Julie Golliot* | Laurent Maury
OPEN ACCESS
Preserving the autonomy of elderlies or of people affected by a neuro-evolutionary disease such as Alzheimer's, and relieving the mental burden on their caregivers, is an ethical, economic, and social challenge for society. To address this issue, an interdisciplinary consortium involving medical experts, researchers and end-users has been created to co-design and develop a socio-technical construct named Mementop. The solution aimed at the entire ecosystem of the care receiver - i.e., his caregivers and health professionals -, bringing together in a unified user experience the features required by these parties while allowing the care receiver to remain actor in his daily life. Mementop is a certified medical device based on a smartphone application shared by all the contributors of this senior-centred ecosystem, a multi-sensory and customisable printed press product as well as a set of digital inclusion aids. The first version is available since early 2022 and research is conducted to improve its acceptability. Other ongoing research deal with advanced AI techniques to create an intelligent companion based on a predictive model of the evolution of the loss of autonomy.
euro-evolutionary diseases, autonomy, mental load, stimulation, social link, self
According to the WHO, by 2030, more than one billion people in the world will be aged 65 and over. The Ministry of Solidarity and Health states that in 2021, France had 2.5 million elderly people suffering from loss of autonomy, a figure that is likely to rise to 3 million by 2030, when the over-60s will represent 21 million people, compared to 18.5 million today. 1.4 million French people are affected by a neuro-evolutionary disease (ND) such as Parkinson's disease, Alzheimer's disease and related diseases. Every year, 250,000 new cases of Alzheimer's disease are diagnosed. According to France Alzheimer association, 51% of sufferers live at home and a further 30% live with a caregiver. Thus, less than 25% of sufferers are hospitalized or accommodated in a specialized environment, such as an EHPAD. No curative medical treatment has proven to be clinically effective. The available drug treatments are putting considerable pressure on health systems; in France, they have been delisted from the reimbursement list in 2019.
Although the aetiologies differ, the different ND have some symptoms in common. In particular, amnesia takes three forms. Firstly, episodic memory disorders concern past events and often appear first. The subject forgets what he or she did recently, what he or she ate for lunch or what he planned to do in the afternoon. Working memory problems are the second most common symptom of early onset. Patients have difficulty remembering a telephone number long enough to write it down, memorizing directions to find their way or doing mental calculations. Finally, semantic memory disorders usually appear at a later stage of the disease. This concerns the automatic gestures used, for example, to open a door, put on a pull-over or eat correctly. There are other symptoms to consider. These include progressive aphasia, which affects word knowledge, syntax and speech, and thus impairs communication. Apraxia, or motor difficulties, causes clumsiness of movement, forgetting how to handle an object or loss of sensation. The gestures of daily life are considerably more complex to achieve. Agnosia takes the form of mental confusion causing non-recognition of faces or objects, leading to indifferent, mute or aggressive postures.
The psychological and emotional constraints and difficulties experienced by the people concerned stem from these cognitive and memory problems: (1) A significant and progressive reduction in self-esteem (shame, embarrassment, self-deprecation); (2) A feeling of loss of control, of being left behind and of discomfort (I can no longer do anything on my own, I feel overwhelmed); (3) A feeling of dependence (at least in the early stages of the disease) on other people, especially the care receiver's family and friends.
According to the French National Authority for Health, more than 80% of people with ND in France suffer from loneliness or isolation, while 75% of them express the wish to remain at home if possible. The expectations commonly expressed by the subjects concerned can be factorised. These are the wish to remain at home as long as possible; the wish to remain independent as long as possible and not to be totally dependent on family caregivers, although daily help may be necessary; the wish not to harm family caregivers, especially family members and close friends; and the wish to occupy free time. Memory and cognitive issues associated with ND have a strong impact on the daily life of patients and affect their autonomy. Relatives and caregivers frequently report a feeling of exhaustion. The systemic family upheaval now leads us to focus on the care receiver/caregiver tandem and not only on the care receiver himself.
