gathered}$ (1)
As a proxy that does not require a classification of sleep versus wake time, we use restlessness in bed, as captured by the bed sensor. Specifically, we use the minutes of restlessness to account for the time when the older adult is in bed and not sleeping. Hence, Eq. (1) for sleep efficiency takes the form of Eq. (2), which we call SQIrestlessness.
$S Q I_{ {restlessness }}=1-\frac{\text { restlessness time (minutes) }}{\text { total TiB (minutes) }}$ (2)
The rationale behind using restlessness as a proxy for sleep efficiency lies in its ability to provide a non-intrusive measure of sleep quality. Traditional methods, such as polysomnography, often require the classification of sleep versus wake time, which can be cumbersome and less accurate, particularly in older adults with irregular sleep patterns [24]. By focusing on restlessness, our approach circumvents the need for extensive sensor setups while still delivering meaningful insights into sleep efficiency.
However, using restlessness as a proxy has its limitations and edge cases. For instance, restlessness may not perfectly correlate with wakefulness in all cases; some individuals might experience minimal movement during wakeful periods, leading to an overestimation of sleep efficiency [33]. Conversely, some sleep disturbances, like periodic limb movement disorder (PLMD), could cause significant restlessness without fully waking the individual, potentially leading to an underestimation of sleep quality [34]. Additionally, restlessness may not capture short, subtle awakenings that are typically recorded in polysomnography-based methods [35]. These edge cases highlight the trade-off between the convenience and non-intrusiveness of using restlessness as a proxy and the detailed accuracy provided by direct sleep vs. wake classification.
Note, however, that the SQIrestlessness percentage does not reflect if someone got enough total sleep. For example, someone who sleeps for 4 out of 5 hours in bed will have the same SQI as when he/she sleeps for 8 out of 10 hours in bed. To account for total sleeping time, we use a weight that penalizes the index value if the older adult sleeps fewer than the recommended number of hours for people in this age range. Based on the latest recommendations from the National Sleep Foundation's updated report, people 65 or older are recommended to sleep seven to eight hours per day [36]. Residents who spend less than this amount of time in bed should expect to have a lower sleep quality. Therefore, for these residents, a penalty is applied to their sleep quality index as shown in Eqs. (3) and (4).
$S Q I_{T i B}=\mathrm{W}_{T i B} *\left(1-\frac{\text { total restlessness time (minutes) }}{\text { total TiB (minutes) }}\right)$ (3)
$W_{T i B}=\left\{\begin{array}{ll}-\left(\frac{\text { total TiB }(\text { hours })-8}{8}\right)^2+1 & \text { if total } \mathrm{TiB} \text { (hours) }<8 \\ 1 & \text { if total } \mathrm{TiB} \text { (hours) } \geq 8\end{array}\right\}$ (4)
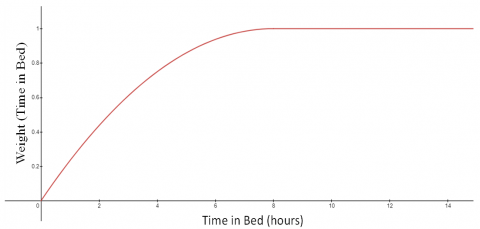
This formula penalizes residents who sleep fewer than 8 hours, with greater weight given to less time in bed. We chose 8 hours as a cutoff in order to balance the formula. For example, a time in bed of 7 hours gives a weight of 0.984, which is less than a 2% adjustment. Six hours gives a weight of 0.938, a more meaningful adjustment, 5 gives 0.859, 4 gives 0.75, and so on to 0 hours giving a weight of 0. For any amount of time in bed at or greater than 8, WTiB is 1. This formula is represented graphically in Figure 1.
Figure 1. Visualization of the effect of time in bed on the selected weight (WTiB)
By incorporating a time-in-bed adjustment, our method ensures that the sleep quality index more accurately reflects the total sleep duration, an essential factor in evaluating sleep health. The penalty applied for insufficient sleep hours helps highlight the importance of adequate sleep duration, which is particularly relevant for older adults who may struggle to achieve the recommended 7-8 hours of sleep.
WTiB is one of two weights that are multiplied by the restlessness percentage in order to create our sleep quality index. The second weight is calculated by using 'sleep normality,' a metric that determines how typical a resident's sleep looks compared to their prior sleep data. Detailed information on this metric is described in the sleep normality section. The sleep normality weight WSN is computed by taking the mean of a resident's sleep normality scores from the previous two weeks and comparing it to the current date's sleep normality as described in Eq. (5).
$W_{S N}=\left\{\begin{array}{c}\frac{S N-S N_{\text {Baseline }}}{S N_{\text {Baseline }}}, \text { if exist }\left(\mathrm{SN} \text { and } \mathrm{SN}_{\text {Baseline }}\right) \\ 1, \text { otherwise }\end{array}\right\} f(x)$ (5)
where, SN is sleep normality, and SNBaseline is the mean sleep normality from the previous two weeks.
