Noor Dheyaa Azeez* | Niebal Younis Mohammed
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Mobile patient monitoring systems are among the most important systems that seek to enhance the efficiency and effectiveness of services provided to patients. The study would aim to investigate the influencing factors of ambulatory patient monitoring system adoption from the patients' perspective. The proposed model in this study included the (UTAUT2) factors of the extended unified theory of technology acceptance with the addition of a confidence factor. To collect the data, a questionnaire was used, which was distributed to 200 participants. The results of the study showed that performance expectations, price value, effort expectation, and confidence positively and significantly affect behavioral intention. Moreover, in the last section, the study's directions and future directions will be discussed.
mobile health monitoring services, AUTAUT2, trust, structure equation modeling (SEM)
E-Health refers to specific technologies of information and communication that use for health"[1, 2]. Mobile Health, is considered one of the components of e-health, as health care is provided through the use of personal digital assistants, cell phones, or any other devices, which leads to reducing the cost of health care [3, 4]. Mobility provides freedom from time and space constraints for health care providers and recipients, making it easier to participate in healthcare delivery [5]. Mobile health includes mobile applications for general medical practices to provide health-related information, patient screening, the process of monitoring patients' physiological signs and providing direct care to them, as well as educating patients with these applications [6]. "MPMS is a part of the telemedicine, indicate a remote supply of persons with community support and nursing care. Likewise, telehealth indicates to the provision of delivered public health services to people who are not certainly sick, but who wish to remain healthy and independent” [7].
Mobile Patient Monitoring System considers a special service provided by mobile health services through which vital signal data of patients which is provided by wearable sensors by patients are collected to healthcare centers or hospitals [8]. "The common health problems such as high blood pressure, arrhythmia, or diabetes, and patients are often advised to check with their doctors periodically for regular medical check-ups. A medical monitoring system is one of the efficient services for patients to get medical feedback as it is faster and gives them more confidence in personal control of their health and reduces the cost of medical care in a long term” [9]. accordingly, this study focused on mobile health monitoring and public perceptions about it.
This study attempts to underline the relevance of real and actual use of the service and awareness of service for users.
This study aims to investigate the perspective of users of mobile health monitoring services, by taking different user and non-user perceptions about the factors that can be effective to the acceptance of mobile health monitoring services. it performs a deep and knowledgeable inspection of users’ interests and needs. In addition to that, it sets practical guidance on how mobile health monitoring services can be designed and delivered by service-developer providers. A literature review on the acceptance of telemedicine services was conducted to find out the patients' perceptions that have an impact on the acceptability of telemedicine services, through which the study reveals four perceptions: accessibility, communication, service risk, and intimacy.” The four perceptions were identified within three main categories related to the patient’s perception of accepting telemedicine services, namely: 1) benefit and harm factors, 2) merit factors, and 3) Harm factors. The literature shows that using medical services made patients realize that it will improve their health [9-11] and it will provide health care or health records that are not restricted in space and time [11-13]. In addition, patients realized that the use of Telemedicine includes communicating with health service providers, the clinical institution, hospital staff, and other users, and patients experienced a feeling of emotional connectedness between them and service providers through trust, respect, and sympathy; However, they have indicated their concern about these factors" [13-15]. On the flip side, patients had a state of doubt of the telemedicine service [16, 17].
2.1 E-Health
The term E-Health is a common unifying and collective definition of multiple technologies and modalities, it refers to "the use of emerging information and communication technology, especially the Internet, to improve or enable health and health care” [18, 19]. Electronic health communication tools have become particularly important. The process of patient empowerment of self-efficacy behaviors usually occurs during short sessions at the clinic after several days [7]. The eHealth System is a new paradigm for mainstream computing to provide high-quality health care backed by electronic health data and communications processing [20]. The term "e-health" refers to health services and information that is easily updated about health and is improved or provided by the Internet and related technologies [The Impact of eHealth on the Quality and Safety of]. e-health refers, as an effective field of medical informatics, to the organizing, delivering and consuming of online health services and related information and technologies. In particular, the concept surpasses technical development to include" a new way of working, position, and commitment to global network thinking to improve local, regional and global health care using ICTs" [21, 22].
Telemedicine, according to Fischer et al. [23, 24], is defined as the use of telecommunication technology to provide medical information and services that allows transmission of audio, visual, and digitized data using broad telephonic communication. Communication improvements and lower costs helped health care providers to combine traditional healthcare delivery systems with telemedicine. In addition to the progress made in technology and applications. Telemedicine and telehealth services help allow the chronic disease to be monitored remotely [25]. Telemedicine procedures can be transformed from telemedicine clinics into individual mobile healthcare and personal accommodations at home or at work [26].
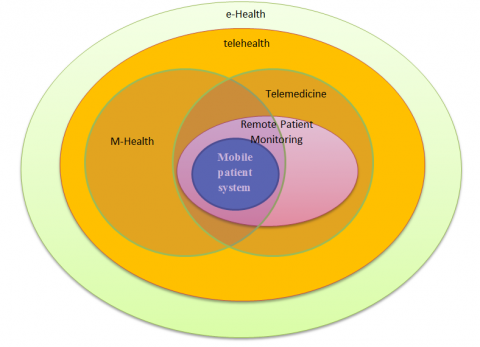
Mobile health "(M-Health), is a medical practice of a health care using mobile phones, personal digital assistants (PDAs) and other wireless devices provides a potentially cost-effective solution" [27]. Mobility is fundamental and essential to the concept of participatory healthcare. It works to provide freedom from spatial and temporal constraints for both recipients and health care providers, and thus facilitates participation in health care [5]. “For mobile applications and devices the clinical use of it is increasing. Doctors indicated that M-Health will become a health management tool of great importance in the near future. It can help citizens take responsibility for their health, move toward prevention rather than treatment, and reduce costly hospital visits”. "‘Mobile health (M-health) including mobile applications (‘Apps’): the practice of medicine and public health care supported by mobile technologies provide health information, check patients, monitor physiological signs, provide direct care and patient education" [6, 28], Figure 1 illustrates the relationship between electronic health models and ambulatory patient monitoring. Studies have shown that M-Health has a role in providing an opportunity for promising technological integration between healthcare service. Therefore, “M-Health is central to the widespread concept of health care as information services can reach anyone, anywhere, at any time, by removing all geographical, time and other barriers” [29, 30]. Monitoring is done by using external sensors that are not integrated into the mobile device. The sensors usually connect to the mobile device through Wi-Fi or short-range protocols such as Bluetooth [9]. The mobile device acts as a gateway to collect primary data from the sensors, then it is redirected to a separate system that processes it and retrieves data ready for visualization, by the patient himself or the doctors. A Systematic Review on Mobile Health Care. Effective smart health technologies are cost-effective, can cross language and cultural barriers, and can provide health services to areas where access to health services is low [7].