The successful development of initiatives described as digital - i.e., relying on software and/or hardware devices - and the conduct of numerous research projects highlight the interest in using digital tools to compensate for loss of autonomy, through sensory transposition devices, for people suffering from a disability or characterized by diminished autonomy [1]. The search for solutions adapted to problems related to the compensation of disability or loss of autonomy mobilizes several dozen laboratories in France. Great progress has been made in recent years in nanoelectronics and in the field of deep learning, particularly about mathematical algorithms for increasing the learning speed of neural networks. Although older users may experience difficulties, fear, or rejection regarding the use of digital technologies, a high added value of use and a perfect consistency of experience between each function contribute to their acceptation and adoption [2, 3]. In 2021, 78% of 60-69-year-olds and 59% of 70 years old own and use a smartphone.
Acting on the preservation of autonomy or delaying the onset of a situation of dependence requires working on six axes: preservation of health; preservation of memory; security and safety; preservation of self-esteem; preservation of social ties with loved ones; maintenance of the implementation of projects. As medical treatments don't seem to be a suitable solution soon, other avenues need to be explored, by using digital devices capable of involving care receiver, their family, and friends and, when appropriate, healthcare staff. The aim of the Mementop research program is to create an innovative digital solution, based on IA, to: (1) The care receiver to remain autonomous, active, safe, in contact with his or her loved ones and at home for as long as possible, as well as to preserve or even strengthen the social link within the dyad (caregiver - care receiver one); (2) Support caregivers and reduce the mental burden on them; (3) Inform health professionals to improve the effectiveness of their management and supportive care.
To address this interdisciplinary issue, a consortium was constituted. It involved two internal researchers from the company carrying out the project, a scientific committee composed of two geriatricians, two neurologists, a mathematician, and an expert in HMI, six multidisciplinary laboratories (Data Science, Computer Science, Neuropsychology, Information and Communication Sciences, Design) as well as potential users (associations, families, care receivers).
The Scientific Committee took part in the indispensable ideation effort that characterizes any research project. This privileged space for sharing the know-how and expertise of each contributor has enabled them to contribute to the search for specific solutions, depending on the progress of the work. The validation and improvement of the solutions envisaged, particularly in terms of the creation of devices to stimulate the cognitive and memory faculties of care receivers, also took place in this framework. The committee also contributed to the definition of a study methodology and the testing of certain working hypotheses, thanks to the voluntary and deliberate contribution of certain care receivers. Finally, it facilitated and supervised the conduct, follow-up, and interpretation of these tests.
The inclusion of users in the design of such a solution was essential, particularly in the identification of issues relating to the ergonomics of the solutions envisaged, as in the choice of control modes for digital devices. Such research methods, including users in an interdisciplinary design process would help to match the innovator's perceptions and desires for improvement with those of the targeted users. They would guarantee an innovation that would be at their service (and by rebound, at the service of all) [4].
Conducted since 2017, the research has been carried out in two phases: The first consisting of observations and preliminary studies and leading to a theoretical design; the second, iterative, taking the form of an initial design and then an arbitrary number of intermediate designs.
2.1 Phase 1
2.1.1 Observations and preliminary studies
State of the art: A corpus of texts and reference documents was established, with data being collected on various knowledge sharing and dissemination platforms, including CAIRN, ERUDIT, PERSEE, WORDCAT, the SUDOC catalogue and the ISIDORE platform. These data were classified and structured in thematic trees and shared with the consortium to be discussed in plenary sessions or in groups according to the topics addressed. If is a lot of research in this field exist, a very few aims to create a commercialized solution made available to the care receivers or their relatives. We found no solution designed with a solid scientific approach or scientifically validated. Furthermore, none of the solutions is aimed both at the care receivers and at his caregivers, offers an extended functional scope nor proposes an intelligent companion calculating clinical health indicators to personalize his behavior (social isolation, undernutrition, etc.). Finally, during the initial phase of the research, the importance of thinking about human-machine interaction (HMI) and interface ergonomics for an elderly population was analyzed at length.