The inclusion of sleep normality as a metric allows the SQI to account for variations in sleep patterns over time. By comparing the current night's sleep to a baseline established over two weeks, our method can detect deviations that might indicate emerging health issues. This dynamic adjustment helps ensure that the sleep quality index remains sensitive to changes in sleep behavior, which could be crucial for early detection of health deterioration.
Nights that appear more typical will give a weight greater than 1, while nights that look more unusual give a weight from 0 to 1. Since the typical range of values for sleep normality in the test cases we examined is about 60 to 90 out of 100, this weight is typically no more than a 15% adjustment to SQITiB. In other words, the range of values for WSN was found to be between 0.85 and 1.15.
The combination of both weights with the restlessness percentage gives us our new SQIFinal metric, as shown in Eq. (6). This is the metric that is used in the experimental results section.
$S Q I_{F i n a l}=W_{S N} * \mathrm{SQI}_{T i B}$ (6)
The final sleep quality index, SQIFinal, integrates both time in bed and sleep normality adjustments, offering a comprehensive measure of sleep health that is tailored to the specific needs of older adults. This approach not only captures the quantity and quality of sleep but also considers how consistent sleep patterns are over time, making it a powerful tool for long-term monitoring in eldercare settings.
Sleep normality is a metric we developed to capture how well a resident’s bed sensor data for restlessness (RST), heart rate (HR), and respiration (RSP) in a 24-hour period compares against a baseline taken from the previous two months (60 days) of sensor data. A high sleep normality indicates that a resident's RST, HR, and RSP were similar to the values of the previous 60 days. Conversely, a low sleep normality indicates that the resident had values for RST, HR, or RSP which were either abnormally high or abnormally low for a significant period of their sleep as compared to the resident's baseline. A 60-day window for the baseline was chosen because it provides enough data to accurately assess what 'normal' is for a resident while allowing for a gradual change in the baseline if the resident shifts to a 'new normal'.
First, a baseline is calculated from the resident's previous two months' bed data which is collected in 15-second intervals throughout the entire day. These 15-second intervals are grouped into 5-minute intervals which are only kept if bed data exists for the entire 5 minutes. This is done to reduce variability in the data from periods in which it is unlikely that the resident is sleeping, such as when a resident is getting in to or out of bed. Each of the 5-minute intervals has a mean RST, HR, and RSP calculated from the smaller 15-second intervals that the sensor system provides. Once all the 5-minute intervals from the previous 60 days are collected, they are split between day and night intervals with an adjusting window. This is done so that any differences in the resident's typical RST, HR, and RSP for daytime sleep are not reflected in the baseline against which night sleep will be compared and vice versa. For example, the normal respiration of a napping resident may be significantly different than their normal respiration for overnight sleep. After night-time and daytime 5-minute sleep intervals over the past 60 days are differentiated, the mean and standard deviation RST, HR, and RSP are calculated for both. With a baseline established, the sleep normality for a date can be calculated.
$\begin{aligned} S N_{ {Night }}=(12 & + { RST }_{ {Factor }_{ {Night }}}+H R_{ {Factor }_{ {Night }}} \left.+ { RSP }_{ {Factor }_{\ {Night }}}\right) *\left(\frac{25}{3}\right)\end{aligned}$ (7)
The sleep normality equation consists of 3 factors, one for each data stream (RST, HR, and RSP). Each of the 3 factors is a value from -4 to 0 where -4 is completely abnormal data and 0 is perfectly normal data for that measure. The calculation takes each of the factors and gives an overall sleep normality score on a scale from 0-100. Gathering each of the factors is more complex, so pseudocode for the calculation of one factor is presented below and explained.
Pseudocode for calculating the RST factor for a night:
For each 5-minute interval in the night, the difference between its value and the mean value of the previous two months is taken and divided by the standard deviation. This gives a value for how different that particular 5-minute interval looks compared to all other 5-minute intervals over the past two months. Next, that value is squared to give greater weight to intervals with a larger deviation. A max value of 4 is applied so that extreme outliers do not have too much weight. The effect of these calculations is that for a resident to have low sleep normality they must have many 5-minute intervals in their sleep which deviate significantly from the baseline mean. Once this calculation has been done for every interval in the night/day, the mean of those calculations is taken and multiplied by -1 to give a final value between -4 and 0. A score of 0 indicates that every interval was exactly equal to the mean and a score of -4 indicates that every interval had an absolute difference of at least 2 standard deviations from the mean.
These calculations are repeated 6 times for RST, HR, and RSP for both day and night sleep. Finally, SNDay and SNNight are averaged proportionally by time in bed. The end result is a single sleep normality score out of 100 for a given 24-hour period.
In this section, we introduce the dataset used to evaluate our approach in computing the sleep quality for six older adults from our eldercare monitoring system. We use bed sensor data, which captures the resident's heart rate, respiration, restlessness, and time in bed (TiB). Our goal is to develop a sleep quality index (SQI) that accurately reflects the quality of the resident's sleep in terms of the number of sleeping hours, amount of restlessness, and the normality of the sleep compared to a baseline.
