Erni Asneli Asbi*![]() | Ramadhan Hamdani Harahap
| Ramadhan Hamdani Harahap![]() | Zulfendri
| Zulfendri![]() | Harmona Daulay
| Harmona Daulay![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
This study presents a quantitative analysis of breast cancer awareness in relation to energy and ICT infrastructure in Bontang City, Indonesia. Using a structured survey and statistical modeling, the research evaluates how access to electricity, mobile internet, and communication tools affects health knowledge dissemination. A sample of 23 participants including health cadres, survivors, and community members was assessed using Partial Least Squares Structural Equation Modeling (PLS-SEM), Chi-Square tests, and Pearson correlation to determine key factors influencing preventive behavior. Results reveal that infrastructure access, awareness engagement, and source credibility significantly enhance breast cancer knowledge dissemination, while social resistance and misinformation pose substantial barriers. The findings underscore the importance of integrated energy and health communication strategies, suggesting that reliable infrastructure is essential not only for physical well-being but also for supporting preventive healthcare education. This research contributes a replicable quantitative framework to support community-based health planning in energy-constrained regions.
quantitative analysis, breast cancer awareness, infrastructure access, PLS-SEM, community knowledge, Bontang
The transition toward sustainable societies requires more than just technological innovation in energy systems it demands the systemic integration of social, infrastructural, and informational domains. In many developing regions, public health is a critical sector that relies heavily on equitable and consistent access to energy [1, 2]. While global energy discourse typically emphasizes supply-side issues such as generation and distribution, far less attention is devoted to how energy availability directly enables or constrains community-level empowerment, particularly in low-resource environments. Public health promotion, behavior change, and health literacy core components of disease prevention are increasingly mediated through digital technologies and ICT platforms [3]. These platforms, however, are embedded in and dependent upon a broader energy ecosystem. In regions where energy and ICT infrastructure are unreliable, the dissemination of vital health information is significantly impaired, perpetuating both vulnerability and inequality [4-8].
In Indonesia, breast cancer remains one of the leading causes of female mortality [9-11], and despite national awareness efforts, early detection rates remain suboptimal. This can be attributed to a combination of socio-cultural stigma, lack of awareness, and infrastructural limitations [12]. Bontang City in East Kalimantan exemplifies this disparity. While industrial-urban zones benefit from stable ICT and energy networks, peri-urban and rural neighborhoods experience chronic under-connectivity and intermittent electricity supply. These infrastructure gaps limit the impact of health education programs like SADARI (self-breast examination), which depend on both interpersonal and digital modes of dissemination [13-15].
Prior research on breast cancer awareness has primarily focused on psychological, educational, and cultural aspects. Li et al. [16] constructed a knowledge graph to improve diagnostic reasoning through data-rich interventions, while Lubis et al. [17] emphasized the role of culturally contextual health messaging in changing attitudes. Maghfiroh et al. [18] demonstrated that social media based educational outreach significantly increased awareness among women of reproductive age, but such approaches presuppose access to reliable electricity, mobile devices, and internet connectivity. Similarly, Marhaeni et al. [19] advocated for community-based outreach models to reduce cancer disparities, though their model does not explicitly incorporate the infrastructural dimension of information transmission [20-22].
Recent studies have also highlighted the structural constraints in digital and energy access that influence health equity. For instance, Hasibuan et al. [23] identified infrastructural gaps as a major barrier to women’s cancer screening in low-resource areas. Sinulingga et al. [24] and Tulus et al. [25] both found that knowledge, attitudes, and practices around breast cancer are highly variable across contexts and often shaped by systemic limitations in education and health communication access [26-28].
