Jerin Tasnim | Fahamida Yeasmin Nishat | Muhammad Sheikh Sadi* | Prottoy Saha
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
COVID-19 has become one of the most alarming pandemics throughout history. Thus, detecting, preventing, and curing COVID-19 has gradually become one of the most important research fields. Artificial intelligence and medical science are both contributing significantly to achieve success in these areas. Research in this area may assist in preventing the fast spread of COVID-19 by providing effective treatments. This paper discusses recent works that emphasize the contribution of artificial intelligence, IoT, and other techniques to preventing COVID-19 outbreaks. The paper classifies different research on the detection, prevention, and cure of COVID-19. Moreover, it shows the taxonomy and relative analysis among those systems and analyzes the impact of these systems on the pandemic situation. This paper aims to present an easily understandable and comparative description of the recent works on the battle against coronavirus.
COVID-19, review, deep learning, artificial intelligence, IoT
COVID-19 outbreak has created the most devastating pandemic history that the world has ever seen till now [1-3]. The pandemic is affecting health, the economy, and general lifestyle all around the globe. Because of the crown shape of the virus, it is called "coronavirus". The first appearance of the coronavirus was observed among chickens as intense respiratory pestilence in 1930. In 1960, coronavirus-infected human patients were found for the first time. The significant appearance of coronavirus occurred as severe acute respiratory syndrome coronavirus (SARS-CoV) and Middle East respiratory syndrome coronavirus (MERS-CoV) in 2002 and 2012 respectively with the zoonotic origin. Finally, the outbreak started in Wuhan, China in 2019, and the spread of this disease is continued till now.
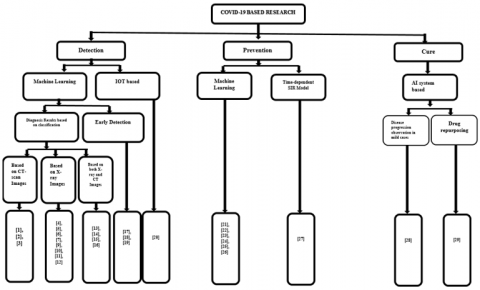
The COVID-19 outbreak was declared a pandemic on March 11, 2020. Because of the uncontrollable chaotic situation, coronavirus has become the first priority of scientists around the world. To defeat the outbreak, firstly the detection of coronavirus infection plays a crucial role. Thus, scientists worked on various detection methods. Most of the research is based on finding the solution to cope with the recent situation by providing various techniques. In this paper, these researches are categorized according to detection, prevention, and cure techniques. Furthermore, they are classified based on the adopted methodology. The detection methods, based on Machine Learning (ML), mostly use X-ray images [1-3], CT-Scan images [4-12], the combination of X-ray images, and CT-Scan images [13-16] for faster identification of the COVID-19 infection. The detection method includes an early detection process [17-19], and IoT based detection [20]. The prevention method includes ML, NLP, and some other methods [21-27]. The cure methods tend to find out useful medicines using drug repurposing based on AI and other processes [28, 29].
The paper is summarized as follows. Section 2 represents a survey on COVID-19 detection, prevention, and cure methods. Section 3 elaborates the discussion on the subjective review performed in this paper. Section 4 concludes the paper.
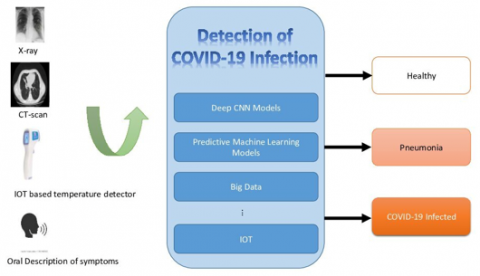
Researchers have developed various systems for COVID-19 detection, prevention, and cure procedure (Figure 1). Some systems have utilized deep learning and ML techniques (Figure 2). Some other systems have proposed IoT-based systems. The paper reviews the systems into three categories: i) detection, ii) prevention, and iii) cure techniques of COVID-19.
2.1 COVID-19 detection based system
Detecting Covid-19 with its types is a challenging task. Some of the research has led to a better and clear distinction between the types of Covid-19. This paper has classified the COVID-19 detection system into two categories: i) ML-based detection and ii) IoT-based detection.
2.1.1 ML-based detection
Researchers have developed various ML-based systems to detect COVID-19. Some systems have classified COVID-19 into normal or pneumonia cases. Some systems have been proposed for the early detection of COVID-19. The systems mainly extract deep and unique features from X-ray or CT-scan images and then classify COVID-19. We have classified ML-based detection systems into three sections: i) diagnosis based on CT-scan and X-ray images individually, ii) diagnosis based on both X-ray and CT images, and iii) early detection of COVID-19.
Diagnosis based on CT-scan and X-ray images individually In this category, diagnosis systems have been categorized into two sections: i) based on both CT-scan images, and ii) based on X-ray images. These are described shortly as follows.
Barstugan et al. [1] used CT pictures to classify COVID-19. The system will find 3 cases: COVID-19 cases, influenza, and healthy cases. The researchers classified them by a three-dimensional deep learning model. The model showed 87.6% accuracy. The feature extraction ways used here were: gray Level Co-occurrence Matrix, native Directional Pattern, Grey Level Run Length Matrix, grey Level Size Zone Matrix, and distinct wave rework. The extracted options were classified by the SVM (Support Vector Machine). Among all the feature extraction ways, the grey Level Size Zone Matrix methodology gave the simplest classification accuracy of 99.68% with 10-fold cross-validation. However, this analysis faced AN overfitting problem because of an absence of comfortable knowledge assortment.
An advised methodology by Özkaya et al. [2] detects coronavirus malady from CT pictures. The system developed a feature fusion and ranking methodology. The model advised a pre-trained CNN model that took the patch-based pictures as input. The feature vectors obtained from CNN provided new options with fusion in line with the correlation coefficients. Then it became hierarchical by the t-test methodology. Each of the fusion and ranking deep options was evaluated by SVM. The analysis showed 96.54% Matthews correlation (MCC) metrics, 98.28% F1-score, and 98.27% accuracy. However, the analysis was evaluated with a small dataset.
Pokhrel et al. [3] showed how to identify the panic zone inefficiently. Also, it enhances the diagnosis detection by analyzing the previous results of detection Kits, RT-PCR, and Immunoassay test results. The research also describes how to identify the most dangerous zone of a specific area. Also, by predicting the transmission rate, it can provide an assumption of the upcoming spread rate of COVID-19. The research provides a plan to build point-of-care to the most crucial places for the spreading of the pandemic to mitigate the maximum harm. The research indicates the progress of COVID-19 detection through RT-PCR and CT scan images has been possible till now. It shows that CT image results are 98% more sensitive than the RT-PCR method. It also identified that the Immunoassay test results show 100% specificity in the case of COVID-19 patients.