Figure 1. Relationship between e-health paradigms and mobile patient monitoring
2.2 Mobile patient monitoring system
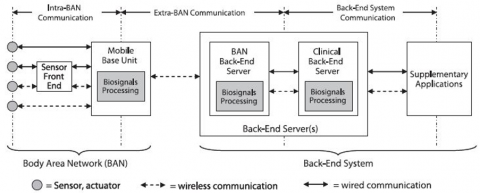
"Mobile Patient Monitoring (MPM) is a specific type of M-Health service, designed to provide a unified view of patient status and acquires patient's feedback, which refers to the continuous or frequent measurement, collect and transmit biosignal data already provided by wearable sensors from patients to a hospital or any health care center" [21]. Recently, the developing mobile patient monitoring systems (MPMS) have been done using wireless sensor technologies and mobile devices [31]. MPMS collects and monitors patients' vital signs and indicators such as body temperature (BT) and blood pressure (BP), in addition to monitoring a patient's physical activity such as running and walking [32]. MPMS uses environmental sensors to collect information about patients ’ambient environmental conditions such as light level, humidity, and room temperature [33]. “The architecture of the mobile patient monitoring system consists of a Back End System (BEsys) and a Body Area Network (BAN). (BAN) is a group of intercommunication devices that are worn on the patient's body, working to provide an integrated set of personal services to him, and it consists of a mobile base unit (MBU) and BAN devices (such as actuators, sensors or other wearable devices that are Use it for medicinal purposes)”. MBU works on a smartphone or personal digital assistant. “The connection between BAN components is known as Intra-BAN communication which can be wireless, wired, or a combination of them”. From the sensors the vital signal data is sent from directly to the MBU while some sensors require an intermediate data acquisition device called a Sensor Front-End (SFE) connected to the MBU via a wireless or wired link. In this case, analog vital signals are digitized and filtered by SFE before being sent to the MBU. Extra-BAN connection refers to the connection between BANs and the Back-End system, the connection must be a wireless link. Complementary applications are embedded in the BEsys and backend server (s) to process vital signals and data received by the servers.
In agreement with the presented definition of mobile patient monitoring, extra-BAN communication need to be strengthened by a wireless link. The MBU serves as a communication gateway that connects networks with different transmission protocols together for remote access to the patient's biosignals and medical data between the BAN and the user (e.g. a hospital or health professional), via the Back-End system. The biosignals may be processed locally within the BAN and/or remotely in the Back-End system. One Back-End system supports multiple monitored patients, i.e. multiple BANs are served by one Back-End system The BESys comprises the Database Server (Backend) and accessorial applications, their functions include processing biosignals and other data received by the servers. We distinguish the BAN Back-End to which the MBU transmits biosignals data from the Clinical Back-End” [8, 21]. Figure 2 shows the expanded architecture, which has been generalized to accommodate mobile patient monitoring systems.
Figure 2. A generic architecture of mobile patient monitoring systems
2.3 UTAUT
With the rapid advances in technology, in particular the technology of communication and information, and the incorporation of these technologies into users' lives, the question of acceptance or rejection of new technologies by users remains an open question 10. Acceptance of technology is linked to exploring the features of Mobile Health monitoring services and their relationships with user acceptance [34].
Over the years the adoption of technology has been repeatedly studied and examined. Some studies have focused on the relationships between technology adoption and variables that influence it, such as TAM and UTAUT. UTAUT has been tested and applied to various technologies, such as instant messaging and online billboards [35]. The UTAUT Model includes four main combinations: 1) anticipating effort, 2) anticipating performance, 3) social impact, and 4) facilitating the situation. The UTAUT model has several advantages that could be of use to this study. The UTAUT model was developed by many powerful models that determined that the UTAUT model is basic, robust, and appropriate, "this model accounts for 69% of the indentation for using IT, which is slightly higher than other theoretical models". Last but not least, the UTAUT model has been used frequently in the fields of healthcare research [36].
"This study relied on four factors of the unified acceptance theory and the use of the technology model proposed by Venkatesh et al. [37]". The proposed model can provide an understanding of the user's acceptance of the technology [10].
2.4 Previous studies
The study and examination of patients’ intentions and the adoption of the mobile monitoring system and the services provided through mobile channels has been the focus of attention of scientists and practitioners around the world, and this field has witnessed a growth in the literature related mobile health monitoring, Table 1 shows a number of studies that dealt with this topic.
Table 1. Previous studies
|
Ref |
Title |
year |
|
[31] |
“The study objective was to evaluate nurses’ perception of the ease of use and usefulness of PDA application, designed with customerized design principles” |
2009 |
|
[22] |
“Factors of adoption of mobile Information Technology by Homecare Nurses: a technology Acceptance model 2 approach” |
2010 |
|
[32] |
“Factors affecting mobile diabetes monitoring adoption among physicians: questionnaire study and path model” |
2013 |
|
[23] |
“m-Health adoption by healthcare professionals: a systematic review” |
2015 |
|
[25] |
“Mobile patient monitoring systems from a benchmarking aspect: challenges, open Issues and recommended solutions” |
2019 |
Based on the table above explain [38] this study dealt with the evaluation of the nurses' perception in terms of the ease of use of the personal digital assistant application, which was designed depending on the user's requirements and the extent of the application's usefulness for nurses [29]. This study conducted an empirical study depended on the technology acceptance model in ambulatory home care nursing. The sample of the study were 91 Canadian nurses random who used personal digital assistants in their daily activities for a month [39]. this study examined the factors affecting the adoption of mobile health monitoring for Japanese doctors, and the study sample was diabetics [30]. the aim of the study is to collect current knowledge of the factors that have an impact on healthcare professional adoption of mobile health applications through systematic review [32]. this study provided comprehensive insights into ambulatory patient monitoring systems according to two main directions: assessment and measurement. The current evaluation criteria for mobile patient monitoring systems formulated on its architectural components and possible solutions were discussed.