We use the dataset described in the previous section to verify the effectiveness of the proposed SQI in capturing nights where the resident either does not sleep enough, has a high restlessness, and/or has highly unusual sleep. We also pull several case studies to show the effectiveness of the proposed measure in capturing trends in health conditions that affect the resident's sleep quality.
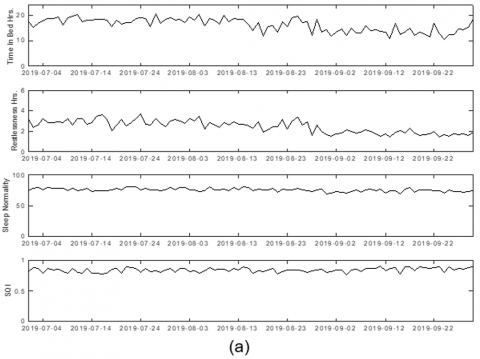
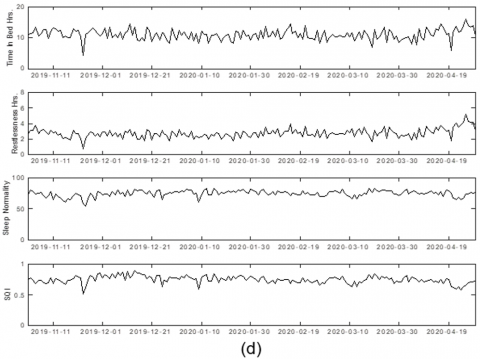
In each figure, we display the total time in bed, total restlessness, sleep normality, and the SQI. Due to the limitation of the manuscript size, we will display 3 months of data for each resident.
Figure 2a shows data for resident I, who spends ample time in bed and has consistent sleep normality with low restlessness. As we expect, this combination of factors causes the resident to sustain a high overall SQI for the entire 3-month period. This is an ideal case that shows how the SQI behaves on a resident with a stable sleep pattern.
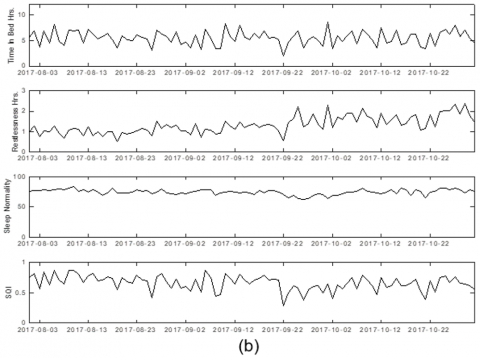
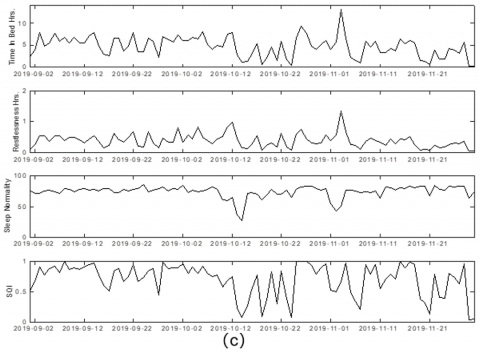
For each resident, the graphs from top to bottom are: Time in Bed (hours), Restlessness (hours), Sleep normality, and the final SQI.
Figure 2. SQI for: a) resident I, b) resident II, c) resident III, and d) resident IV
Figure 2b shows data for resident II, who has a high variability of total time in bed from 4 to 9 hours each 24 hours. This explains the volatility of the sleep quality index. In addition, around the 22nd of September 2020, the resident had a significant increase in restlessness compared to their total time in bed. This change was reflected in the sleep normality as it dropped for about a week after the change and then began to recover as this higher amount of restlessness became 'the new normal'. Despite the volatility and subtlety of the change, an observer can tell that the average sleep quality was lower for a few weeks following the change seen on the 22nd.
Figure 2c shows resident III, who has with a highly volatile sleep pattern as seen in their total time in bed ranging from around 8 hours down to just a couple hours. The wide range of time in bed values well below 8 hours means that WTiB has a large influence on the resident's SQI. On August 26, 2019, an electronic health record (EHR) noted that the resident self-reported that, "some days [they] can sleep well but other days [they] can’t sleep at all." This would explain some of the volatility in sleep quality around that time and into the future. The data for this resident also captured a couple of uniquely sharp drops in sleep normality around October 14 and November 2 which correlated with health conditions found in the EHR data. One of these instances is discussed in the case studies section.
Figure 2d shows resident IV who has a high overall time in bed and consistent restlessness compared to time in bed. Overall, these two factors lead to a relatively stable SQI with most variation coming as a direct result of variations in sleep normality. The variations in sleep for this resident seemed to correlate with EHR data, an example of which can be found in the case studies section.
To investigate the effectiveness of the proposed SQI and sleep normality metric, we pull multiple case studies for the residents in Table 1. Each case study has a time span of about 2 weeks and shows a general trend in our proposed metrics.