Mangal et al. [4] developed a system to check the coronavirus-infected patient additional with efficiency from X-ray reports and didn't have any feature to control CT-image results. The system classified the input image into 3 sections: traditional, (bacterial/viral) respiratory illness, and COVID-19. The system developed a deep neural network-based AI detector. The analysis conjointly showed much better performance than Covid-Net in terms of both the F1-score and mythical creature curve.
Alqudah et al. [5] projected a man-made Intelligence-based system for quicker detection of COVID-19 cases from X-ray pictures. The system developed a hybrid AI model. AI models were trained with extracted options. To extract deep options of the X-ray pictures, a complicated optical coherence imaging network (AOCT-Net) model was projected. The AOCT-Net extracted the machine-driven graphical options from the connected (FC) layer. Then support vector machine (SVM) and random forest (RF) are applied to build a classifying model with those deep options. These hybrid models showed a much better performance score with 95.2% of accuracy.
Majeed et al. [6] introduced a brand new methodology to spice up the radiography-based designation with the assistance of ML. The system used X-ray pictures to judge the CNN design. The model was trained through the CNN transfer learning procedure. The projected CNN design classified healthy cases and COVID-19 cases. The category activation maps (CAM) will find the precise region wherever the X-ray pictures vary. The CNN architectures that were utilized in this model are twelve of-the-shelf CNN models. They projected a CNN design referred to as CNN-X for X-ray testing to induce a much better result. The model wasn't evaluated with correct performance metrics. Hence, it had been arduous to match this analysis with alternative works.
Sahinbas and Catak [7] introduced a deep learning-based system that worked on raw X-ray pictures and runs 5 different pre-trained CNN architectures for the classification and detection of COVID-19 cases. They are VGG16, VGG19, ResNet, DenseNet, and InceptionV3. The transfer learning was done by coaching the pre-trained models with a little dataset. Among them, the VGG16 model showed higher accuracy of eightieth to classify COVID-19 cases.
Ozturk et al. [8] presented an automated coronavirus detection system using a neural network coupled with radiological images. The ‘DarkNet’ deep neural network model was considered a classifier. Chest X-ray images were considered databases. The model had 17 convolutional layers and was trained for 100 epochs. The model was trained in two steps. At first, it classifies the images into COVID-19, No-Findings, and Pneumonia class levels, and then the model was trained only for COVID-19 and No-Findings cases. The grad-CAM heat map approach was also used to depict the decisions of the deep model. The model generates 98.08% accuracy for binary classes and 87.02% for multi-class cases. Since COVID-19 is considered a subset of pneumonia, the diagnosis method was correct but the interpretation might be incorrect. The system required high-quality images.
Mahmud et al. [9] proposed a CovXNet model for coronavirus diagnosis which is based on a deep neural network. The network follows depth-wise convolution that has a variety of dilation rates and the network was efficient to analyze X-rays from different perspectives. The model specially used a stacking algorithm to get more optimization. The method followed the process in the way that, first images were pre-processed, then the depth was increased for spatial reduction and the output feature map depth was increased to increase filtering operations. After training individual networks, the networks predicted from different perspectives, and finally, the networks generated the output that was used for proper optimization. The process is called the meta-learning process. As COVID-19 X-rays are inadequate, fine-tuning layers were added to train the model. To highlight the abnormal areas, a gradient-based discriminative was used too. The system provided very satisfactory detection performance with an accuracy of 97.4% for COVID/Normal, 96.9% for COVID/Viral pneumonia, 94.7% for COVID/Bacterial Pneumonia, and 90.2% for multiclass COVID/normal/Viral/Bacterial pneumonia.
Khan et al. [10] proposed a deep convolution neural network that predicts COVID-19 using X-ray images. The system proposed three models. They are a multi-class model or 4-class CoroNet model for COVID-19, normal, pneumonia-bacterial, and pneumonia-viral classification; 3-class CoroNet model for COVID-19, normal, pneumonia classification; and binary 2-class CoroNet model for COVID-19, normal, and pneumonia classification. The model is based on the Xception pre-trained model. The presented Xception model of 71 layers follows the Max pooling layer and fully connected layer and uses softmax to predict the class of X-ray images. The model shows an average accuracy of 89.6% for the 4-class CoroNet model and 90% 4-class CoroNet model.
Rajaraman et al. [11] proposed a custom convolutional neural network including Talos optimization package, dropout ratio layer, non-linear soft-max activation function and pre-trained ImageNet to detect COVID-19 from chest X-rays. Instead of max-pooling, strided separable convolution was used. SGD optimizer was also used to improve performance. Iteratively pruned deep learning model reduces complexity and increases the efficiency of memory. The model was iteratively pruned with the highest average percentage of zeros and meta-learner. This optimally combines the individual pruned models. Gradient manipulation for visualization. To segment lung pixels, U-Net semantic segmentation was used. 95% confidence interval was computed to explain the performance of models. The model showed an overall accuracy of 99.01% and an area under the curve of 0.9972 in detecting COVID-19.
Rahimzadeh and Attar [12] introduced a model of a concatenation of Xception and ResNet50V2 networks. The Xception and ResNet50V2 networks generated the same size as the feature map. Extracted features were concatenated to the convolutional layer and were connected to the classifier. The dataset consists of X-ray and CT scan images of patients infected with COVID-19, SARS, Streptococcus, ARDS, Pneumocystis, and other types of pneumonia from different patients. The model differentiated pneumonia and normal cases with COVID-19 cases in each phase. Four different matrices were used to evaluate the network. The training set was divided into 8 successive phases and number of each class was almost same to get better results for the detection of COVID-19. The model had an average accuracy of 99.50% on the proposed network and an overall average of 91.4%.
Diagnosis based on both X-ray and CT images He et al. [13] projected a deep learning model to spot COVID-19 cases. The CT-scan pictures of patients were used as a knowledge set to benchmark 2 styles of progressive deep learning models. They are: 3D CNN together with DenseNet3D121, R2Plus1D, MC3 18, ResNeXt3D101, PreAct ResNet, ResNet3D series; and 2nd CNN, together with DenseNet121, DenseNet201, ResNet50, ResNet101 and ResNeXt101. The analysis showed that the 3D CNN performed higher than the 2nd CNN. The gain of an upper foreign terrorist organization was doable if the slices were regenerated to grayscale pictures. The analysis jointly deployed a fault knowledge augmentation methodology.