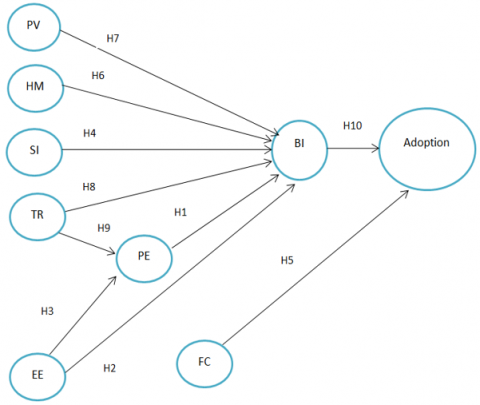
The UTAUT2 theory has been proposed to illustrate the acceptability of the technology from the patient's perspective. Therefore, in an attempt to choose a suitable model that includes all the combinations through which the Iraqi patient's intention is determined and the mobile patient monitoring systems adopted, the UTAUT2 model was used as a theoretical basis to suggest the conceptual model to be used. Figure 3 shows the main factors in UTAUT2: average voltage (EE) and expectation of performance (PE), motive pleasures (HM), social impact (SI), and the price value (PV) is suggested as major and direct determinants of intent patient in adopting mobile patient monitoring systems. Agree with [40], two factors: Facilitating conditions (FC) and behavioral intentions (BI) both have been identified as major predictors of behavior for adopting mobile patient monitoring systems. Rather than what was suggested before [40], The current study model does not take into account the role of habit. This is because when examining the role of the habit factor, the patient must have experience in using this technology. The respondents in “this study are potential users who have not tried this technology or have not used this type of system yet.
Figure 3. Proposed conceptual model [40, 41]
Figure 3 proposed conceptual model [40, 42]. Therefore, in this study the role of habit was difficult to study and was excluded. According to the previous literature of ambulatory patient monitoring systems, trust (TR) is widely accepted as a critical factor in determining client reception and intent to adopt such [43]. This interest is due to the nature of mobile health services, which can be described as high-risk services as they are related to the lives of patients [10]. Therefore, trust was included in the proposed model as an exogenous factor in UTAUT2 [40].
3.1 Performance expectancy
Performance expectancy is defined as “the degree to which an individual believes that using the system will help him or her to attain gains in job performance” [44]. Venkatesh et al. It was found that the strongest determinant when adopting a new technology affects the behavioral intention of the user is PE [45]. Refers to the effect of BI when using health information systems with Performance expectancy. Study [46] also revealed that the expected effort has a positive and direct impact on the intention to use mobile devices. It has been empirically proven by Hoque & Sorwar [47] if there is an increase in the probability of adopting mobile health services as the PE increases. Therefore, this study demonstrates hypothesis as follow:
“H1. Performance expectancy has a positive effect on Iraq patients’ intention to appropriate mobile patient monitoring systems”.
3.2 Effort expectancy
EE is defined as “the degree of ease levels associated with the use of the system”. Previous studies indicated that energy efficiency has a powerful effect on users' intentions to adopt and accept a health information system. For instance, EE has been described as a significant factor that have an immediate impact on intention of users to use mobile health monitoring systems, e-Health services via a smartphone, clinical decision support systems and mobile health [47-49]. Thus, this study hypothesizes he following:
“H2. The effort expectancy has a positive effect on intention of Iraqi patient to adopt mobile patient monitoring systems”.
“H3. The effort expectancy has a positive effect on performance of mobile patient monitoring systems”.
3.3 Social influence
Social influence is defined as “the degree to which an consumer conceives that important others believe he/she should use the new system” [50]. Study [48] reported that social influence has an effect on behavioral intention when using mobile health services [47] "identified a significant co-relationship between SI and users’ behavioral intention to use digital information in healthcare. As per the above discussion, the following hypothesis was posited”:
“H4. Social influence has a positive effect on Iraqi patients’ intention to adopt mobile patient monitoring systems.
3.4 Facilitating conditions
Facilitating conditions is defined as “the degree to which consumers believe that an organizational and technical infrastructure presents to support the use of the system” [37, 51]. "A study by Brown & Venkatesh [52] estimated that FC positively influences the behavioral intention and use behavior of using smartphones for health services". Based on the foregoing, the following hypothesis was developed:
“H5. Facilitating conditions has a positive effect on Iraqi patient’ adopt mobile patient monitoring systems”.
3.5 Hedonic motivation
It’s defined the hedonic motivation from the consumer's perspective as “the fun or pleasure derived from using a technology” [40]. For an extended period, when patients need to receive health care services, they will go to the hospital, and the services will be provided to them face to face. And considering that mobile health has specific characteristics, it has become an alternative channel for receiving services for some medical problems, which are comprehensively dominated by patients' preferences that have behavioral components and emotional and cognitive beliefs [53]. Based on the foregoing, enjoyment can have a strong influence on behavioral motivation in the case of adoption of portable health which is defined “as the emotional pleasure or risen from the use of this alternative health care service system”.
“H6. Hedonic motivation has a positive effect on Iraqi patient’ adopting mobile patient monitoring systems”.