Table 1. Dataset description
|
Resident ID |
# Days with Sensor Data |
|
I |
275 |
|
II |
275 |
|
III |
150 |
|
IV |
184 |
|
V |
99 |
|
VI |
182 |
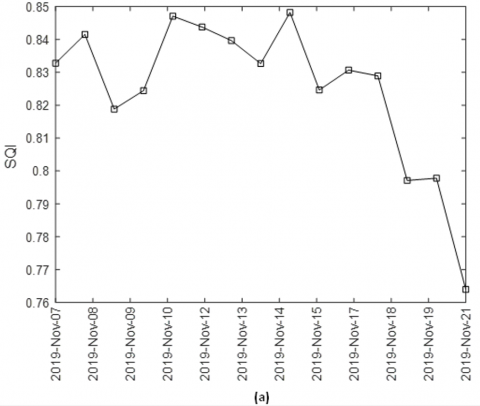
Figure 3a shows the first case study for resident I in Table 1. On November 21, 2019, this resident had a fall incident. It is expected that the sleep quality degrades prior to a fall. We can see in the figure the previous 14 days leading to the incident date, which shows a clear decreasing trend. The trend slope is very sharp the week before the fall. This case study shows the effectiveness of the proposed index in correlating the reduction in the SQI and the possibility of fall. This could be used by our monitoring system to generate an alert any time there is a decreasing trend or reduction in the SQI, which can help in detecting early signs of illness.
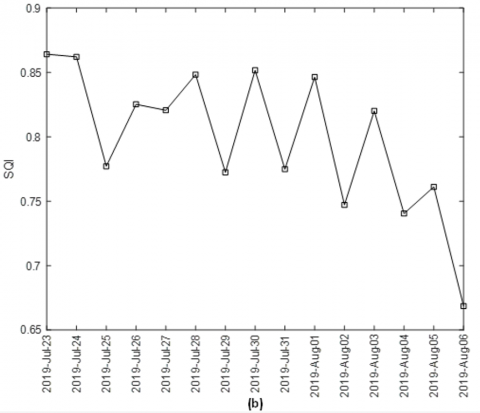
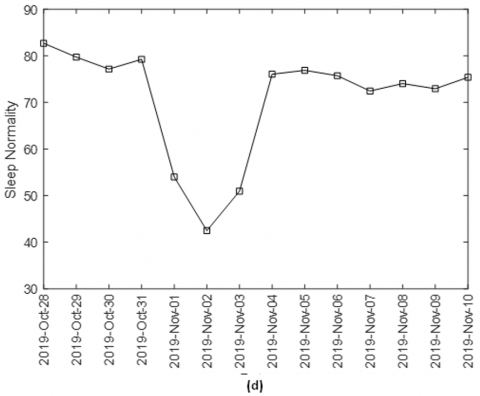
Figure 3. SQI for: a) resident I, b) resident VI, c) resident II, and d) resident IV
Figure 3b shows the second case study for resident VI in Table 1. Around August 06, 2019, the resident had to be taken to the ER. Also, the resident had lower back pain on that day. The SQI values are computed for 14 days leading to the event to check if there is a trend or noticeable change in the sleep quality. We can see that there is a clear decreasing trend captured by the SQI. During these 14 days the resident also experienced multiple health conditions. On July 24, 2019, the resident experienced knee pain which might explain the reduction in SQI value on the following day. The resident was supplied with painkiller medications afterward, which might explain the improvement in the SQI for the next three days. It was reported in the notes that the resident was sleeping well on the nights of 27-28 of July, which showed up in the SQI value for July 27th. The resident had a wound on July 30th and severe pain, which could help explain the reduction in SQI on that day leading to the night of the 31st. Then, a new medication for severe pain was ordered and used on the day of the 31st. After that, the resident was in bed and did not want to eat for some of the remaining days. Also, the resident was confused on the remaining days and was found on the floor multiple times which explains the poor SQI for the days leading to the ER visit.
Figure 3c depicts data for Resident II from April 18 to April 30, 2020. For about a week starting on April 18, we can see that the SQI dropped from around 0.7-0.75 down to around 0.6. On April 21, a note read, "Resident is c/o severe pain and is needing assistance getting in and out of the bed." The note suggests that the resident could be having difficulty sleeping and the drop in the SQI reflects this. A few days later, on April 27 a note read, "[Resident] stated [they] did feel somewhat better but still has quite a bit of pain in the thigh area of [their] right leg." The increase that we see in the sleep quality index around this time reflects the improvement of the resident's health as they continue to recover.
The other case study shows sleep normality data for Resident IV in Figure 3d. From October 31 to November 2, 2019, the resident had a significant drop in their sleep normality which coincides with EHR notes that give context to the chart. On November 2, the day with a local low for sleep normality at just over 40, an EHR note reads, "Resident running a fever this am 101.4 gave [them] some ibuprofen started [them] on [their] antibiotic fever broke after giving ibuprofen." Along with this note, the resident's bed sensors gave readings for RST, HR, and RSP which are highly unusual when compared to the previous 2 months of data for the resident. Later, on November 8, an EHR note read, "Resident's temp is 95.4 [They are] feeling better." At this point, the sleep normality has recovered to a stable level that seems to line up well with what we would expect from the EHR note.