Salih et al. [14] proposed a system that worked on a specific CNN model for the detection of COVID-19 cases. It was a specialized deep learning-based CNN that worked on CT images and X-ray images. The modified AlexNet model was represented with different types of pooling layers and the second fully connected layer. The MATLAB software was used to conduct the results from the experience. It analyzed a larger amount of dataset to provide more accurate results. The architecture was significantly effective obtaining accuracy of 96% and 97.27% for X-ray and CT scans respectively. It outperformed the existing AlexNet CNN model.
Alom et al. [15] introduced a brand new methodology to find COVID-19 from X-ray pictures and CT scan pictures. The infected regions are known and analyzed through the deep learning model with the detection and localization methodology. The training of the model was done by grouping the general public samples. The chest segmentation was done by the victimization of the NABLA-N model. In this case, the training was done by mathematical morphological approaches. Thus, it had been known as a NABLA-N-based segmentation model and IRRCNN primarily based detection model that showed 84.67% and 98.78% accuracy for X-ray and CT pictures severally.
Öztürk et al. [16] introduced a system that classified the coronavirus malady from X-ray and CT pictures. The analysis classified the pictures into six different categories. It showed that the results of X-ray and CT pictures are identical for the initial and coronavirus case. Respiratory illness or alternative cases varied within the result. The analysis was performed by victimization CNN and deep learning design. The extraction feature methodology was gray Level Co-occurrence Matrix (GLCM), native Binary Grey Level Co-occurrence Matrix (LBGLCM), grey Level Run Length Matrix (GLRLM), and Segmentation-based pattern Texture Analysis (SFTA). The classification was done by SVM. The analysis showed 90% accuracy.
Early detection of COVID-19 based on analyzing the symptoms Hashmi et al. [17] presented a goal to identify the connection between the symptoms and COVID-19. Thus, healthcare organizations or clinical practitioners can detect COVID-19 for taking proper steps to mitigate major casualties at an early stage. The model predicts which symptoms are much more likely to occur in COVID-19 patients such that patients having vulnerable positions can be identified and faster actions can be taken. The features were assigned with respected scores accordingly with the help of Borg scoring method. But it is slightly modified with the help of an upgraded Hashmi-Asif COVID-19 assessment Chart. To find the actual connections of the sign and symptoms with the presence of the COVID-19 virus in a human body the Pearson correlation and Spearman Correlation coefficient is used. And the Linear regression analysis showed exactly which correlating features would be more accurate. The frequency rate of the symptoms being related to the disease is assessed through the Chi-square test two-tailed with Cramer’s V strength. The result of this experiment shows the relation between the symptoms and the virus like: Fever in 43.9% (P = 0.000) cases, cough 54.08% and dry mucus 25.68% equally significant (P = 0.000), Hyperemic pharyngeal mucus membrane 17.92% (P = 0.005), leukopenia 28.11% (P = 0.000), lymphopenia 64.35% (P = 0.000), thrombopenia 35.49% (P = 0.000), elevated Alanine aminotransferase 50.02% (P = 0.000), and Aspartate aminotransferase 34.49% (P = 0.000). So, it shows how much a person with probable symptoms is more likely to be infected with a very effective prediction.
Roland et al. [18] worked on a predictive model to detect corona patients. It takes the symptoms as input data and provides a possibility of being infected with the coronavirus.
The predictive model was built by analyzing symptoms, demographic information, comorbidities, and COVID-19 test results. The predictor was selected through logistic regression. The classifiers were implemented using receiver operating characteristic analysis (ROC). The presence of fever, smell or taste changes, and body aches shows a higher possibility of being COVID-19 positive. On the other hand, shortness of breath and sore throat symptoms shows a higher possibility of COVID-19 negative. Unreasonable body aches show the highest sensitivity of 80% and the reduction of smell and taste sense shows the specificity of 73%. So, those specific symptoms showing a higher possibility are the ones riskier.
Escobar et al. [19] showed an AI based pooling technique to test COVID-19. Pooling based molecular testing is one of the most effective ways to test COVID-19. With the help of ML, this can become far accurate. Hence, the two-steps pooling are applied to create a smarter pooling system with the help of AI. It shows 42% accuracy gaining in case of testing a patient for COVID-19 where the possible disease prevalence can be up to 25%. It enhances the accuracy of diagnosis of CT images. The use of symptomatology can predict whether the patient is infected or not. This can be done with the help of a regression model that is trained with the previous clinical database of other patients. That is also useful to have a forecast of the pandemic situation in a specific zone. It is essential to understand that the research does not produce any new technique, but rather enhances the efficiency of older techniques. So, it can’t be compared within the same metric as other techniques. It fulfills almost all the criteria that it targeted to succeed.
Figure 1. Summary of COVID-19 research work
Figure 2. Deep Learning and Convolutional Neural Network (CNN) research
2.1.2 IoT-based COVID-19 detection
Mohammad et al. [20] showed that as temperature increases due to COVID-19, a temperature-based system can be useful for detecting COVID-19. To minimize the spread of COVID-19, a system with instant identification and alert notification is needed. This paper developed a smart helmet and a camera which is developed as optical and thermal. Then the camera is mounted on the smart helmet. The camera can recognize a person. The images are set to the helmet. The helmet processes the data. If there is any person with a temperature more than normal, a notification is sent to the smartphone. GPS is used to determine the position. Through the IoT system, a notification is sent. Arduino IDE is adopted here. This system does the job very fast and reduces human error. The visited location by identified infectee is collected by GLH (Google Location History). These google features are done by mainly google accounts. Blynk server is utilized to transfer the information from the micro-controller over the web to provide it independently.
2.2 COVID-19 prevention techniques
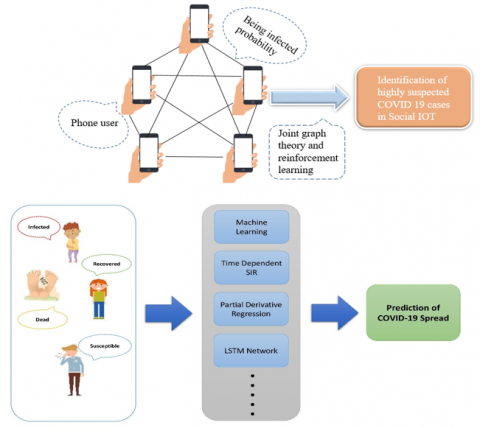
The observation and analysis of the COVID-19 cases around the world helped the healthcare organizations around the world to take early steps to prevent the massive spreading of the pandemic. The prediction-based analysis helped them to understand the characteristics of the uprising graph of infected people to fight the possibilities of major harm from the very beginning. Many AI-based prediction models helped them to be successful in the path of reducing the spreading rate (Figure 3). The prevention techniques are divided into two categories: i) ML-based Prevention Techniques, and ii) Time-dependent SIR models. These are detailed as follows.