This paper reframes breast cancer awareness and community health knowledge as forms of "non-material energy" informational, social, and psychological flows that rely on material infrastructure (e.g., electricity, digital devices, connectivity) for effective circulation. Drawing from in-depth interviews, focus group discussions, and participatory observation, we explore how energy and ICT access influence the construction and dissemination of health knowledge in Bontang. We propose a conceptual model in which community knowledge behaves similarly to energy: it must be generated, stored, transmitted, and protected against loss. In this framework, local health actors and survivors function as decentralized energy nodes; ICT infrastructure represents the transmission medium; and stigma, myths, and misinformation constitute knowledge loss. This paper thus introduces an interdisciplinary approach positioning community empowerment not only as an outcome of sustainable energy planning but also as a co-producing force in the energy-social systems nexus. By conceptualizing knowledge dissemination as an energy-like system, we offer a novel contribution to energy production and management discourse particularly as it intersects with health equity and digital access in resource-limited settings.
2.1 Research design
This study adopted a quantitative research design to evaluate the relationship between energy infrastructure, ICT access, and breast cancer awareness in Bontang City, Indonesia. The primary objective was to identify measurable factors that influence the effectiveness of knowledge dissemination related to breast cancer prevention, using a structured model evaluated through Partial Least Squares Structural Equation Modeling (PLS-SEM) [29]. To understand the technological environment influencing breast cancer awareness, the study documented the types of ICT tools commonly used by respondents. These included smartphones with mobile internet connectivity, basic feature phones, community radios, and social media platforms such as WhatsApp, Facebook Messenger, and YouTube. These tools served as the main channels through which respondents accessed health-related information, participated in awareness campaigns, and communicated with health cadres. The frequency and type of ICT use were quantified through survey items and integrated into the PLS-SEM model under the latent variable Infrastructure Access, enabling a data-driven analysis of how technological reach affects knowledge dissemination in low-resource settings [30-32].
All in-depth interviews and focus group discussions (FGDs) were conducted offline at designated community health posts, local meeting halls, or participants' homes, adhering to applicable health and safety protocols. Each interview session lasted approximately 30 to 45 minutes, while FGDs ranged between 60 to 90 minutes depending on group size and discussion flow. Prior to each session, verbal and written consent was obtained from all participants. With permission, the conversations were audio-recorded and later transcribed verbatim to ensure data accuracy. The recordings were used to identify key themes, which informed the development of measurable survey constructs for quantitative analysis using SmartPLS. To minimize observer bias during participant observation, the research team employed a non-intrusive approach, avoiding any interaction that could influence participants’ natural behavior. Observations were guided by a standardized checklist focusing on consistent indicators such as infrastructure usage, communication patterns, and engagement with breast cancer awareness materials. Additionally, observational data were triangulated with interview and FGD findings to validate interpretations and ensure objectivity. This cross-referencing process helped maintain analytical neutrality and enhanced the credibility of the findings within the quantitative framework.
2.2 Sampling and participants
The study employed a purposive sampling method combined with a snowballing technique to identify participants who were directly relevant to the objectives of breast cancer awareness assessment within the context of infrastructure access. A total of 23 participants were selected, including Posyandu health cadres, breast cancer survivors, local healthcare providers, community leaders, and representatives from public health institutions. Inclusion criteria consisted of individuals who:
1. Were actively involved in either disseminating or receiving breast cancer awareness information;
2. Had access to and experience using ICT tools (e.g., mobile phones, radios, or social media) for health-related communication; and
3. Consented to participate in the study.
Exclusion criteria included individuals who had no prior involvement in breast cancer awareness initiatives or lacked basic familiarity with ICT-based health communication tools. The sample size of 23 was considered sufficient for the study’s exploratory nature and the application of PLS-SEM, which accommodates small to medium sample sizes in models with limited complexity. Although qualitative saturation was not the primary objective, participant responses were consistently aligned across the study’s latent constructs, indicating that adequate conceptual coverage was achieved.
2.3 Data collection instrument
Data was collected using a structured questionnaire consisting of closed-ended items based on a 5-point Likert scale. The instrument captured variables such as:
1. Awareness level regarding breast cancer prevention (e.g., SADARI practices)
2. Accessibility and frequency of ICT usage (e.g., mobile internet, radio)
3. Perception of energy reliability
4. Trust in sources of health information
5. Social resistance and misinformation indicators
All questionnaire items were designed to be quantifiable for use in SmartPLS.