During a period of flu-like symptoms where resident III experienced a noticeable drop in their sleep quality index (SQI), falling from the baseline average of 0.61 to around 0.5. According to an EHR note, the resident was "having a temp during night and cough worse. I requested nurse make SNV to assess him/her. He/she is up and dressed. States she/he had to sleep on three pillows last night to keep from coughing and had temperature. States had several coughing episodes that just couldn't stop coughing. L lung clear but has rhonchi and slight wheeze throughout R lung fields today which had been clear. SN called Dr. X office to try to get an appointment with Someone there today." After about a week of these symptoms, the resident's health began to improve, and a subsequent note stated, "Pt states he/she is feeling better." Correspondingly, the SQI gradually returned to the baseline level, reflecting the recovery of their sleep quality.
In another instance, Resident V experienced a health issue where they "came to the nurse station wanting something for cough. Slept in chair because every time he/she laid down, he/she would have a coughing fit. I called Nurse and she said he/she can go to urgent care if he/she likes." Unlike Resident III, whose similar symptoms resulted in a clear drop in their sleep quality index (SQI), Resident V's SQI remained unaffected because the resident slept in a chair rather than in bed, where our sensors are placed. This case highlights a limitation of our current approach, which relies solely on bed sensors to monitor sleep quality. When residents sleep outside of bed, the system cannot capture changes in sleep quality, leading to gaps in the data and potentially missing important health events.
As we can see, the proposed SQI is effective in capturing a variety of health issues that lead to a drop in sleep quality. However, a key limitation of this approach is its dependency on the resident being in bed. Since we do not use wearable sensors for continuous monitoring, any time spent outside of bed goes unrecorded. To enhance the robustness of our approach, integrating additional sensors, such as radar, depth imaging, or even passive infrared sensors, could allow for more comprehensive monitoring. These technologies would enable us to track the resident's activity and sleep patterns even when they are not confined to their bed, thereby improving the accuracy and reliability of the SQI in various health scenarios.
To provide a broader perspective on the performance of the sleep quality index (SQI), we conducted a comprehensive quantitative analysis across the entire dataset. This analysis supplements the qualitative insights gained from individual case studies.
8.1 Statistical summary of sleep metrics
We calculated key sleep metrics, such as average SQI, average restlessness (in hours), average time in bed (TiB, in hours), and average sleep normality (SN) for each resident. Table 2 provides an overview of these metrics, presenting the mean values along with their standard deviations (SD).
Table 2. Dataset description and statistics
|
Resident ID |
# Days with Sensor Data |
Average Restlessness (hours) |
std Restlessness (hours) |
Average TiB (hours) |
std TiB (hours) |
Average SN (hours) |
std SN (hours) |
Average SQI |
Std SQI |
|
I |
275 |
2.2287 |
0.4194 |
16.0263 |
2.5995 |
78.1718 |
4.6428 |
0.8571 |
0.0750 |
|
II |
275 |
3.0199 |
0.7413 |
13.0455 |
2.3975 |
78.7580 |
5.1400 |
0.7720 |
0.0541 |
|
III |
150 |
1.3648 |
0.4672 |
5.6929 |
1.1600 |
75.9233 |
3.8199 |
0.6133 |
0.1346 |
|
IV |
184 |
2.7329 |
0.9299 |
14.7000 |
4.0417 |
77.6944 |
4.6526 |
0.8096 |
0.0838 |
|
V |
99 |
0.1990 |
0.1418 |
2.2005 |
1.4518 |
76.3866 |
8.0024 |
0.2887 |
0.1916 |
|
VI |
182 |
2.1029 |
0.5717 |
12.7788 |
3.3438 |
79.0739 |
3.1773 |
0.8244 |
0.0833 |
The dataset reveals significant differences in sleep behaviors among the residents. For example, Resident I spent an average of 16.03 hours in bed daily, with moderate restlessness (2.23 hours), leading to a high SQI of 0.8571, indicative of good sleep quality. In contrast, Resident III had a much lower average TiB of 5.69 hours and a lower SQI of 0.6133, suggesting poorer sleep quality despite having less restlessness (1.36 hours).
Resident V, who had the shortest average TiB (2.20 hours) and the lowest SQI (0.2887), highlights the importance of sufficient sleep duration in maintaining sleep quality, even though their restlessness was minimal (0.20 hours). On the other hand, Residents II and IV exhibited higher restlessness (3.02 hours and 2.73 hours, respectively) but still maintained reasonable sleep quality with SQIs of 0.7720 and 0.8096, respectively, due to longer times in bed (13.05 hours and 14.70 hours).
Resident VI, with an average TiB of 12.78 hours and moderate restlessness (2.10 hours), achieved an SQI of 0.8244, reflecting a balanced sleep pattern with consistent sleep quality. Their sleep normality score also suggests fewer deviations from their baseline, contributing to their relatively high SQI.