2.2.1 ML-based prevention techniques
Wang et al. [21] presented reinforcement learning for low dimensional vectors. It identified high-risk vertices gradually. A complex network of virus transmission is shown using IoT data for a weighted unidirectional-directional graph where mobile users as vertex, contact between users as edge, and being infected probability as vertex weight. The n-step Q-learning can handle the issue of the delayed score" (green bars), which quantifies the degree of risk from the perspective of the graph structure. In the final stage, reinforcement learning and the RAI algorithm are invoked for solving the MWVC by considering both the node score and weight. If the probability of contact is set to 0.8 proposed scheme then it reduces the 43% infection rate. The proposed method performs better than methods based on graph-theoretic. Traditional graph optimization performance degrades in dynamically time-varying environments but reinforcement learning performs well in continuously evolving graph structures.
Rustam et al. [22] developed future forecasting that is done by supervised ML models. This type of forecasting system can help effectively in making the decision to maintain the situation caused by the COVID-19 outbreak. For different class predictions performance of the ML algorithm changes. In the paper three predictions are done which are death rate future forecasting, new infected confirmed cases future forecasting, and recovery rate future forecasting. Four ML approaches or models are used which are LR (Linear Regression), SVM (Support Vector Machine), LASSO (LASSO Regression), and ES (Exponential Smoothing). The datasets were used from the GitHub repository (Number of new positive cases, deaths). For instance, like unknown inputs, a supervised learning model is built to predict. For the linear Regression model training, the input dataset is used as independent variable and class labels as a dependent variable. Using the regularization method to penalize extra features automatically LASSO model leads the regression model more effortless. SVM solves the problems of regression using a linear function and for non-linear regression, it uses mapping techniques as an input vector to feature space. ES methods are used for univariate data and also for earlier periods’ data forecasting. After processing COVID-19 datasets, datasets are divided into two sets. One is a training set that is trained using LR, SVM, LASSO, and ES models and another is a testing set. Then with the help of evaluation parameters like R-squared score, Adjusted R-squared, MAE, MSE, and RMSE the model is evaluated. Here 56 days are required to train and 10 days to test the model. ES model performs best for all forecasting and the SVM model performs worst in all cases. By increasing the days all models perform better.
Tuli et al. [23] presented that as COVID-19 is increasing rapidly, ML, and Cloud Computing can be helpful to control and observe the disease. This study includes a model for analyzing and predicting the state of the epidemic. Cloud computing is used to enhance the prediction process. Here the “Robust Weibull fitting” model is used. The model is based on an iterative weighting strategy. The model is deployed using the FogBus framework. The model can predict the date when the total number will reach 97% of expected cases. This model is better than Gaussian or Exponential models because COVID-19 data has many outliers and noise that makes it hard to predict perfectly. On the basis of comparison between the proposed and baseline Gaussian model, it is found that the Mean Square Error (MSE) and the Mean Absolute Percentage Error (MAPE) of the proposed model are lower than baseline for most cases.
Ardabili et al. [24] represented an analysis of ML and soft computing models that predict the outbreak of the disease. SEIR and SIR models are not used here because of the non-stationary mixing. Then another lack of conventional epidemiological models is when lead-time increases, model accuracy declines. That’s why this paper focuses on finding optimal performance of models based on equations like Logistic, Linear, Logarithmic, Quadratic, Cubic, Compound, Power, and exponential. Here are two ML models that MLP and ANFIS were used. To develop an accurate estimation model, constants were estimated. Among three ML optimizers GA, PSO, and GWO were considered, and GWO provided the highest accuracy within the smallest time. The best-fit prediction was achieved for the logistic model followed by the cubic model and quadratic model. The models MLP and ANFIS showed the capability of high generalization for long-term prediction while testing for up to 150 days.
Arora et al. [25] introduced a hybrid AI model based on embedding an NLP module and a long short-term memory (LSTM) network into an improved susceptible–infected (ISI) model to predict COVID-19. In the framework of the hybrid AI-based model, cured and deceased patients are not included in the epidemic model because they have no direct impact on the number of new confirmed cases. The infection rate deviation of the epidemic model is estimated using an LSTM network. The proposed ISI model is combined with the LSTM network to estimate the number of infected cases. Most of the previous research based on epidemic models follows a fixed number of days, for example, assuming the spreading of COVID-19 is exaggerated by k prior days. These models do not get into great detail on how epidemics spread. However, the suggested prediction algorithm can determine if new confirmed cases would infect newly confirmed patients on a given day. It is also possible to obtain the evolution laws of patients at various time intervals during the epidemic transmission process. The infection rate of patients in various places at various time intervals is researched, as well as whether current new confirmed cases are infected by the cumulative number of confirmed cases in the previous days. The infection rate and the time it takes for patients to become infected have a strong correlation. Multi-parameters are used to avoid drastic weight changes caused by a single data abnormality and it also reduces the complexity of the model. NLP technology is used with the LSTM network to get a more effective method by extracting semantic features from news reports related to preventing the COVID-19 epidemic.
Kavadi et al. [26] proposed partial derivative regression and a nonlinear ML method for prediction. The method finds the best parameter to evaluate the number of exposed, affected, cured, and dead people through Progressive Partial Derivative Linear Regression in the space of big data and perfectly predicts through Nonlinear Global Pandemic ML model normalization. The model overcomes the problem of correlation evaluation dependency on point estimates of limit variables. The system goes on the basis of building mathematical design then applying progressive hypothesis using normalized features and finally predicting the outbreak based on Kuhn-Tucker conditions. The prediction time of the model is smaller than linear regression-based prediction. Better accuracy is found using NGP- MLP. (Normalized Graded Pace-multilayer perceptron) with the PDR-NML method.
2.2.2 Time-dependent SIR model
Waqas et al. [27] used the time-dependent Susceptible-Infected-Recovered (SIR) model for prediction. The model depends on two impartment tunable parameters. ML approach is also used but it doesn’t give superior results. The total number of population is measured as the summation of Susceptible, Infective, and remove persons. The model assumes that the recovered person will not be infected again and they are removed. The obstacle to the estimation of parameters is that variables have to be monotonically decreasing and increasing functions with time. Another obstacle is that if the parameter decreases quickly, the model underestimates epidemic transmissibility. The model works better when it is fitted using different subsets of data. The analysis is first done over the pandemic peak and cumulative Infective of Switzerland and European countries and gets validation. Then the analysis is done over Pakistan.