3.6 Price value
In the context of the user, when evaluating user acceptance and actual use behavior [40], "extended the original UTAUT model by placing UTAUT2 with the insertion of price-value among others to exchange the sharing consumers' aforementioned preference". When a consumer purchases a service or product, the consumer preference for choosing a particular brand is controlled by exchanging money for the value generated from the product [54]. Under this concept, cognitive evaluation of a user's belief in price value is a factor that has a significant impact on adoption behavior. Venkatesh et al. [40] defined price-value as “consumers' cognitive trade-off between the perceived benefits of the applications and the monetary cost for using them”. Mobile health is an alternative channel for accessing healthcare services. Perhaps this channel may not be a substitute for the physical presence in the hospital. So why would patients be interested in accepting a new health care service that is unfamiliar? Among several reasons, highlighting the transaction cost analysis, researchers can conclude that price value is a strong determinant when identifying the behavior of patients for the adoption of health services through the mobile phone; This has broad support from previous literature, the researchers redefine a mobile health price value as “the cognitive trade-off between the values experienced by citizens through the use of the mobile health service system as an alternative channel to the health care service receiving the alternative system and the financial costs including the opportunity cost of its use.” So the following hypothesis can be formulated:
“H7. Price value will positively influence Iraqi patient ’intention to mobile patient monitoring systems”.
3.7 Trust
Trust plays a significant role in the adoption of a new IT [55]. Previous studies confirm that trust is an important and basic condition of social behavior and is positively related to users' intentions when using the Internet store [56], purchasing books on the internet, e-government services [57], and mobile payment [58]. From a mobile health services perspective, Heart & Kalderon [59] showed that patients' confidence positively affects the intention to adopt mobile health services. According to the findings at the later stage of adoption. Theorists conceptualized trustworthiness (belief in trust) in mobile health service research and indicated that trustworthiness positively affects user trust (trust intent), which directly affects the Patients' continuity intentions. In subsequent research, Meng et al. [60] showed that perceived trust has a positive effect on satisfaction with mobile health services and intention to continue using them. Since m-Health is a personalized service, trust plays a large and important role in anticipating users' adoption intentions. Elderly individuals face greater difficulties when using new technology, and have little experience using mobile health services. Since the subject of health is sensitive, users may pay more attention to health services obtained through mobile channels. So the following hypotheses was proposed:
“H8. Trust has a positive effect on Iraqi patients’ intention to adopt mobile patient monitoring systems”.
“H9. Trust has a positive effect on the performance expectancy associated with using mobile patient monitoring systems”.
3.8 Behavioral intention
Previous literature in the field of information systems/information technology showed that behavioral intention has a major role in adopting and using new systems [55, 61]. Accordingly, this study hypothesizes that the adoption of ambulatory patient monitoring systems can be significantly predicted by patients' willingness to adopt the system. This relationship has been proven in a number of studies related to mobile monitoring systems such as [62], So the following hypothesis was proposed:
“H10. Behavioral intention has a positive effect on Iraqi patients’ adoption of mobile patient monitoring systems”.
To validate the proposed model, data were collected, and 200 subjective questionnaires were allocated to obtain responses from patients regarding their perception of aspects associated with behavioural intention and adoption of ambulatory monitoring systems. use of 36 scale items in this study to measure the basic structures in the model. In particular, the major constructs of UTAUT2 (EE, PE, FC, SI, PV, HM, and BI) were measured with the same ones used by Okazaki et al. [30, 39-41] validating their new model (UTAUT2). “Patients’ trust in mobile patient monitoring systems was measured by six items taken. Conceptually, Ho et al. [41, 63] have defined trust as “individual willingness to depend based on the beliefs in ability, benevolence, and integrity”. In the line with Gefen et al. [41, 60], Patient trust in this study was defined as an accumulation of trust beliefs: benevolence, integrity, and ability that correlate with the ambulatory patient monitoring systems channel. Therefore, trust items have been selected in a way that includes these aspects and as documented by Zhang et al. [29, 48, 59]. In this study, the five-point Likert scale was used to measure the respondents' responses to the elements of the proposed model. “Finally, four questions were assigned to the demographic variables: gender, age, education level, and mobile experience”. Bearing in mind that in this study the language of the respondents was Arabic, and the reverse translation method was relied upon to convert the study questionnaire into Arabic to avoid the impact of linguistic and cultural differences.
5.1 Respondents profile and characteristics
The descriptive statistics showed that with regard to age, the group that obtained the highest percentage was the 25-40 age group, while in terms of sex, the percentage of males was 65.6% and the percentage of females was 34.4% of the total respondents. The descriptive statistic, with regard to mobile experience, also indicates that the majority of respondents (92.8%) have sufficient experience in the mobile phone field (more than 3 years), as for the educational level, a bachelor's degree obtained a percentage (72.3%).
5.2 Structural equation modeling analysis
To analyze the collected data, structural equation modeling was used. A two-step SEM analysis used, the first one is to evaluate the measurement model and the second step is to estimate the structural model. All combinations of the model and the confidence factors were subjected to the measurement model analysis and then the structural model analyzes were carried out. It is worth noting that the structural model was examined without trust. It was necessary to perform this process to see how the predictive power of the proposed model varies with and without trust.
5.2.1 Measurement model: Confirmatory factor analysis
Firstly the (unidimensionality) model fitness was tested in CFA and then an assessment of constructs reliability and validity was carried out.
5.2.2 “Model fitness
Main fitness indices including CMIN/DF, CFI, AGFI, RMSEA, and GFI were tested to assess model fit. The resulting fitness indices for the standard model for ambulatory patient monitoring systems were as follows: CMIN/DF 2.066, AGFI = 0.769, GFI = 0.88, CFI = 0.885 and RMSEA= 0.062, As seen in Table 2. Some of these indicators did not reach the acceptable value (ie, GFI) [64], so to enhance the fit of the model re-evaluation and purification were performed [65].
The model optimization process adopted a number of criteria to improve the fit of the model by examining factor loading (standardized regression weights) [65] .By inspecting of (factor loading) standardised regression weights , one item (BI3)from Behavioural Intention ,one item (Hm4)from hedonic motivation and one item (FC2) from facilitating conditions, and one item (BE2) from performance expectancy and one component of the facilitating conditions (FC2) was less than its terminal value (<0.50) [64, 65]. Hence, the decision was to remove these four items.