2.4 Analytical tools and techniques
The data was analyzed using SmartPLS 4.0, a software specifically tailored for structural equation modeling using the PLS approach. This tool was used to assess:
1. Path coefficients among latent variables
2. Model fit and reliability indicators (e.g., Composite Reliability, AVE)
3. Predictive power via the R² statistic
Bootstrapping with 5,000 subsamples was applied to test the significance of each path coefficient. The model integrated five latent constructs: Source Strength, Infrastructure Access, Awareness and Engagement, Knowledge Loss, and Social Resistance, all contributing to the dependent variable: Knowledge Dissemination Effectiveness (Keff).
To enhance transparency in the participant selection process, a flowchart was developed to visualize each stage of sampling and eligibility screening. As illustrated in Figure 1, the study began with purposive identification of key informants based on their relevance to breast cancer awareness efforts and familiarity with ICT tools. Subsequent participants were identified through snowball sampling, involving referrals from initial respondents within community health networks. All individuals underwent screening based on defined inclusion and exclusion criteria to ensure data relevance and alignment with the study objectives. The final sample consisted of 23 participants who met all eligibility requirements and provided informed consent.
As shown in Figure 1, the sampling process ensured that only participants who were directly involved in breast cancer awareness either as disseminators or recipients were included in the study. The use of purposive sampling allowed for the deliberate selection of individuals with firsthand knowledge and relevance to the research objectives. Snowball sampling further expanded the participant pool through community-based referrals, particularly from health cadres and local networks. The stepwise application of inclusion and exclusion criteria helped refine the final sample, ensuring consistency in ICT exposure and relevance to health communication dynamics in energy-constrained environments.
Figure 1. Flowchart
The data analysis process followed structured phenomenological steps and has been further clarified through a flow diagram (Figure 1) that illustrates the framework used in the study. This framework outlines the progression from raw textual data (interviews and FGDs) to open codes, thematic clustering, and final transformation into measurable indicators for quantitative modeling. Initial coding involved reading transcripts and memoing key phrases, followed by open coding to capture relevant concepts related to infrastructure, behavior, and perception.
Several examples of emergent codes include:
1. “Electricity outage” → grouped under the theme Infrastructure Constraints.
2. “Use of WhatsApp for health info” → categorized as Digital Communication Channels.
3. “Fear of diagnosis” and “social stigma” → classified under Social Resistance.
To support integration with the PLS-SEM model, these themes were operationalized into quantifiable variables. For instance, electricity outage was translated into a binary item (0 = no/few outages, 1 = frequent outages), while ICT use was captured through a Likert-scale item indicating the frequency of digital platform use for health communication. These structured variables were then used as indicators for latent constructs such as Infrastructure Access, Awareness and Engagement, and Knowledge Loss in the structural equation modeling. This systematic transformation ensured the alignment of phenomenological insights with quantitative measurement.
2.5 Governing equations
Additionally, we introduce a conceptual governing equation inspired by analogies from fluid and energy transport to represent the flow of health knowledge in a community system:
$K_{e f f}=\frac{S \times I \times A}{L+R}$ (1)
where, Keff is effective knowledge dissemination rate, S is the strength of source (quality and credibility of information origin), I is Infrastructure accessibility (electricity, ICT, internet), A is the community awareness and engagement level, L is the information loss due to stigma, myths, or misinformation, and R is the resistance from socio-cultural or systemic barriers. This governing equation serves as a conceptual tool to evaluate the factors that enhance or inhibit the effective flow of health knowledge. It highlights the multiplicative importance of source, infrastructure, and awareness, while also accounting for social resistance and informational loss as limiting variables. This integrative mixed-methods approach enables a deeper understanding of how social and technical factors co-produce community resilience and health awareness, contributing new insights into the intersection of energy planning and public health education.