2.3 AI system-based COVID-19 cure techniques
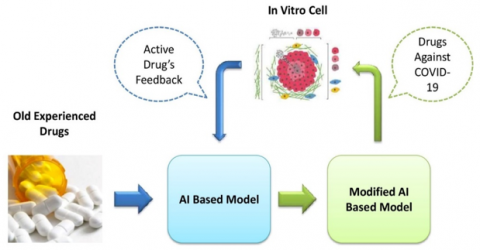
AI not only helped medical science by providing information about the dreadfulness of the COVID-19 outbreak but also helped to analyze different medicines to find out the cure for coronavirus (Figure 4). Though the medicines are not invented yet, bigger progress in the pathway of doing so is made by the contribution of AI. It helped the pharmacist to experiment on drugs without facing major backlashes. The cure techniques are divided into two categories: i) Drug Repurposing, and ii) Disease Progression Observation in Mild Cases.
2.3.1 Drug repurposing
Ke et al. [28] presented that in this pandemic situation there is a need for a cure that can be identified quickly and that has previous experience. For that purpose, AI technology can be used. This technology can identify old drugs against COVID-19. In this study, the predicted drugs using an AI-based system based on Deep Neural Network (DNN) are tested against feline coronavirus in vitro. AI system performs screening for old drugs by generating a relevant prediction model. The learning datasets are divided. One has proven active against SARS-CoV and another 3C-like protease inhibitors. Here two AI models are used. For antiviral activity verification, AI-identified drugs are evaluated. The identified drugs are verified against feline coronavirus in vitro. That’s why it requires relearning and generating a modified model. Here ECFP, FCFPs, and ALogP_count molecular descriptors are used. AI model 1 is based on a learning dataset containing drugs for influenza, SARS-CoV, HIV, and AI model 2 is based on a learning dataset of 210 inhibitors of 3C-like protease of SARS-CoV. Among 80 identified drugs only 8 drugs showed activity in vitro and the other five additional drugs are found also. 13 drugs are found that have a high potential for future development use for COVID-19 treatment.
2.3.2 Disease progression observation in mild cases
Huang et al. [29] represented the prediction of progression in mild cases as the major number of patients of COVID-19 are with mild syndromes. Here also the risk factor of oxygen requirement is explored using multivariate logistic regression. Two models were developed. One for patients for self-isolation and another for doctors for making an early decision. To compare distributed and normally distributed variables t-test is used. Based on distribution, continuous variables are expressed as medians with interquartile ranges. For diagnostic accuracy, an area under the receiver operator characteristic curve (AUROC) is used. It is found that the disease progression rate is high in older and more likely to be males and also has symptoms long period of time. The two nomograms based on laboratory data are not included in multivariate analysis were shorter than laboratory data included in multivariate analysis. As mild COVID-19 patients have no availability of blood tests, the application of model-based laboratory data gets limited. These two models are useful for the possibility of further medical intervention as the NPV was 96% for both models.
Table 1. Summary of COVID-19 detection-based research
|
Author Name |
Input |
Method & Model |
Performance |
Advantage |
Limitations |
Resources |
|
Barstugan et al. [1] |
CT image of the chest |
Extraction models: Grey Level Co-occurrence Matrix, Local Directional Pattern, Grey Level Run Length Matrix, Grey Level Size Zone Matrix, Discrete Wavelet Transform and classified by the SVM (Support vector machines) |
87.6% accuracy till now, Grey Level Size Zone Matrix method gave the best classification accuracy of 99.68% with 10-fold cross-validation. |
Detects COVID-19 faster |
Data set that the model is tested on isn’t sufficient in numbers |
SVM |
|
Özkaya et al. [2]
|
CT image of the chest |
A pre-trained CNN, SVM |
96.54% on Matthews Correlation Coefficient (MCC) metrics and 98.28% F1-score with 98.27% accuracy |
Detects faster and shows accurate classification for COVID-19 |
The classification performance is limited and there’s scope to do better with data augmentation |
|
|
Pokhrel et al. [3] |
RT-PCR test, Immunoassay test and CT image test results |
RT-PCR |
CT images results are 98% more sensitive than the RT-PCR method. It also identified that the Immunoassay test results shows 100% specificity in case of COVID-19 patients |
|
|
|
|
Mangal et al. [4] |
X-ray reports of chest |
Deep neural network based AI detector named CovidAID |
Accuracy: 90.5%, F1 score: 0.9178-0.9282 (95% CI) |
Better and faster detection |
Worked with publicly maintained tool only which is not enough. Further better accuracy can be gained if experimented for clinical tests. |
CovidAID |
|
Alqudah et al. [5] |
X-ray reports of chest |
Hybrid model consisting support vector machine (SVM), random forest (RF), and many more |
95.2% accuracy |
Faster detection of COVID-19 |
|
|
|
Majeed et al. [6] |
X-ray reports of chest |
CNN-X architecture consisting of 12 off-the-shelf CNN models |
Accuracy: 97.82 |
Faster detection and classification |
Only rely on X-ray report which may not give the best result |
CNN-X |
|
Sahinbas and Catak [7] |
X-ray reports of chest |
pre-trained CNN architectures: VGG16, VGG19, ResNet, DenseNet, and InceptionV3 |
VGG16 model shows higher accuracy of 80% |
can provide more accurate performance if the number of instances in the dataset increases |
|
|
|
Ozturk et al. [8] |
Chest X-ray image of COVID, normal and Pneumonia |
deep neural networks |
generates 98.08% accuracy for binary classes and 87.02% for multi-class cases. For multi-class classification Sensitivity 85.35% and specificity 92.18% For binary classification Sensitivity 95.13% and specificity 95.30% F1 score for multi-class 87.37% and for binary 96.51% classification |
avoids feature extraction method to classify |
limitation of data |
|
|
Mahmud et al. [9] |
Chest X-ray image of COVID, normal and Pneumonia |
Deep convolutional neural network |
to get more optimization stacking algorithm is used. accuracy of 97.4% for COVID/Normal, 96.9% for COVID/Viral pneumonia, 94.7% for COVID/Bacterial Pneumonia and 90.2% for multiclass COVID/normal/Viral/Bacterial pneumonia. F1 score 97.1% for COVID/Normal, 87.8% for COVID/Viral pneumonia and 93.9% for COVID/Bacterial Pneumonia based on Performance comparison of proposed method with other traditional networks on COVID-19 and other pneumonia detection |