The CFA test was performed a second time without the extra elements, and the model's fitness improved significantly. Since the value of the chi-square (DF=465, CMIN=343.651, P = 0.000), the rest of the indicators suitable for the modified measurement model were found, within the recommended ones. Values: CMIN/DF was 1.841, GFI=0.90, AGFI=0.80, CFI=0.90, and RMSEA=0.062 [64]. Accordingly, the modified scaling model proved to be adequate to the data [64, 65].
Table 2. Results of measurement model
|
“Fit indices” |
“Cut- off point” |
“Initial measurement model” |
“Modified measurement model” |
|
“CMIN/DF” |
“≤3.000” |
“2.066” |
“1.841” |
|
“GFI” |
“≥0.90” |
“0,88” |
“0.90” |
|
“AGFI” |
“≥0.80” |
“0.769” |
“0.80” |
|
“CFI” |
“≥0.90” |
“0,88” |
“0.90” |
|
“RMSEA” |
“≤0.08” |
“0.062” |
“0.062” |
5.2.3 Structural model
The statistical results obtained for the fit indicators of the structural model indicate that the structural model is adequately fitted to the data. In the path factor analysis, the causal pathways suggested in the conceptual model supported to be significant. Accurately, behavioral intention was found to be predicted by UTAUT2 factors: mean effort (CR=4.482, P<0.00), pleasure motivation (CR=5.418, P<0.00), price value (CR=2.42, p<0.01), social influence and (CR=4.71, p<0.00). However, the results did not support the performance expectation pathway with behavioral intention (CR=0.97, p<0.32), and the effort expectation pathway with behavioral intention was not a significant path t (CR=-1.76, p<0.07). As for the two main combinations of predicting performance, the results showed that both mean expected effort (CR=4.482, p<0.00) and trust (CR=4.456, p<0.05) have a significant effect on predicting performance. Finally, it was found that adoption of mobile health monitoring services was predicted by both the facilitated conditions (CR=4.003, p<0.00) and behavioral intention (=0.467, p<0.001).
Therefore, the research hypotheses were confirmed: H3, H5-H10, while two hypotheses: H1 and H2 were rejected. R2 values extracted for internal factors were as follows: 31% for adoptive behavior, 65% for behavioral intentions; 49% for expected performance; It is worth noting that confidence was not included when examining the structural model. As expected, factors of the UTAUT2 model (without confidence) had the ability to predict behavioral intention by about 59%.
However, when the trust was included in the UTAUT2 model the R2 value representing behavioral intent was boosted up to 65%. Thus, it can be concluded that the structural model has greater power to predict behavioral intention when the confidence factor is added.
The statistical results proved that the proposed model of the study was able to reach an acceptable level of predictive power for all internal structures: adoption behavior (32%), behavioral intention (65%), and average performance (49%). In addition, “the criteria related to the measurement model all achieved success in the validity and suitability of the model and the reliability of the construction”. And in the UTAUT2 model the trust factor is included, the value of the extracted R2 increases to reach 65%, and this result supports confidence as an external factor in the proposed model.
Therefore, this result is fairly close to the value of the variance that has been explained by other studies that rely on the UTAUT model. For example, the study conducted by [29] “study the adoption of mobile information technology by home care nurses”.
In the path analysis, it was found that the confidence coefficient value of 0.26 proved to be an important factor for predicting patients' intention when adopting ambulatory health surveillance. Moreover, the value of the trust path with the expected performance was 0.24, which is an important path. This indicates that trust has an important role not only to motivate patients to use Mobile health monitoring but, also to contribute to formation of patients' perception of this technology as a new technology. “This can be attributed to the sensitive nature associated with patient transactions carried out through the mobile phone [1, 3, 4]. These results are in agreement with what has been validated by IS field studies and Mobile health monitoring studies associated with the role of trust” [5, 39].
“Statistical results showed strong evidence the path weight of the path between behavioral intent and mean performance 0.19, which confirms this path. This result indicates that the aspects related to performance expectation are among the patients' attention that affect their intention to adopt and use Mobile health monitoring”.
Results showed that the relationship is not significant with a regression weight of 0.18 between behavioral intention and expectation of effort when adopting the “mobile health monitoring”. This result clearly shows that patients are concerned about use of mobile health monitoring system. This could be due to patients' concern that they need to have special skills to deal with mobile health monitoring services [30]”.
The statistical results confirmed the effect of the expected effort on the performance expectation. In other words, if patients realize that using technology is not difficult and requires less effort, they will rely more on it in different areas of life [66]. Previous literature reviews in the fields of information system /information system Demonstrate the impact of the ease of use of a system on individuals perception of the benefit of the system [66]. Along the same lines, several studies in the field of mobile health monitoring indicated a relationship between the ease of use of the system and its usefulness [29]. The results confirmed the role of social influence in behavioral intention., which indicates the possibility of the influence of relatives and friends on patients' intention when adopting the mobile health monitoring system.
Statistical results (=0.153, p<0.021) confirmed the existence of an effect of facilitating conditions on the adoption of mobile health monitoring. This indicates respondents' interest in having the skills and resources required to ensure the successful use of mobile health surveillance. Indeed, in the case of mobile health monitoring the required facilities (i.e. smartphones, internet access, Wi-Fi, 4G services, secure applications) are important factors to ensure easy access to services. This result is consistent with the results of studies that dealt with facilitating conditions.
As expected, tasty motivation has been experimentally demonstrated with values (=0.20, p<0.000) to be an important factor influencing patients' intention when adopting ambulatory health surveillance. This strong correlation increases the likelihood that the adoption of ambulatory health monitoring can reach a high level among patients who find it fun when using this type of system [52, 53]. In the study model, the statistical results confirmed presence of pathways between patients' intention to adopt mobile health monitoring and the price value a weight of 0.15. Accordingly, this finding indicates that price-value issues are of interest to patients influencing their decision to reject or adopt a mobile health monitoring, in line with Muhayiddin et al. [67]. Furthermore, a significant the number of respondents in this study were middle-income and therefore more price sensitive [52, 54].