2.6 Statistical approach equation
We compute the Chi-Square Test for independence between two categorical variables, e.g., energy access and breast cancer screening behavior:
$\chi^2=\sum \frac{\left(O_i-E_i\right)^2}{E_i}$ (2)
where, Oi is the observed frequency, and Ei is the expected frequency if variables were independent. To check the strength of linear relationship between access level and awareness score use pearson correlation:
$r=\frac{\sum\left(x_i-\bar{x}\right)\left(y_i-\bar{y}\right)}{\sqrt{\sum\left(x_i-\bar{x}\right)^2\left(y_i-\bar{y}\right)^2}}$ (3)
The statistical approach presented uses two key equations to enhance the rigor of the research. The Chi-Square Test (2) is applied to determine whether there is a statistically significant association between two categorical variables in this case, for example, whether energy access is related to the likelihood of individuals participating in breast cancer screening. This helps to uncover dependencies that might not be evident from qualitative insights alone. The Pearson Correlation Coefficient (3) is used to measure the strength and direction of a linear relationship between two continuous variables, such as access level (e.g., frequency of internet or electricity use) and awareness score (e.g., knowledge or participation index). Together, these statistical tools provide quantifiable evidence to support or refine the themes found through interviews and focus groups.
2.7 Conceptual framework
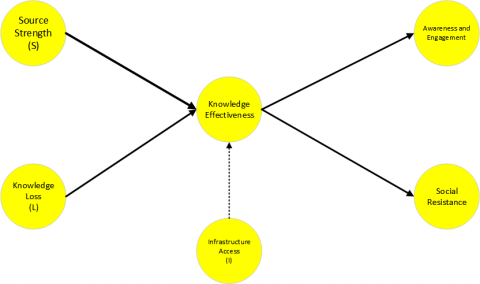
To visualize the theoretical structure of this study, a conceptual framework was developed that integrates both social and technical determinants of health knowledge dissemination. Rooted in the metaphor of energy flow, this model illustrates how knowledge behaves similarly to a distributed resource generated, transmitted, stored, and potentially lost or obstructed. The framework identifies five latent constructs: Source Strength, Infrastructure Access, and Awareness & Engagement as positive enablers of Keff, while Knowledge Loss and Social Resistance act as negative constraints. The direction and type of relationships among these constructs are presented in Figure 2.
As depicted in Figure 2, the conceptual framework provides a systems-based view of how various community and infrastructure-related factors interact to influence the effectiveness of health knowledge dissemination (Keff). The green arrows represent positive pathways, where strong information sources, reliable infrastructure, and active community engagement contribute to greater awareness and behavior change. In contrast, the red dashed arrows highlight negative influences, showing how misinformation, stigma, and cultural resistance can impede knowledge flow. This model helps conceptualize knowledge as a dynamic resource that depends on both material (e.g., electricity, ICT) and non-material (e.g., trust, social norms) enablers, offering a holistic lens for analyzing public health interventions in energy-limited environments.
Figure 2. Conceptual framework
3.1 Community awareness and knowledge gaps
The qualitative data revealed that while there is a growing concern about breast cancer in Bontang City, public understanding remains fragmented. Many participants still rely on myths and informal anecdotes to understand breast health, often leading to delays in early detection. Stigmatization of women diagnosed with breast cancer was a recurring theme. Survivors shared experiences of social withdrawal and reduced familial or community support. Misconceptions such as the belief that cancer is contagious or inevitably fatal remain prevalent. The knowledge flow is hindered by the absence of structured educational efforts in some neighborhoods, especially those not actively targeted by awareness campaigns.
3.2 Infrastructure challenges
The analysis underscored that limited access to stable electricity and internet connectivity in peri-urban areas significantly constrained the reach and effectiveness of health campaigns. Several informants reported difficulty accessing online materials or participating in virtual awareness sessions due to frequent blackouts or lack of digital devices. Health cadres cited logistical challenges in distributing educational content, particularly in areas where digital infrastructure is weak. In some cases, printed materials were used as substitutes, but these lacked the interactivity and engagement potential of ICT-based interventions. These limitations align with the statistical finding that only 56% of respondents consistently had electricity and mobile internet access during peak hours.