Depth wise convolution helps to analyze X-rays in different perspectives |
Combination of clinical data and radiographic findings can improve performance |
|
|
Khan et al. [10] |
Radiography image of COVID, normal and Pneumonia |
a deep convolution neural network based on exception architecture |
accuracy improves to 90% by combining pneumonia-bacterial and pneumonia-viral into one single class and fine tuning all classes. F1 score 89.8%. overall accuracy of 89.6% and for COVID-19 cases are 93%, specificity of 96.4% |
Less expensive and gives promising result |
More training data can improve the model |
|
|
Rajaraman et al. [11] |
Chest X-ray image of COVID, normal and Pneumonia |
Iteratively Pruned Deep Learning and pretrained ImageNet models |
Parameters are reduced 46.03% for VGG16 model and 16.13% for VGG19 model compared to unpruned weighted pruned method performs better. Overall accuracy of 99.01% and area under the curve of 0.9972 in detecting COVID-19. Average F1 score is 0.9901 for weighted pruned method |
reduces complexity and increases efficiency of memory because of pruning |
No visualization and interpretation of the pruned model and application to COVID-19 detection |
|
|
Rahimzadeh and Attar [12]
|
Chest X-ray image of COVID, normal and Pneumonia |
modified deep convolutional neural network based on the concatenation of Xception and ResNet50V2 |
Almost same number of class shows better result of detection of COVIV-19. average accuracy of 99.50% for proposed network and overall average of 91.4%. average specificity 99.33 for ResNet50V2 and 99.56% for Concatenated |
Multiple feature extraction gets best result |
Network can be increased by using larger dataset |
|
|
He et al. [13] |
CT image and X-ray report of the chest of patient |
two types of state-of-the-art (SOTA) Deep Learning models: 3D CNN including DenseNet3D121, R2Plus1D, MC3 18, ResNeXt3D101, PreAct ResNet, and ResNet3D series and 2D CNNs, including DenseNet121, DenseNet201, ResNet50, ResNet101 and ResNeXt101 |
|
|
|
CNN software |
|
Salih et al. [14] |
CT images and X-ray images of the chest of COVID-19 patients |
modified AlexNet model |
accuracy of 96% and 97.27% for X-ray and CT scans respectively |
Better detection than existing Alexnet model |
|
MATAB software |
|
Alom et al. [15] |
CT image and X-ray report of the chest of patient |
Multi-Task Deep Learning, NABLA-N based segmentation model, IRRCNN based detection model |
84.67% and 98.78% accuracy for X-ray and CT images respectively |
Detects faster and shows accurate classification for COVID-19 |
COVID-Det_CT model is trained and examined with 300 cases only which is not a sufficient number to show results |
CNN softwares, COVID-Det_CT |
|
Öztürk et al. [16] |
CT image and X-ray report of the chest of patient |
Feature extraction: Grey Level Co-occurrence Matrix (GLCM), Local Binary Grey Level Co-occurrence Matrix (LBGLCM), Grey Level Run Length Matrix (GLRLM), and Segmentation-based Fractal Texture Analysis (SFTA) and classification: SVM |
90% accuracy overall |
Detects COVID-19 faster
|
Because of working on only 260 images in total the model seems to face an overfitting problem |
SVM and CNN softwares |
|
Hashmi et al. [17] |
Previous disease dataset |
Pearson correlation and Spearman Correlation coefficient |
Fever in 43.9% (P = 0.000) cases, cough 54.08% and dry mucus 25.68% equally significant (P = 0.000), Hyperemic pharyngeal mucus membrane 17.92% (P = 0.005), leukopenia 28.11% (P = 0.000) lymphopenia 64.35% (P = 0.000), thrombopenia 35.49% (P = 0.000), elevated Alanine aminotransferase 50.02% (P = 0.000), and Aspartate aminotransferase 34.49% (P = 0.000) |
Early assessment helps patient to take precautions and treatment from the early stage |
|
|
|
Roland et al. [18]
|
symptoms, demographic information, comorbidities and COVID-19 test results |
predictive model selected through logistic regression and classifiers were implemented using receiver operating characteristic analysis (ROC) |
Unreasonable body aches shows the highest sensitivity of 80% and the reduction of smell and taste sensing shows the specificity of 73% |
Early detection of COVID-19 through prediction |
|
|
|
Escobar et al. [19] |
sociodemographic data of the previous cases |
Machine learning based pooling method |
shows 42% accuracy gaining in case of testing a patient for COVID-19 |
|
|
|
|
Mohammed et al. [20] |
Thermal image |
IOT based system integrated with GPS and camera |
Can detect all people in short time |
Early detection. Reduces human error |
Cannot exactly identify a corona patient |
Arduino IDE and Helmet, thermal camera, optical camera are used |
Table 2. Summary of COVID-19 prevention and cure research
|
Authors |
Input |
Method & Model |
Performance |
Advantage |
Limitations |
Resources |
|
Wang et al. [21] |
users as vertex, contact between users as edge and being infected probability as vertex weight for graph. |
Joint Graph Theory with SIoT and Reinforcement Learning |
For 0.8 contact probability infection reduces 43% Beneficially reduces infection |
better than methods based on graphtheoretic and performs well in continuously envolving graph structures |
More data have to use to verify more accuracy |
|
|
Rustam et al. [22] |
Number of new positive cases, deaths and recoveries from GitHub repository |
supervised machine learning (LR, SVM, LASSO, ES) |
ES model performs best and SVM model performs worst all cases ES model gives best accuracy |
Focuses on live and early forecasting of COVID-19 confirmed case and outbreak |
Models perform better with increasing day MSE for death rate are 840240.11(LR),3244066.79(LASSO),16016210.98(SVM),662228.72(ES) MSE for new infected confirm case are 1472986504.96(LR),234489560.99(LASSO),5760890969.30(SVM),283201302.2(ES) |
|
|
Tuli et al. [23] |
Data of confirmed cases of COVID19 |
Robust Weibull Fitting model |
MAPE 12% lower than non-iteratively weighted Weibull |
Real time prediction because of cloud computing |