Identification of the needs and expectations of the vulnerable person: Between 2017 and 2018, the expectations of people affected by a ND were mapped according to the stage of their disease. In stage 1, care receivers are inclined to "refuse to be dominated by the disease, to remain active" and turn to cognitive and memory stimulation devices. In stage 2, they frequently look for some technical helping solutions, without involving a third party (human), to avoid forgetting tasks or actions. They also look for some exosomatic storage solutions, to put in a safety place some information they are likely to forget and that helps them maintain their autonomy (codes, passwords, recipes, instructions for using household appliances, etc.). At stages 3, 4 and 5, representing the main target of this research, an extensive personae analysis was carried out and reveals similar, albeit varying, expectations, with a pronounced appetite for digital technologies and more or less strong support from family caregivers. Finally, beyond stage 5, the risks of aphasia and/or apraxia constitute serious obstacles to the use of a digital device. The proposed functions therefore mainly affect family caregivers, helping to simplify their daily tasks while improving the effectiveness of their individual and collective contributions.
Identification of the needs and expectations of the stakeholders involved in supporting the frail person: In France, nearly 3.5 million people are caregivers to at least one sick or dependent person. On average, each caregiver spends 6.5 hours a day with the people they care for. Stress, a feeling of loneliness and a sense of powerlessness are recurrently described by the family caregivers of people with an ND. Two focus group were conducted with four groups of caregivers. Their expectations were divided into five areas: Reassurance and stress management; locating the relative; communication with the relative; providing assistance to the relative; possibility of setting up a collective organization.
Identification of processes and mapping of existing interactions: A mapping of inter-relationships between the different actors of the patient’s tribe has been established. We can mention the reflexive relationship (1) of the care receiver and his or her relationship to the self, reflecting in part his or her well-being, feeling, self-confidence and the active notion of awareness of being. It also encompasses the possibilities of therapeutic actions on the abilities of the care receiver. The relationship (2) between the care receiver and the caregiver is at the heart of societal concerns about the caregiver's situation. It contributes to the essential maintenance of social links. Culturally dominant, it provokes a simplistic assimilation of the caregiver's word to that of the cared-for. The relationship (3) with the health professional comprises three processes. The first is societal, with an expectation of the professional to whom a certain comfort of life is entrusted. The second is psychological, resulting from family relationships. The last is socio-professional, with the caregiver's training not always sufficient and subject to clumsiness and misunderstandings.
2.1.2 Theoretical design
(1) Assumptions and definition of data collection and interpretation protocols: Sociographic and anthropological data collected during the experiments make it possible to envisage new hypotheses and to revise theoretical models in terms of support for frail people. Putting these data and technological potential into perspective also allows for the development of tools and services relatively easy to integrate into the user's environment. Compliance with the RGPD by all the components and processes implemented is also a primary obligation and a priority [5]. Hosting of "Health Data Hosting" (HADS) is imperative.
(2) Theoretical modelling: Seven use cases were identified for the design of a scalable and adaptable digital platform, centered on both the care receiver and his caregivers. The identification of the initial functional perimeter has enabled us to put forward hypotheses for technological solutions to be tested. Accessibility is of course a determining element to obtain the highest possible level of adoption. It must be considered as a key concern when evaluating a smartphone application [6]. Standards and research in the context of Alzheimer's disease and the WCAG recommendations allow for an evaluation of the accessibility parameters of the functionality of an application for a clearly defined user group. Accessibility was assessed as soon as possible. Usability was then studied through a set of usability heuristics comprising five main components [7]: Learnability; memorability; effectiveness; errors; satisfaction. These evaluations were carried out in close partnership with associations, families, and frail people, particularly suffering from Alzheimer's disease.
(3) Experiments and analysis: Several hypotheses were tested with the help of our Scientific Committee as well as with care receivers and their family caregivers. The analysis of the results made it possible to adjust both the functional scope and the envisaged HMIs.
2.2 Phase 2
A series of iterations took place, each following the same logic and resulting in an enriched version of the device. First, the working assumptions and the definition of the data collection and interpretation protocols were made. This allowed the specification and modelling of new functionalities or the necessary adjustments to existing functionalities. A prototype was then built, tested internally, submitted to the Scientific Committee, and then tested with care receivers and their family caregivers. The results were analysed and when they were satisfactory the final implementation was made so that the enhanced version could be made available to users.