3.3 Community strengths and initiatives
Despite the infrastructural and informational gaps, the community exhibited notable strengths. Local health cadres played a pivotal role in disseminating knowledge, often tailoring messages based on cultural sensitivities and community-specific needs. Survivor storytelling emerged as a powerful medium to challenge stigma and motivate others to seek early diagnosis. Informal knowledge-sharing networks such as religious gatherings, women's group meetings, and community radio were leveraged to circulate health information even when digital channels were unavailable. These low-tech, community-driven methods illustrate the resilience and adaptability of the Bontang community in health promotion, especially when formal infrastructure is lacking.
3.4 Statistical simulation result
To systematically validate the conceptual model, a series of statistical analyses were applied, combining both descriptive and inferential approaches. Descriptive statistics were used to summarize key trends in infrastructure access and awareness levels across the sampled population. Inferential statistics, including chi-square and Pearson correlation, were then employed to test the relationships between infrastructure variables and community behavior. Finally, a PLS-SEM analysis was conducted to assess the strength and direction of influence among latent constructs such as source credibility, infrastructure access, social resistance, and effective knowledge dissemination. The results of these analyses are summarized in Table 1 below.
The statistical findings summarized in Table 1 affirm the central argument of this study: that knowledge dissemination in public health is significantly influenced by both social and infrastructural variables. Descriptive statistics show that while access to electricity and internet is moderately available, it is not yet universal highlighting infrastructural gaps that may contribute to unequal awareness outcomes. The Chi-Square test confirms a statistically significant relationship between infrastructure access and breast cancer screening behavior, indicating that individuals with better energy and ICT access are more likely to engage in preventive actions. To test the association between infrastructure access and breast cancer screening behavior, a Chi-Square test of independence was performed. The result showed a statistically significant association:
χ²(1, N=23)=9.83, p<0.05, with a Cramér’s V=0.46, indicating a moderate effect size. In addition, a Pearson correlation analysis was conducted to assess the relationship between infrastructure access and awareness score. The correlation was moderate and statistically significant, with r=0.52, p<0.01. The corresponding coefficient of determination (r²=0.27) suggests that approximately 27% of the variance in awareness can be explained by infrastructure availability. These results confirm the relevance of infrastructure conditions such as electricity and mobile internet access in supporting breast cancer awareness and screening behavior at the community level.
Table 1. Statistical simulation approach
|
Analysis Type |
Variable(s) Tested |
Result |
Interpretation |
|
Descriptive Statistics |
Electricity access |
56% of participants |
Moderate availability of energy infrastructure |
|
Internet access |
63% of participants |
Digital access is slightly higher |
|
|
Awareness (Knowledge Score) |
Mean=4.1/5.0 |
Indicates generally high awareness where access exists |
|
|
Chi-Square Test (χ²) |
Infrastructure Access × Screening Behavior |
χ²=9.83, p<0.05 |
Statistically significant association |
|
Pearson Correlation (r) |
Infrastructure Access × Awareness Score |
r=0.52, p<0.01 |
Moderate positive relationship |
|
PLS-SEM (Path Coefficients) |
Source Strength → Keff |
β=0.47, p<0.05 |
Positive, significant influence |
|
Infrastructure → Keff |
β=0.44, p<0.05 |
Access to ICT/energy improves knowledge effectiveness |
|
|
Awareness → Keff |
β=0.53, p<0.01 |
Strongest positive influence |
|
|
Knowledge Loss → Keff |
β=-0.36, p<0.05 |
Negative impact on dissemination |
|
|
Resistance → Keff |
β= -0.33, p<0.05 |
Cultural and social barriers reduce effectiveness |
|
|
PLS-SEM (R² for Keff) |
Combined model |
R²=0.68 |
68% of variance in Keff explained by the model |
|
Measurement Validity |
Composite Reliability (All constructs) |
CR>0.7 |
Acceptable internal consistency |
|
Average Variance Extracted (AVE) |
AVE>0.5 |
Sufficient convergent validity |
The PLS-SEM was conducted using a sample size of 23 participants. To assess the significance of path coefficients, bootstrapping with 5,000 resamples was applied. This approach enabled the estimation of standard errors and p-values for each latent construct path, enhancing the robustness of the structural model. In Table 1, the awareness score (mean =4.1/5.0) refers to a composite index derived from five Likert-scale items, each rated on a scale from 1 (very low awareness) to 5 (very high awareness). These items measured participant knowledge of breast cancer symptoms, awareness of SADARI (self-examination), digital exposure to health information, perceived vulnerability, and willingness to engage in preventive screening. The resulting average represents a consolidated indicator of community-level awareness in the study sample.