Biases in data. For World. MSE is 2.41E+07 and. MAPE is 49.14 |
64-bit Microsoft Windows Server 2016 and Single core Azure B!s virtual machines with 1 GiB RAM,SSD storage are used |
|
Ardabili et al. [24] |
Data of cases of COVID19 Based on 5 countries |
machine learning and soft computing based MLP and ANFIS |
High generalization for long-term prediction while testing for up to 150 days logistic model and GWO shows highest accuracy among GA, PSO, GWO |
Avoids accuracy declines due to lead-time increasing |
Models were trained using dataset based on only Italy, China, Iran, Germany and USA. RMSE are 196.83, 2270.57, 397.47, 55.56, 22.33 for Italy, China, Iran, Germany and USA respectively |
|
|
Arora et al. [25] |
32 individual time-series data of confirmed COVID-19 cases |
recurrent neural network (RNN) and long short-term memory (LSTM) |
bi-directional LSTM performs best. bi-directional LSTM gives accuracy of error less than 3% for daily predictions and less than 8% for weekly predictions |
It gives state-wise prediction |
Dataset only based on India. Average MAPE 4.81% for stacked LSTM, 3.22% for bi-directional LSTM and 5.05% for conv-LSTM |
|
|
Kavadi et al. [26] |
Number of exposed, affected, cured and dead people |
partial derivative regression and nonlinear machine learning |
Prediction time is smaller than linear regression based prediction. PDR-NML gives 2% and 3% better accuracy than linear regression and AI-based method |
overcomes the problem of correlation evaluation dependency on point estimates of limit variables |
Dataset is based on only India |
|
|
Waqas et al. [27] |
Data of infeted, recoverd and susceptible cases |
Time-dependent Susceptible-Infected-Recovered (SIR) Model |
Decreasing of parameter happens to underestimation of epidemic transmissibility |
ML approach don’t give superior result than this model |
if parameter decreases quickly, model underestimates epidemic transmissibility |
|
|
Ke et al. [28] |
Old and experienced drugs |
Deep Neural Network (DNN) |
Among 80 identified drugs 8 showed and other 5 additional drugs were found. 13 drugs were found that had high potential to future development |
Gives efficient drugs within short of time |
Feedback delay |
|
|
Huang et al. [29] |
extracted data from electronic medical records |
nomogram based logistic regression model |
NPV was found 96%. Sensitivity, 80% |
Disease progression can be observed |
With small sample size internalexternal validation was not performed |
|
This review paper is about the detection, prevention, and cure of the COVID-19 pandemic through different mathematical models and Artificial Intelligence. A lot of initiatives are taken in the major fields such as IoT, AI, CNN, and ML to prevent this pandemic. In recent few months, an unthinkable number of researches have been performed against COVID-19. Though their procedures are not the same, each of the proposed works has a common goal which is to resist COVID-19. The papers [1-16] represent the ML-based COVID-19 detection method. By extracting features from images, faster models are developed to detect the COVID-19 effect on human organs. This portion uses chest CT-Scan images, chest X-ray images, and other detecting features. The early COVID-19 detection method is adapted in papers [17-19]. The IoT-based method [20] detects temperature, appearance, and other external symptoms through different hardware tools like helmets, mobile phones, etc. The papers [21-27] are dedicated to finding the processes for preventing COVID-19 spread by using the ML model, Time-dependent SIR Model, LSTM network, NLP module, ISI, Partial derivative regression, and nonlinear machine, etc. The cure processes use AI-based techniques [28, 29] to find out reusable drugs and other medications for COVID-19 infection. The summary of COVID-19 Detection-based Research is shown in Table 1, and the summary of COVID-19 prevention and cure-based Research is shown in Table 2.
The methods have the scope for improvement by using enough datasets [1, 8, 10, 12, 15, 16, 21]. The method [4] may improve its performance by using the clinical dataset rather than using the public dataset only. A combination of clinical data and radiographic findings may improve performance in the paper [9]. There is a scope of working on visualization and interpretation of the pruned model and application to COVID-19 detection as an enhancement [11]. These modifications will help the researchers to reach a new dimension.
This paper represents the recent works of different fields like CNN, AI, IoT, Data analysis, etc. against COVID-19. The main purpose of all of these works is either to detect, prevent or find a cure for COVID-19. Real-time data was taken to measure the output. Different tools and methods are introduced, which are capable of handling the situation by their own mechanism. Though there is a limitation, further modification can bring the systems into a new dimension of research. During this COVID-19 pandemic, the reviewed works, done in this paper, will be effective for the researchers who are enthusiastic about developing a system to control the effect of COVID-19.
[1] Barstugan, M., Ozkaya, U., Ozturk, S. (2020). Coronavirus (COVID-19) classification using CT images by machine learning methods. arXiv preprint arXiv:2003.09424, https://doi.org/10.1101/2020.04.03.20048868
[2] Özkaya, U., Öztürk, Ş., Barstugan, M. (2020). Coronavirus (COVID-19) classification using deep features fusion and ranking technique. In: Hassanien, AE., Dey, N., Elghamrawy, S. (eds) Big Data Analytics and Artificial Intelligence Against COVID-19: Innovation Vision and Approach. Studies in Big Data, vol 78. Springer, Cham. https://doi.org/10.1007/978-3-030-55258-9_17
[3] Pokhrel, P., Hu, C., Mao, H. (2020). Detecting the coronavirus (COVID-19). ACS sensors, 5(8): 2283-2296. https://doi.org/10.1021/acssensors.0c01153
[4] Mangal, A., Kalia, S., Rajgopal, H., Rangarajan, K., Namboodiri, V., Banerjee, S., Arora, C. (2020). CovidAID: COVID-19 detection using chest X-ray. arXiv preprint arXiv: 2004.09803. https://doi.org/10.48550/arXiv.2004.09803
[5] Alqudah, A.M., Qazan, S., Alquran, H., Qasmieh, I.A., Alqudah, A. (2020). COVID-19 detection from X-ray images using different artificial intelligence hybrid models. Jordan Journal of Electrical Engineering, 6(2): 168-178. https://doi.org/10.5455/jjee.204-1585312246