8.2 Comparative analysis
To further understand the relationship between health conditions and sleep quality, we performed a comparative analysis between Resident III, who has frequent health issues, and the other residents, excluding Resident V, who generally do not sleep on their bed and have unreliable SQI measure. Resident III's sleep quality index (SQI) was compared with the aggregated SQI of Residents I, II, IV, and VI.
The results of the analysis revealed a significant difference in SQI between Resident III and the other residents. Specifically, Resident III had a mean SQI of 0.6133, while the average SQI for the group of residents with fewer health issues was 0.8158. The t-test yielded a t-statistic of -17.98 and a p-value of 1.22e-40, indicating that this difference is highly statistically significant. This suggests that the health issues experienced by Resident III are strongly associated with a lower SQI compared to the other residents.
These findings reinforce the earlier observations, highlighting the impact of frequent health problems on sleep quality. The significant decrease in SQI for Resident III compared to the healthier group underscores the utility of the SQI as a sensitive measure for detecting and monitoring health-related changes in sleep quality in older adults.
The sleep quality index (SQI) developed in this study offers several potential applications in clinical practice, particularly within the context of eldercare monitoring and early intervention. Its ability to provide continuous, non-intrusive monitoring of sleep quality makes it a valuable tool for enhancing patient care and detecting early signs of health deterioration.
One significant application of the SQI is its integration into existing eldercare monitoring systems. By continuously tracking changes in sleep quality, the SQI can serve as an early warning tool for healthcare providers. This capability allows clinicians to identify residents who may be experiencing health decline, enabling timely interventions before health issues become critical. The early detection of such changes can lead to more proactive care and potentially prevent the escalation of health problems.
Furthermore, the SQI's ability to facilitate remote monitoring presents substantial opportunities for telehealth applications. Clinicians can utilize the SQI to monitor patients from a distance, thereby reducing the need for frequent in-person visits while still ensuring that any concerning trends in sleep quality are promptly addressed. This remote capability is especially valuable in managing the health of older adults, where regular in-person check-ups might be challenging.
In addition to monitoring, the SQI can play a crucial role in preventative care and early intervention strategies. By incorporating the SQI into routine care protocols, healthcare providers can enhance the early detection of health issues, such as sleep disorders or the initial stages of cognitive decline. The continuous monitoring offered by the SQI allows for early identification of sleep disruptions, enabling healthcare providers to initiate interventions at the earliest signs of potential health problems, ultimately improving patient outcomes and quality of life.
In our assisted living facilities, older adults are monitored using unobtrusive sensors. Bed sensors are placed under the mattress, which capture time in bed, heart rate, respiration rate, and restlessness in bed. Sleep is an important aspect of the mental and physical health of older adults. Therefore, in this paper, we introduce a new way to capture sleep quality using a Ballistocardiography sensor, which does not require explicit sleep stages. We avoided using wearable devices existing in the market for monitoring because of the extra burden on older adults to remember to charge the device and wear it during sleep.
We evaluated the proposed index on six residents with bed sensor data. The index was able to capture days where the resident did not sleep enough or had highly unusual sleep. We also pulled multiple case studies from our Electronic Health Record (EHR). Our preliminary findings suggest a correlation between the EHR data and the sleep index value, where a decreasing trend in the index may relate to declining health.
A comparative analysis demonstrated the relationship between health conditions and sleep quality by comparing Resident III, who has frequent health issues, with the other residents (excluding Resident V). The analysis revealed a significant difference in SQI between Resident III and the other residents, with Resident III showing a lower mean SQI of 0.6133 compared to the healthier group's average of 0.8158. The statistical significance of this difference underscores the utility of the SQI as a sensitive measure for detecting and monitoring health-related changes in sleep quality among older adults.
While the proposed SQI effectively captures variations in sleep quality, a key limitation of our approach is its reliance on the resident being in bed. When residents are not sleeping in their beds due to illness, hospitalization, or other health conditions, the system cannot monitor their sleep quality. This limitation highlights the need for integrating additional sensors, such as radar, depth imaging, or passive infrared sensors, to ensure continuous monitoring regardless of the resident's location.
The SQI developed in this study also presents several potential applications in clinical practice. It can be integrated into eldercare monitoring systems as an early warning tool, helping healthcare providers to identify and address declining health in residents. The ability to remotely monitor sleep quality via the SQI further enhances telehealth applications, allowing clinicians to track patients' well-being without requiring frequent in-person visits. Moreover, incorporating the SQI into preventative care strategies can improve early detection of health issues, such as sleep disorders or the onset of cognitive decline, leading to timely interventions and better patient outcomes.
In future work, we plan to investigate the effectiveness of incorporating sleep stages into the sleep quality index. We also plan to compare the proposed measures (with and without sleep stages) to Polysomnography data collected in a sleep lab.
[1] Vincent, G.K., Velkoff, V.A. (2010). The next four decades: The older population in the United States: 2010 to 2050. U.S. Department Commerce, Economics and Statistics Administration, U.S. Census Bureau, pp. 1125-1138. https://www.census.gov/library/publications/2010/demo/p25-1138.html.