Despite the fruitful attempt of this study in the field of mobile health surveillance adoption, there are a number of limitations that have been encountered. For example, the sample approved in the study included an appropriate sample of patients in only two Iraqi cities (Nineveh and Erbil), which could have a negative impact if generalized to other cities. Description of the sample showed that the largest segment of respondents are young people, with middle incomes, and have sufficient experience in using a mobile phone and the Internet. Therefore, these may raise concerns in terms of the applicability from outcomes to other categories of the population may have different characteristics (e.g. education level, gender, age, income level, technological experience). The results of this study are based on cross-sectional data, and to obtain a broader understanding of this problem, a longitudinal study can be conducted.
This is due to the fact that the rate of adoption of the mobile health monitoring system is still slow in Iraq, patients have not yet been able to form a habitual behavior towards it, Therefore, from the proposed model, the habit factor was excluded. However, in the long run, once Mobile health monitoring system is used and patients get used to it, patients can form a habitual behavior towards, and therefore future studies can discuss the role of habit factor in actual behavior and intention.
The mobile health monitoring system represents one of the important areas that needs to be studied and examined, especially with the great challenges accompanying this type of technology, and the low rate of adoption of mobile health monitoring. Therefore, the current study realized the need to examine the factors that have a role in shaping the intention and adoption of the mobile health monitoring system, and what This is encouraged by the presence of a small number of studies examining the problems associated with the mobile health monitoring system. Moreover, a need arose to select a theoretical basis capable of capturing Aspects related to the adoption of the mobile health monitoring system, and thus the UTUAT2 model was selected in this study. To expand the model, the confidence factor was added as an external factor, which is considered one of the important factors affecting patients' intention to adopt the new technology.
[1] Furusa, S.S., Coleman, A. (2018). Factors influencing e-health implementation by medical doctors in public hospitals in Zimbabwe. South African Journal of Information Management, 20(1): 1-9. https://doi.org/10.4102/sajim.v20i1.928
[2] Alsalem, M.A., Zaidan, A.A., Zaidan, B.B., Hashim, M., Madhloom, H.T., Azeez, N.D., Alsyisuf, S. (2018). A review of the automated detection and classification of acute leukaemia: Coherent taxonomy, datasets, validation and performance measurements, motivation, open challenges and recommendations. Computer Methods and Programs in Biomedicine, 158: 93-112. https://doi.org/10.1016/j.cmpb.2018.02.005
[3] Mohsin, A.H., Zaidan, A.A., Zaidan, B.B., et al. (2018). Real-time medical systems based on human biometric steganography: A systematic review. Journal of Medical Systems, 42(12): 1-20. https://doi.org/10.1007/s10916-018-1103-6
[4] Jacob Rodrigues, M., Postolache, O., Cercas, F. (2020). Physiological and behavior monitoring systems for smart healthcare environments: A review. Sensors, 20(8): 2186. https://doi.org/10.3390/s20082186
[5] Cameron, J.D., Ramaprasad, A., Syn, T. (2017). An ontology of and roadmap for mHealth research. International Journal of Medical Informatics, 100: 16-25. https://doi.org/10.1016/j.ijmedinf.2017.01.007
[6] Táborský, M., Linhart, A., Skalická, H. (2017). e-Health: A position statement of the European Society of Cardiology. Cor et Vasa, 2(59): e204-e207.
[7] Dedding, C., Van Doorn, R., Winkler, L., Reis, R. (2011). How will e-health affect patient participation in the clinic? A review of e-health studies and the current evidence for changes in the relationship between medical professionals and patients. Social Science & Medicine, 72(1): 49-53. https://doi.org/10.1016/j.socscimed.2010.10.017
[8] Pawar, P., Jones, V., Van Beijnum, B.J.F., Hermens, H. (2012). A framework for the comparison of mobile patient monitoring systems. Journal of Biomedical Informatics, 45(3): 544-556. https://doi.org/10.1016/j.jbi.2012.02.007
[9] Parmanto, B., Lewis Jr, A.N., Graham, K.M., Bertolet, M.H. (2016). Development of the telehealth usability questionnaire (TUQ). International Journal of Telerehabilitation, 8(1): 3-10. https://dx.doi.org/10.5195/ijt.2016.6196
[10] Lee, J., Rho, M.J. (2013). Perception of influencing factors on acceptance of mobile health monitoring service: a comparison between users and non-users. Healthcare Informatics Research, 19(3): 167-176. https://doi.org/10.4258/hir.2013.19.3.167
[11] Yip, M.P., Chang, A.M., Chan, J., Mackenzie, A.E. (2003). Development of the Telemedicine Satisfaction Questionnaire to evaluate patient satisfaction with telemedicine: A preliminary study. Journal of Telemedicine and Telecare, 9(1): 46-50. https://doi.org/10.1258%2F135763303321159693
[12] Lee, S.H. (2002). Electronic resources and collection development (Vol. 36). Psychology Press.
[13] Varkey, P., Schumacher, K., Swanton, C., Timm, B., Hagen, P.T. (2008). Telemedicine in the work site: A study of feasibility, and patient and provider satisfaction. Journal of Telemedicine and Telecare, 14(6): 322-325. https://doi.org/10.1258%2Fjtt.2008.080512
[14] Katz, S.J., Moyer, C.A. (2004). The emerging role of online communication between patients and their providers. Journal of General Internal Medicine, 19(9): 978-983. https://doi.org/10.1111/j.1525-1497.2004.30432.x
[15] Shore, J.H., Brooks, E., Savin, D., Orton, H., Grigsby, J., Manson, S.M. (2008). Acceptability of telepsychiatry in American Indians. Telemedicine and e-Health, 14(5): 461-466. https://doi.org/10.1089/tmj.2007.0077
[16] Houston, T.K., Sands, D.Z., Jenckes, M.W., Ford, D.E. (2004). Experiences of patients who were early adopters of electronic communication with their physician: satisfaction, benefits, and concerns. Am J Manag Care, 10(9): 601-608.
[17] Lim, N. (2002). Classification of Consumers' Perceived Risk: Sources versus Consequences. In Proceedings of the Sixth Pacific Conference on Information Systems, Tokyo, Japan, pp. 540-554.
[18] Eng, T.R. (2001). The eHealth landscape: A terrain map of emerging information and communication technologies in health and health care.