[6] Majeed, T., Rashid, R., Ali, D., Asaad, A. (2020). COVID-19 detection using CNN transfer learning from x-ray images. Medrxiv. https://doi.org/10.1101/2020.05.12.20098954
[7] Sahinbas, K., Catak, F.O. (2021). 24 - Transfer learning-based convolutional neural network for COVID-19 detection with X-ray images. Data Science for COVID-19, pp. 451-466. https://doi.org/10.1016/b978-0-12-824536-1.00003-4
[8] Ozturk, T., Talo, M., Yildirim, E.A., Baloglu, U.B., Yildirim, O., Acharya, U.R. (2020). Automated detection of COVID-19 cases using deep neural networks with X-ray images. Computers in Biology and Medicine, 121: 103792. https://doi.org/10.1016/j.compbiomed.2020.103792
[9] Mahmud, T., Rahman, M.A., Fattah, S.A. (2020). CovXNet: A multi-dilation convolutional neural network for automatic COVID-19 and other pneumonia detection from chest X-ray images with transferable multi-receptive feature optimization. Computers in Biology and Medicine, 122: 103869. https://doi.org/10.1016/j.compbiomed.2020.103869
[10] Khan, A.I., Shah, J.L., Bhat, M.M. (2020). CoroNet: A deep neural network for detection and diagnosis of COVID-19 from chest x-ray images. Computer Methods and Programs in Biomedicine, 196: 105581. https://doi.org/10.1016/j.cmpb.2020.105581
[11] Rajaraman, S., Siegelman, J., Alderson, P.O., Folio, L.S., Folio, L.R., Antani, S.K. (2020). Iteratively pruned deep learning ensembles for COVID-19 detection in chest X-rays. IEEE Access, 8: 115041-115050. https://doi.org/10.1109/access.2020.3003810
[12] Rahimzadeh, M., Attar, A. (2020). A modified deep convolutional neural network for detecting COVID-19 and pneumonia from chest X-ray images based on the concatenation of Xception and ResNet50V2. Informatics in Medicine Unlocked, 19: 100360. https://doi.org/10.1016/j.imu.2020.100360
[13] He, X., Wang, S., Shi, S., Chu, X., Tang, J., Liu, X., Yan, C., Zhang, J., Ding, G. (2020). Benchmarking deep learning models and automated model design for COVID-19 detection with chest CT scans. MedRxiv. https://doi.org/10.1101/2020.06.08.20125963
[14] Salih, S.Q., Abdulla, H.K., Ahmed, Z.S., Surameery, N.M.S., Rashid, R.D. (2020). Modified alexnet convolution neural network for COVID-19 detection using chest X-ray images. Kurdistan Journal of Applied Research, 5(3): 119-130. https://doi.org/10.24017/covid.14
[15] Alom, M.Z., Rahman, M.M., Nasrin, M.S., Taha, T.M., Asari, V.K. (2020). COVID_MTNet: COVID-19 detection with multi-task deep learning approaches. 2020, arXiv:2004.03747. https://doi.org/10.48550/arXiv.2004.03747
[16] Öztürk, Ş., Özkaya, U., Barstuğan, M. (2021). Classification of coronavirus (COVID‐19) from X‐ray and CT images using shrunken features. International Journal of Imaging Systems and Technology, 31(1): 5-15. https://doi.org/10.1101/2020.04.03.20048868
[17] Hashmi, H.A.S., Asif, H.M. (2020). Early detection and assessment of COVID-19. Frontiers in Medicine, 7: 311. https://doi.org/10.3389/fmed.2020.00311
[18] Roland, L.T., Gurrola, J.G., Loftus, P.A., Cheung, S.W., Chang, J.L. (2020). Smell and taste symptom‐based predictive model for COVID‐19 diagnosis. International Forum of Allergy & Rhinology, 10(7): 832-838. https://doi.org/10.1002/alr.22602
[19] Escobar, M., Jeanneret, G., Bravo-Sanchéz, L., Castillo, A., Gomez, C., Valderrama, D., Roa, M., Martinez, J., Madrid-Wolff, J., Cepeda, M.L., Guevara-Suarez, M., Sarmiento, O.L., Medaglia, A., Forero-Shelton, M., Velasco, M., Pedraza-Leal, J.M., Restrepo, S., Arbeláez, P. (2020). Smart pooling: AI-powered COVID-19 testing. medRxiv, https://doi.org/10.1101/2020.07.13.20152983
[20] Mohammed, M.N., Syamsudin, H., Al-Zubaidi, S., Karim, S.A., Ramli, R., Yusuf, E. (2020). Novel COVID-19 detection and diagnosis system using IOT-based smart helmet. International Journal of Psychosocial Rehabilitation, 24(7): 2296-2303. https://doi.org/10.37200/IJPR/V24I7/PR270221
[21] Wang, B., Sun, Y., Duong, T.Q., Nguyen, L.D., Hanzo, L. (2020). Risk-aware identification of highly suspected COVID-19 cases in social IoT: A joint graph theory and reinforcement learning approach. IEEE Access, 8: 115655-115661. https://doi.org/10.1109/access.2020.3003750
[22] Rustam, F., Reshi, A.A., Mehmood, A., Ullah, S., On, B.W., Aslam, W., Choi, G.S. (2020). COVID-19 future forecasting using supervised machine learning models. IEEE Access, 8: 101489-101499. https://doi.org/10.1109/access.2020.2997311
[23] Tuli, S., Tuli, S., Tuli, R., Gill, S.S. (2020). Predicting the growth and trend of COVID-19 pandemic using machine learning and cloud computing. Internet of Things, 11: 100222. https://doi.org/10.1016/j.iot.2020.100222
[24] Ardabili, S., Mosavi, A.H., Ghamisi, P., Ferdinand, F., Várkonyi-Kóczy, A.R., Reuter, U., Rabczuk, T., Atkinson, P.M. (2020). COVID-19 outbreak prediction with machine learning. Algorithms, 13(10): 249. https://doi.org/10.1101/2020.04.17.20070094
[25] Arora, P., Kumar, H., Panigrahi, B.K. (2020). Prediction and analysis of COVID-19 positive cases using deep learning models: A descriptive case study of India. Chaos, Solitons & Fractals, 139: 110017. https://doi.org/10.1016/j.chaos.2020.110017
[26] Kavadi, D.P., Patan, R., Ramachandran, M., Gandomi, A.H. (2020). Partial derivative nonlinear global pandemic machine learning prediction of COVID 19. Chaos, Solitons & Fractals, 139: 110056. https://doi.org/10.1016/j.chaos.2020.110056
[27] Waqas, M., Farooq, M., Ahmad, R., Ahmad, A. (2020). Analysis and prediction of COVID-19 pandemic in Pakistan using time-dependent SIR model. 2020, arXiv:2005.02353. https://doi.org/10.48550/arXiv.2005.02353
[28] Ke, Y., Peng, T., Yeh, T.K., Huang, W., Chang, S., Wu, S., Hung, H., Hsu, T.A., Lee, S., Song, J., Lin, W., Chiang, T., Lin, J.H., Sytwu, H., Chen, C.T. (2020). Artificial intelligence approach fighting COVID-19 with repurposing drugs. Biomedical Journal, 43(4): 355-362. https://doi.org/10.1016/j.bj.2020.05.001
[29] Huang, J., Cheng, A., Lin, S., Zhu, Y., Chen, G. (2020). Individualized prediction nomograms for disease progression in mild COVID‐19. Journal of Medical Virology, 92(10): 2074-2080. https://doi.org/10.1002/jmv.25969