This research has given rise to a CE-certified medical device named Mementop, which focuses on the ecosystem (triplet) formed by a care receiver, his caregivers and the health professionals involved in his care or follow-up [8].
Mementop is a socio-technical construct that has three components: (1) A smartphone application, focused on the care receiver and shared with an arbitrary number of helpers; (2) A bi-weekly printed press product, customisable by caregivers; (3) A set of digital inclusion aids, freely accessible to each member of the ecosystem.
To value the "actor" status of the care receiver, each ecosystem {Care receiver (A), Helpers and Health Professionals} is called A's tribe. A tribe is thus articulated around the care receiver (A), who is called the tribe leader, and his or her caregivers, called A's watchers or A’s scouts depending on their level of intimacy with A. Mementop allows an arbitrary number of them to be hosted.
Tribal leader A can then manage his tribe, i.e., invite helpers of his choice or dismiss them. The tribal leader is free to promote a watcher to the rank of scout. A's scouts have specific privileges to access information published within A's tribe and can thus consult confidential elements.
3.1 Description of the Mementop application
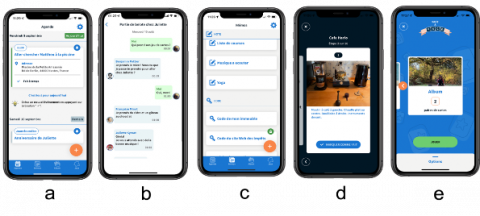
The first version of Mementop was released at the end of 2021. It offers to a tribe, via a unified user experience, several key functions providing practical answers to the functional challenges identified (Figure 1). Each of the elements is based on the privacy rules described above.
Figure 1. Functional perimeter of Mementop V1: a: Activity diary; b: Dedicated messaging for each event; c: Memo details; d: Memory album; e: Games
(1) Co-organisation and communication function: The activity diary contains events that are shared by tribe members according to their role (watcher or scout), and instantly synchronized. The diary allows a visualization of the tribe leader daily’s activities with simplified time markers. The tribe leader can organize himself, communicate with their loved ones, remain active, be guided, or accompanied and be reassured. A dedicated thread of integrated instant messaging is attached to each event to facilitate tribal communication and avoid any loss of information.
(2) Each event has the following characteristics: Confidentiality: {private - confidential - public}; Title; and Timing: Date and {Start time, duration} or time range, with recurrence also programmable. Optional are the Address (possible guidance to the indicated location), Description, marking (to indicate that the tribal leader must affirm that an event has been completed) and Reminder (default 10 minutes before the event starts). Examples: Appointments, medication, birthdays, scheduled visits, phone calls to be made or received.
(3) Exosomatic memory: Memos offer a shared digital safe, dedicated to the secure storage of information whose loss would be detrimental to the autonomy of the tribe leader. Particularly easy to find in the Mementop app, they can thus be used at any time. A rudimentary taxonomy is proposed: codes, passwords, medical prescriptions, notes, instructions for use. Each memo can contain a sequence (ordered list) of items or steps, like a recipe or the instructions to use a coffee machine. There are two ways of consulting the memos. The classic mode gives access to the details of the memo. The "play" mode allows the user to go through the steps associated with the memo one by one, each one being presented in full screen, the passage to step n+1 (if it exists) being possible only after the user has confirmed that step n has been considered (completed). Particularly useful for a "user manual" type memo, this visualization option facilitates the performance of procedural activities which sometimes pose difficulties for people in a situation of cognitive decline.
(4) Cognitive and social stimulation: Games have been designed with the help of neurologists and ND experts to optimize the user's level of engagement while stimulating memory and cognitive abilities and avoiding failure. They consider the cultural references and interests of the users. The level of play is adjustable. Three games are available in version 1 of the application. Word to word is an adaptation of the letter game "Boggle". The aim is to find as many words as possible by forming chains of letters from a board containing 16 dice. Face to face is an adaptation of the memory game "Memory". The aim is to reform pairs of identical images. The application offers many themes and allows the user to play with the images collected by the tribe in their memory album. This option maximizes the emotional impact of the game. The third invites users to reconstruct anagrams.