[19] Whittaker, F. (2013). Electronic communities of care-Measuring the benefits. Doctoral dissertation, University of Southern Queensland.
[20] Fernández-Alemán, J.L., Señor, I.C., Lozoya, P.Á.O., Toval, A. (2013). Security and privacy in electronic health records: A systematic literature review. Journal of Biomedical Informatics, 46(3): 541-562. https://doi.org/10.1016/j.jbi.2012.12.003
[21] Varga, N., Bokor, L., Takács, A. (2014). Context-aware IPv6 flow mobility for multi-sensor based mobile patient monitoring and tele-consultation. Procedia Computer Science, 40: 222-229. https://doi.org/10.1016/j.procs.2014.12.030
[22] Jiang, L.C., Wang, Z.Z., Peng, T.Q., Zhu, J.J. (2015). The divided communities of shared concerns: Mapping the intellectual structure of e-Health research in social science journals. International Journal of Medical Informatics, 84(1): 24-35. https://doi.org/10.1016/j.ijmedinf.2014.09.003
[23] Fischer, U.M., Harting, M.T., Jimenez, F., et al. (2009). Pulmonary passage is a major obstacle for intravenous stem cell delivery: the pulmonary first-pass effect. Stem Cells and Development, 18(5): 683-692. https://doi.org/10.1089/scd.2008.0253
[24] Inumpudi, A., Srinivas, M., Gupta, D.K. (2001). Telemedicine in pediatric surgery. Pediatric Surgery International, 17(5): 436-441. https://doi.org/10.1007/s003830000528
[25] Barlow, J., Singh, D., Bayer, S., Curry, R. (2007). A systematic review of the benefits of home telecare for frail elderly people and those with long-term conditions. Journal of Telemedicine and Telecare, 13(4): 172-179. https://doi.org/10.1258/135763307780908058
[26] Weinstein, R.S., Krupinski, E.A., Doarn, C.R. (2018). Clinical examination component of telemedicine, telehealth, mHealth, and connected health medical practices. Medical Clinics, 102(3): 533-544. https://doi.org/10.1016/j.mcna.2018.01.002
[27] McCarroll, R., Eyles, H., Mhurchu, C.N. (2017). Effectiveness of mobile health (mHealth) interventions for promoting healthy eating in adults: A systematic review. Preventive Medicine, 105: 156-168. https://doi.org/10.1016/j.ypmed.2017.08.022
[28] Cowie, M.R., Bax, J., Bruining, N., et al. (2016). e-Health: a position statement of the European Society of Cardiology. European Heart Journal, 37(1): 63-66. https://doi.org/10.1093/eurheartj/ehv416
[29] Zhang, H., Cocosila, M., Archer, N. (2010). Factors of adoption of mobile information technology by homecare nurses: a technology acceptance model 2 approach. CIN: Computers, Informatics, Nursing, 28(1): 49-56. https://doi.org/10.1097/NCN.0b013e3181c0474a
[30] Gagnon, M.P., Ngangue, P., Payne-Gagnon, J., Desmartis, M. (2016). m-Health adoption by healthcare professionals: A systematic review. Journal of the American Medical Informatics Association, 23(1): 212-220. https://doi.org/10.1093/jamia/ocv052
[31] Ren, Y., Werner, R., Pazzi, N., Boukerche, A. (2010). Monitoring patients via a secure and mobile healthcare system. IEEE Wireless Communications, 17(1): 59-65. https://doi.org/10.1109/MWC.2010.5416351
[32] Almahdi, E.M., Zaidan, A.A., Zaidan, B.B., Alsalem, M.A., Albahri, O.S., Albahri, A.S. (2019). Mobile patient monitoring systems from a benchmarking aspect: Challenges, open issues and recommended solutions. Journal of Medical Systems, 43(7): 1-23. https://doi.org/10.1007/s10916-019-1336-z
[33] Paganelli, F., Giuli, D. (2010). An ontology-based system for context-aware and configurable services to support home-based continuous care. IEEE Transactions on Information Technology in Biomedicine, 15(2): 324-333. https://doi.org/10.1109/TITB.2010.2091649
[34] Sabri Tekantape, E., De Coster, R. (2018). Consumer Survey into Factors Influencing Mobile Health Monitoring Service perceptions in the UK.
[35] Im, I., Hong, S., Kang, M.S. (2011). An international comparison of technology adoption: Testing the UTAUT model. Information & Management, 48(1): 1-8. https://doi.org/10.1016/j.im.2010.09.001
[36] Puuronen, S., Vasilyeva, E., Pechenizkiy, M., Tesanovic, A. (2010). A holistic framework for understanding acceptance of Remote Patient Management (RPM) systems by non-professional users. In 2010 IEEE 23rd International Symposium on Computer-Based Medical Systems (CBMS), pp. 426-431. https://doi.org/10.1109/CBMS.2010.6042682
[37] Venkatesh, V., Morris, M.G., Davis, G.B., Davis, F.D. (2003). User acceptance of information technology: Toward a unified view. MIS Quarterly, 425-478. https://doi.org/10.2307/30036540
[38] Chang, P., Hsu, C.L., Lan, C.F. (2009). Is PDA good for complex documentation in healthcare? In Nursing Informatics, pp. 115-120.
[39] Okazaki, S., Castañeda, J.A., Sanz, S., Henseler, J. (2013). Physicians' appraisal of mobile health monitoring. The Service Industries Journal, 33(13-14): 1326-1344. https://doi.org/10.1080/02642069.2013.815737
[40] Venkatesh, V., Thong, J.Y., Xu, X. (2012). Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Quarterly, 36(1): 157-178. https://doi.org/10.2307/41410412
[41] Gefen, D., Straub, D. (2000). The relative importance of perceived ease of use in IS adoption: A study of e-commerce adoption. Journal of the Association for Information Systems, 1(8): 1-30.