[2] Hayes, T.L., Pavel, M., Kaye, J.A. (2004). An unobtrusive in-home monitoring system for detection of key motor changes preceding cognitive decline. In the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, pp. 2480-2483. https://doi.org/10.1109/iembs.2004.1403715
[3] Ibrahim, O.A., Keller, J., Popescu, M. (2019). An unsupervised framework for detecting early signs of illness in eldercare. In 2019 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), San Diego, CA, USA, pp. 1043-1050. https://doi.org/10.1109/bibm47256.2019.8983010
[4] Scullin, M.K. (2017). Do older adults need sleep? A review of neuroimaging, sleep, and aging studies. Current Sleep Medicine Reports, 3(3): 204-214. https://doi.org/10.1007/s40675-017-0086-z
[5] Yaffe, K., Falvey, C.M., Hoang, T. (2014). Connections between sleep and cognition in older adults. The Lancet Neurology, 13(10): 1017-1028. https://doi.org/10.1016/s1474-4422(14)70172-3
[6] Liu-Ambrose, T., Falck, R.S. (2019). Sleep, physical activity, and cognitive health in older adults. In Handbook of Behavioral Neuroscience, pp. 665-676. https://doi.org/10.1016/b978-0-12-813743-7.00044-x
[7] Efe, E., Özşen, S. (2021). A new approach for automatic sleep staging: Siamese neural networks. Traitement du Signal, 38(5): 1423-1430. https://doi.org/10.18280/ts.380517
[8] Kemidi, M., Marur, D.R., Chantigari, V.K.R. (2023). Detection and classification of obstructive sleep apnea disorders: A comparative analysis of various deep machine learning classifiers. Revue d’Intelligence Artificielle, 37(1): 201-208. https://doi.org/10.18280/ria.370125
[9] Arslan, R.S., Ulutaş, H., Köksal, A.S., Bakır, M., Çiftçi, B. (2023). Tree-based machine learning techniques for automated human sleep stage classification. Traitement du Signal, 40(4): 1385-1400. https://doi.org/10.18280/ts.400408
[10] Lowe, C.J., Safati, A., Hall, P.A. (2017). The neurocognitive consequences of sleep restriction: A meta-analytic review. Neuroscience & Biobehavioral Reviews, 80: 586-604. https://doi.org/10.1016/j.neubiorev.2017.07.010
[11] Banks, S., Dinges, D.F. (2007). Behavioral and physiological consequences of sleep restriction. Journal of Clinical Sleep Medicine, 3(5): 519-528. https://doi.org/10.5664/jcsm.26918
[12] Killgore, W.D.S. (2010). Effects of sleep deprivation on cognition. In Progress in Brain Research, pp. 105-129. https://doi.org/10.1016/b978-0-444-53702-7.00007-5
[13] Falck, R.S., Barha, C.K., Chan, P.C.Y., Liu-Ambrose, T. (2020). Refining sleep measurement using the Motionwatch8©: How many days of monitoring do we need to get reliable estimates of sleep quality for older adults with mild cognitive impairment? Sleep Science and Practice, 4(1). https://doi.org/10.1186/s41606-020-00048-w
[14] Naismith, S.L., Hickie, I.B., Terpening, Z., Rajaratnam, S.W., Hodges, J.R., Bolitho, S., Rogers, N.L., Lewis, S.J.G. (2014). Circadian misalignment and sleep disruption in mild cognitive impairment. Journal of Alzheimer’s Disease, 38(4): 857-866. https://doi.org/10.3233/jad-131217
[15] Tranah, G.J., Blackwell, T., Stone, K.L., Ancoli-Israel, S., Paudel, M.L., Ensrud, K.E., Cauley, J.A., Redline, S., Hillier, T.A., Cummings, S.R., Yaffe, K. (2011). Circadian activity rhythms and risk of incident dementia and mild cognitive impairment in older women. Annals of Neurology, 70(5): 722-732. https://doi.org/10.1002/ana.22468
[16] Roh, J.H., Huang, Y., Bero, A.W., Kasten, T., Stewart, F.R., Bateman, R.J., Holtzman, D.M. (2012). Disruption of the sleep-wake cycle and diurnal fluctuation of β-amyloid in mice with Alzheimer’s disease pathology. Science Translational Medicine, 4(150). https://doi.org/10.1126/scitranslmed.3004291
[17] Ju, Y.E.S., Lucey, B.P., Holtzman, D.M. (2014). Sleep and Alzheimer disease pathology—A bidirectional relationship. Nature Reviews Neurology, 10(2): 115-119. https://doi.org/10.1038/nrneurol.2013.269
[18] Joo, H.J., Joo, J.H., Kwon, J., Jang, B.N., Park, E.C. (2021). Association between quality and duration of sleep and subjective cognitive decline: A cross-sectional study in South Korea. Scientific Reports, 11(1): 16989. https://doi.org/10.1038/s41598-021-96453-x
[19] Ma, Y.J., Liang, L.R., Zheng, F.F., Shi, L., Zhong, B.L., Xie, W.X. (2020). Association between sleep duration and cognitive decline. JAMA Network Open, 3(9): e2013573. https://doi.org/10.1001/jamanetworkopen.2020.13573