3.2 Description of the printed press product: Mementop gazette
The biweekly printed gazette aims to provide temporal reference points, to encourage social links and to stimulate the care receiver (and their caregivers) through activities specifically designed to engage them and enable them to be active daily, while helping to preserve their independence. Through the proposed activities, the ambition is to enhance the skills of the care receiver and to provide them with moments of pleasure throughout the week. Paper, a familiar, reassuring and appreciated element for seniors, encourages tactile stimulation and sharing between the members of the tribe. Each 16-page issue of the Mementop gazette is based on a specific theme close to the cared-for.
(1) Guiding the care receiver and increasing his/her autonomy. Half a page per day is dedicated to the indication of spatio-temporal reference points, namely the date of the day in full (name of the day of the week + dd mm yyyy), the ephemeris, the times of sunrise and sunset, the plus or minus time of day, the phase of the moon and two columns to be filled in with the activities: One for the morning and the other for the afternoon. A gentle gymnastics activity is also proposed to take care of the body. Finally, a recipe is specifically formulated to enable the care receiver to cook despite their neuro-evolutionary disorders.
(2) Soothe the care receiver and increase the social link. Photos can be personalized by caregivers directly via the Mementop application. A reminiscence activity encourages the sharing of memories. Finally, the recipe is a family recipe for sharing the dish made with the family.
(3) Stimulating the assisted in a multi-sensory way. Different elements are used, in relation with the theme, to stimulate the memory of the reader in a passive way. The play activities are adapted to the care receiver to stimulate him or her in an active way (about fifty activities have been identified around letters, numbers, logic, visuals, etc.). A creative activity (drawing, mandala, painting on wood, making objects, etc.) is also available. Finally, the recipe is presented in such a way that the care receiver can carry it out despite his eventual neurodegenerative disorders.
3.3 Description of digital inclusion support
To support each user, whether they are a care receiver or a caregiver, a set of elements has been put in place both to make the application easier to learn and to guide its use. This is all the more important given the sometimes-limited digital literacy of users, especially the elderly. Human resources are available by telephone and e-mail to answer any queries and to guide each user through each situation that arises in daily life. A welcome booklet for the care receiver is sent to them when they register. It details step by step the procedure to follow to use each function of the application. Video tutorials are made available to illustrate the main actions that can be carried out on the application. A forum is available for users to create a community and exchange their problems and tips.
Mementop’s socio-technical construct targets in priority seniors in GIR 4, 5 or 6, i.e., being autonomous or needing occasional help or not for washing, preparing meals and cleaning [9]. In the context of a ND, the declaration of aphasia will certainly mark a definitive limit in terms of the ability to use Mementop by the subjects concerned. It generally appears in phase 6 (of 7) of the development of the disease. Further research is therefore required for more advanced stages of dependence.
Although the ergonomics and accessibility of the socio-technical construct have been tested throughout the design process, there are still limitations and adjustments are needed.
Data collected by the Mementop device, resulting from the different actions of the members of each tribe, also allow the calculation of clinical health indicators, namely Nutrition; Hygiene; Sleep quality; Social behavior; Self-esteem; General autonomy. From a critical volume of data, it will be possible to represent the evolution over time of each clinical health indicator (study of their gradients) using techniques derived from Artificial Intelligence to predict the evolution of the autonomy of the care receiver. It will then be possible to anticipate a need for specific care, resulting for example from a detected risk of undernutrition, and to try to counter this estimated evolution, by soliciting the members of the tribe and, if necessary, by alerting health professionals. The collection of data can also enable further personalization according to the user's profile (expectations, needs, cultural preferences, lifestyle habits, etc.).
The user experience must also evolve to enhance the engagement of every member of the tribe. Research continues to improve: (1) Intrinsic motivation, obtained by the meaning given to interactions, by the integration of gamification elements and by the valorization of each individual; (2) Cognitive and social stimulation, on an individual level as well as through inter- and intra-tribal dynamics, notably through play activities; (3) Dynamic personalization of the experience through AI and the integration of an empathetic conversational agent; (4) Somatic memory to secure users, and facilitate transmission, sharing and support.