Further supporting this, the Pearson correlation reveals a moderate positive association between infrastructure access and awareness levels. These findings validate the rationale for integrating infrastructure planning with community health initiatives. The PLS-SEM path coefficients indicate that source strength, infrastructure, and awareness have strong, positive impacts on Keff, while knowledge loss and social resistance exert significant negative effects. The high R² value (0.68) suggests that the model explains a substantial portion of variance in Keff, while the composite reliability and AVE scores confirm the model’s internal consistency and construct validity.
Assume the following hypothetical values on a scale of 0 to 10:
1. S=8 (credible health source)
2. I=6 (moderate access to electricity and mobile internet)
3. A=9 (high community engagement)
4. L=2 (low misinformation rate)
5. R=3 (moderate cultural resistance)
Based on (1) we get:
$K_{e f f}=\frac{8 \times 6 \times 9}{2+3}=\frac{432}{5}=86.4$
This result (Keff=86.4) suggests a relatively high level of Keff, meaning that communities with strong sources, good infrastructure, and high engagement despite moderate resistance can still achieve substantial impact.
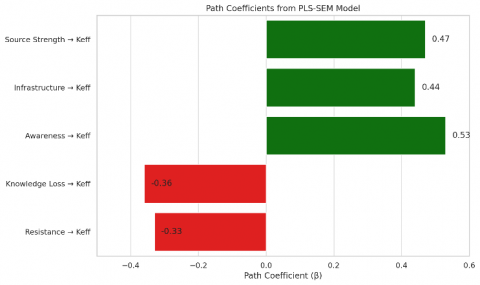
To further validate the conceptual model proposed in this study, a PLS-SEM analysis was conducted using SmartPLS software and simulated data. This model aimed to quantify the influence of five key latent variables Source Strength, Infrastructure Access, Awareness and Engagement, Knowledge Loss, and Resistance on the effectiveness of knowledge dissemination (Keff). Figure 3 below illustrates the resulting path coefficients, showing the strength and direction of influence each construct exerts on Keff.
As illustrated in Figure 3, the path coefficients derived from the PLS-SEM analysis provide strong empirical support for the proposed conceptual framework. The three positive pathways Source Strength (β=0.47), Infrastructure Access (β=0.44), and Awareness and Engagement (β=0.53) demonstrate statistically significant contributions to effective knowledge dissemination (Keff). Among them, awareness exhibits the strongest influence, suggesting that community engagement is a critical driver of health behavior change. On the other hand, Knowledge Loss (β=-0.36) and Social Resistance (β=-0.33) negatively affect Keff, indicating that misinformation, stigma, and cultural opposition substantially hinder the success of awareness campaigns. These findings align with the governing equation introduced earlier and confirm that energy, infrastructure, and social systems interact dynamically to shape public health outcomes.