[20] McCarthy, C.E. (2021). Sleep disturbance, sleep disorders and co-morbidities in the care of the older person. Medical Sciences, 9(2): 31. https://doi.org/10.3390/medsci9020031
[21] Zinkhan, M., Berger, K., Hense, S., Nagel, M., Obst, A., Koch, B., Penzel, T., Fietze, I., Ahrens, W., Young, P., Happe, S., Kantelhardt, J.W., Kluttig, A., Schmidt-Pokrzywniak, A., Pillmann, F., Stang, A. (2014). Agreement of different methods for assessing sleep characteristics: A comparison of two actigraphs, wrist and hip placement, and self-report with polysomnography. Sleep Medicine, 15(9): 1107-1114. https://doi.org/10.1016/j.sleep.2014.04.015
[22] Landry, G.J., Best, J.R., Liu-Ambrose, T. (2015). Measuring sleep quality in older adults: A comparison using subjective and objective methods. Frontiers in Aging Neuroscience, 7: 166. https://doi.org/10.3389/fnagi.2015.00166
[23] Buysse, D.J., Reynolds III, C.F., Monk, T.H., Berman, S.R., Kupfer, D.J. (1989). The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2): 193-213. https://doi.org/10.1016/0165-1781(89)90047-4
[24] Kushida, C.A., Littner, M.R., Morgenthaler, T., et al. (2005). Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep, 28(4): 499-523. https://doi.org/10.1093/sleep/28.4.499
[25] Sadeh, A., Hauri, P.J., Kripke, D.F., Lavie, P. (1995). The role of actigraphy in the evaluation of sleep disorders. Sleep, 18(4): 288-302. https://doi.org/10.1093/sleep/18.4.288
[26] Pinheiro, E., Postolache, O., Girão, P. (2010). Theory and developments in an unobtrusive cardiovascular system representation: Ballistocardiography. The Open Biomedical Engineering Journal, 4(4): 201-216. https://doi.org/10.2174/1874120701004010201
[27] Ancoli-Israel, S., Cole, R., Alessi, C., Chambers, M., Moorcroft, W., Pollak, C.P. (2003). The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 26(3): 342–392. https://doi.org/10.1093/sleep/26.3.342
[28] Inan, O.T., Migeotte, P.F., Park, K.S., Etemadi, M., Tavakolian, K., Casanella, R., Zanetti, J., Tank, J., Funtova, I., Prisk, G.K., Di Rienzo, M. (2015). Ballistocardiography and seismocardiography: A review of recent advances. IEEE Journal of Biomedical and Health Informatics, 19(4): 1414–1427. https://doi.org/10.1109/JBHI.2014.2361732
[29] Rantz, M.J., Marek, K.D., Aud, M.A., Johnson, R.A., Otto, D., Porter, R. (2005). TigerPlace: A new future for older adults. Journal of Nursing Care Quality, 20(1): 1-4. https://doi.org/10.1097/00001786-200501000-00001
[30] Skubic, M., Alexander, G., Popescu, M., Rantz, M., Keller, J. (2009). A smart home application to eldercare: Current status and lessons learned. Technology and Health Care, 17(3): 183-201. https://doi.org/10.3233/thc-2009-0551
[31] Rantz, M.J., Marek, K.D., Aud, M., Tyrer, H.W., Skubic, M., Demiris, G., Hussam, A. (2005). A technology and nursing collaboration to help older adults age in place. Nursing Outlook, 53(1): 40-45. https://doi.org/10.1016/j.outlook.2004.05.004
[32] Skubic, M., Guevara, R.D., Rantz, M. (2015). Automated health alerts using in-home sensor data for embedded health assessment. IEEE Journal of Translational Engineering in Health and Medicine, 3: 1-11. https://doi.org/10.1109/jtehm.2015.2421499
[33] Conley, S., Knies, A., Batten, J., Ash, G., Miner, B., Hwang, Y., Jeon, S., Redeker, N.S. (2019). Agreement between actigraphic and polysomnographic measures of sleep in adults with and without chronic conditions: A systematic review and meta-analysis. Sleep Medicine Reviews, 46: 151-160. https://doi.org/10.1016/j.smrv.2019.05.001
[34] Chervin, R.L. (2001). Periodic leg movements and sleepiness in patients evaluated for sleep-disordered breathing. American Journal of Respiratory and Critical Care Medicine, 164(8): 1454-1458. https://doi.org/10.1164/ajrccm.164.8.2011062
[35] Ancoli-Israel, S., Cole, R., Alessi, C., Chambers, M., Moorcroft, W., Pollak, C.P. (2003). The role of actigraphy in the study of sleep and circadian rhythms. Sleep, 26(3): 342-392. https://doi.org/10.1093/sleep/26.3.342
[36] Hirshkowitz, M., Whiton, K., Albert, S.M., et al. (2015). National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health, 1(4): 233-243. https://doi.org/10.1016/j.sleh.2015.10.004