[42] Gefen, D., Karahanna, E., Straub, D.W. (2003). Trust and TAM in online shopping: An integrated model. MIS Quarterly, 27(1): 51-90. https://doi.org/10.2307/30036519
[43] Hoque, M.R., Bao, Y., Sorwar, G. (2017). Investigating factors influencing the adoption of e-Health in developing countries: A patient’s perspective. Informatics for Health and Social Care, 42(1): 1-17. https://doi.org/10.3109/17538157.2015.1075541
[44] Pal, J.K., Hussain, M.M. (2016). Health care practices of older people in sylhet: A study conducted in slum areas of sylhet city of Bangladesh. International Journal of Humanities Social Sciences and Education (IJHSSE), 3(4): 90-100.
[45] Khan, N.U.Z., Rasheed, S., Sharmin, T., et al. (2015). Experience of using mHealth to link village doctors with physicians: lessons from Chakaria, Bangladesh. BMC Medical Informatics and Decision Making, 15(1): 1-9. https://doi.org/10.1186/s12911-015-0188-9
[46] Khatun, F., Heywood, A.E., Ray, P.K., Hanifi, S.M.A., Bhuiya, A., Liaw, S.T. (2015). Determinants of readiness to adopt mHealth in a rural community of Bangladesh. International Journal of Medical Informatics, 84(10): 847-856.
[47] Hoque, R., Sorwar, G. (2017). Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int J Med Inform., 101: 75-84. https://doi.org/10.1016/j.ijmedinf.2015.06.008
[48] Kabir, Z.N. (2001). The emerging elderly population in Bangladesh: Aspects of their health and social situation. Institutionen för klinisk neurovetenskap, arbetsterapi och äldrevårdsforskning (NEUROTEC)/Department of Clinical Neuroscience, Occupational Therapy and Elderly Care Research (NEUROTEC).
[49] Moudud-Ul-Huq, S., Sultana Swarna, R., Sultana, M. (2021). Elderly and middle-aged intention to use m-health services: an empirical evidence from a developing country. Journal of Enabling Technologies, 15(1): 23-39. https://doi.org/10.1108/JET-04-2020-0018
[50] Ortman, J.M., Velkoff, V.A., Hogan, H. (2014). An aging nation: The older population in the United States.
[51] Baabdullah, A.M., Rana, N.P., Alalwan, A.A., Islam, R., Patil, P., Dwivedi, Y.K. (2019). Consumer adoption of self-service technologies in the context of the Jordanian banking industry: Examining the moderating role of channel types. Information Systems Management, 36(4): 286-305. https://doi.org/10.1080/10580530.2019.1651107
[52] Brown, S.A., Venkatesh, V. (2005). Model of adoption of technology in households: A baseline model test and extension incorporating household life cycle. MIS Quarterly, 29(3): 399-426. https://doi.org/10.2307/25148690
[53] Dwivedi, Y.K., Shareef, M.A., Simintiras, A.C., Lal, B., Weerakkody, V. (2016). A generalised adoption model for services: A cross-country comparison of mobile health (m-health). Government Information Quarterly, 33(1): 174-187. https://doi.org/10.1016/j.giq.2015.06.003
[54] Lichtenstein, S., Williamson, K. (2006). Understanding consumer adoption of internet banking: An interpretive study in the Australian banking context. Journal of Electronic Commerce Research, 7(2): 50.
[55] Azeez, N.D., Lakulu, M.M. (2018). Evaluation framework of mgovernment services success in Malaysia. Journal of Theoretical and Applied Information Technology, 96(24): 8194-8226.
[56] Deng, Z., Hong, Z., Ren, C., Zhang, W., Xiang, F. (2018). What predicts patients’ adoption intention toward mHealth services in China: Empirical study. JMIR mHealth and uHealth, 6(8): e9316. https://doi.org/10.2196/mhealth.9316
[57] Azeez, N.D., Lakulu, M.M. (2019). Review the success of the mobile government from the government perspective. International Journal of Humanities, Management and Social Science, 2(2): 103-109. https://doi.org/10.36079/lamintang.ij-humass-0202.36
[58] Akter, S., Ray, P., D’Ambra, J. (2013). Continuance of mHealth services at the bottom of the pyramid: the roles of service quality and trust. Electronic Markets, 23(1): 29-47. https://doi.org/10.1007/s12525-012-0091-5
[59] Heart, T., Kalderon, E. (2013). Older adults: are they ready to adopt health-related ICT? International Journal of Medical Informatics, 82(11): e209-e231. https://doi.org/10.1016/j.ijmedinf.2011.03.002
[60] Meng, F., Guo, X., Peng, Z., Lai, K.H., Zhao, X. (2019). Investigating the adoption of mobile health services by elderly users: trust transfer model and survey study. JMIR mHealth and uHealth, 7(1): e12269. https://doi.org/10.2196/12269
[61] Xue, L., Yen, C.C., Chang, L., et al. (2012). An exploratory study of ageing women's perception on access to health informatics via a mobile phone-based intervention. International Journal of Medical Informatics, 81(9): 637-648. https://doi.org/10.1016/j.ijmedinf.2012.04.008
[62] Jaruwachirathanakul, B., Fink, D. (2005). Internet banking adoption strategies for a developing country: The case of Thailand. Internet research, 15(3): 295-311. https://doi.org/10.1108/10662240510602708
[63] Ho, K.K., See-To, E.W.K. (2010). An exploratory study on the impact of trust on different E-payment gateways: Octopus card vs. Credit Card, 475-486. https://aisel.aisnet.org/pacis2010/42.
[64] Hair, J.F., Gabriel, M., Patel, V. (2014). AMOS covariance-based structural equation modeling (CB-SEM): Guidelines on its application as a marketing research tool. Brazilian Journal of Marketing, 13(2). https://ssrn.com/abstract=2676480.
[65] Perlman, J.M., Wyllie, J., Kattwinkel, J., et al. (2010). Neonatal resuscitation: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Pediatrics, 126(5): e1319-e1344. https://doi.org/10.1542/peds.2010-2972B
[66] Davis, C.F. (1989). The evidential force of religious experience.
[67] Muhayiddin, M.N., Elsadiq, M.A., Ismail, H. (2011). User acceptance of an electronic dinar payment system in Malaysia. In: Innovation and Knowledge Management: A Global Competitive Advantage - Proceedings of the 16th International Business Information Management Association Conference, IBIMA 2011, pp. 1424-1434.