Finally, the clinical validation of the Mementop socio-technical construct remains to be demonstrated through a large clinical study planned for the period 2023-2025. It will include 220 triads - leader of a tribe affected by a ND - watcher - referring health professional - spread over the whole French territory. This study will aim to study the medical aspects (preservation of caregivers' autonomy; relief of the mental burden of the watchers and the scouts; improvement of the efficiency of the management by the health professionals) as well as the economic aspects concerning each tribe (exogenous costs related to medical visits, hospitalizations, and medical treatments; endogenous costs related to the expenses related to the health status of the tribe leader and his watchers and scouts).
This innovative and interdisciplinary research has led to a first version of the sociotechnical construct Mementop. Based on digital technology including AI, paper, and human interaction, it presents a major challenge for preserving the autonomy of seniors and people suffering from an ND, for relieving the mental burden on their caregivers and for improving the efficiency of care by health professionals. Research is continuing into the accessibility of digital technology for seniors, interface developments and advanced AI techniques to turn the Mementop medical device into an intelligent companion capable of predicting disease progression, relieving caregivers and providing personalized advice to delay situations of dependency.
[1] Thierry, D. (2012). Evaluation socio-environnementale de dispositifs domotiques associés à la téléassistance destinés à la prévention des chutes au domicile de personnes âgées en perte d’autonomie en Creuse. Project DOMOLIM SOCIO. Final Report for the 2012 Call for Research about Handicap and Loss of Autonomy, 3rd Session of the “Institut de Recherche en Santé Publique”. https://www.cnsa.fr/documentation/162-dantoine-rapport.pdf.
[2] Barnard, Y., Bradley, M.D., Hodgson, F., Lloyd, A.D. (2013). Learning to use new technologies by older adults: Perceived difficulties, experimentation behaviour and usability. Computers in Human Behavior, 29(4): 1715-1724. https://doi.org/10.1016/j.chb.2013.02.006
[3] Motti, L.G., Vigouroux, N., Gorce, P. (2015). Ease-of-use of tactile interaction for novice older adults. In International Conference on Human Aspects of IT for the Aged Population, pp. 463-474. https://doi.org/10.1007/978-3-319-20892-3_45
[4] Ben-Sadoun, G., Berrut, G., Bernat, V. (2018). Longévité et Métropole: Innovation pour les seniors, de quoi parlons-nous ? https://www.carsat-pl.fr/files/live/sites/carsat-pl/pdf/partenaires/rapport-gerontopole-debat-longevite-2018.pdf.
[5] Lazaro, C., Le Métayer, D. (2015). Le consentement au traitement des données personnelles. Perspective comparative sur l’autonomie du sujet. Revue juridique Themis, 48(3): 765-815. https://pure.unamur.be/ws/files/55399011/7585.pdf.
[6] Billi, M., Burzagli, L., Catarci, T., Santucci, G., Bertini, E., Gabbanini, F., Palchetti, E. (2010). A unified methodology for the evaluation of accessibility and usability of mobile applications. Universal Access in the Information Society, 9(4): 337-356. https://doi.org/10.1007/s10209-009-0180-1
[7] Fisk, A.D., Czaja, S. J., Rogers, W.A., Charness, N., Czaja, S.J., Sharit, J. (2009). Designing for older adults: Principles and creative human factors approaches. Designing for Older Adults. https://doi.org/10.1201/9781420080681
[8] Collet, L., Durampart, M., Gagnebien, A., Lépine, V. (2021). Dispositif de prise en charge de patients atteints de dégénérescence cognitive: enjeux communicationnels et redéfinition des rôles aidés, aidants, soignants. In Numérisation de la société et enjeux en santé: Transformation des espaces, des processus et des relations, pp. 11-12. https://doi.org/10.3917/gs.141.0195
[9] Benaim, C., Froger, J., Compan, B., Pélissier, J. (2005). Évaluation de l'autonomie de la personne âgée. In Annales de Réadaptation et de Médecine Physique, 48(6): 336-340. https://doi.org/10.1016/j.annrmp.2005.04.005