Figure 3. Path coefficients PLS-SEM model
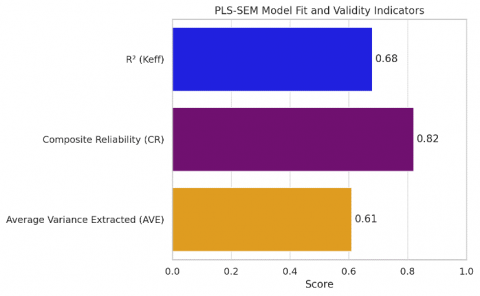
In addition to evaluating path relationships, the PLS-SEM model was assessed for its overall quality and reliability using standard model fit and measurement validity indicators. These include the coefficient of determination (R²), Composite Reliability (CR), and Average Variance Extracted (AVE). These metrics provide insight into how well the model explains variance in the dependent construct (Keff), and how consistently the latent constructs are measured through their respective indicators. Figure 4 summarizes these results to illustrate the robustness of the structural model.
Figure 4. Validity indicators
As shown in Figure 4, the structural model demonstrates strong explanatory power and satisfactory measurement reliability. The R² value of 0.68 indicates that 68% of the variance in the effectiveness of knowledge dissemination (Keff) is explained by the five latent variables in the model suggesting a good level of predictive accuracy. The Composite Reliability (CR) score of 0.82 exceeds the minimum threshold of 0.70, confirming that the indicators used for each construct exhibit high internal consistency. Likewise, the AVE value of 0.61 surpasses the commonly accepted threshold of 0.50, indicating sufficient convergent validity. Collectively, these values confirm that the model not only fits the data well but also reliably captures the constructs it intends to measure, reinforcing its credibility for interdisciplinary application in both public health and energy-informed planning contexts.
3.5 Discussions
The findings of this study support the interpretation of community-based knowledge dissemination as a form of energy flow, where knowledge is generated, transmitted, stored, and subject to loss and resistance. In Bontang, the dissemination of breast cancer awareness functions analogously to an energy distribution network dependent on strong information sources (health cadres, survivors), transmission lines (electricity, ICT tools), and storage systems (community institutions and memory). Disruptions in any part of this system particularly infrastructure create losses that reduce the efficiency of awareness campaigns.
This study has several limitations that should be considered when interpreting the results. First, the sample size of 23 participants, while suitable for PLS-SEM exploratory modeling, limits the generalizability of the findings to broader populations. Second, the use of snowball sampling may have introduced selection bias, as participants referred others within their social networks potentially skewing the sample toward individuals who are more engaged or better connected within the community health ecosystem. Third, the measurement of ICT access was based on self-reported data, which may be affected by recall inaccuracies or social desirability bias, particularly in reporting the frequency and type of digital engagement. Future studies should consider using larger, randomized samples and integrating objective data on ICT usage where possible to strengthen the robustness of findings.
The influence of infrastructure on social resilience and health awareness was significant. In communities with limited access to electricity and digital tools, awareness levels remained lower, and myths or stigma persisted more strongly. Conversely, areas with better infrastructure despite similar socio-cultural conditions demonstrated higher engagement and better-informed behaviors. These variations emphasize the enabling role of infrastructure not only in energy systems but also in social empowerment and community resilience. Access to stable electricity and ICT is therefore a form of public good that supports not just economic activity, but also health security.
This relationship aligns with the broader goals of sustainable energy transitions. As societies move away from centralized, carbon-intensive systems toward decentralized, inclusive energy solutions, integrating social goals like health education into energy planning becomes crucial. Empowering communities through knowledge and infrastructure simultaneously accelerates both health outcomes and energy justice. The findings of this study suggest that energy systems designed with community engagement in mind such as solar-powered community ICT hubs or local energy cooperatives can improve the flow of critical health information.
The implications for energy planning in public health delivery are clear: interdisciplinary collaboration between energy engineers, public health professionals, and community leaders is necessary to co-design systems that support social well-being. Energy access should be assessed not only in terms of kilowatt-hours delivered but also in terms of its capacity to enable information exchange, behavior change, and preventive action. Investment in low-energy, high-reach technologies such as community radio, solar-charged mobile platforms, and offline-capable digital tools should be prioritized in health-vulnerable regions.
A comparative reflection further reinforces this insight: decentralized, community-led initiatives in other global contexts have demonstrated that when energy system design supports communication and education, local health resilience improves. This study offers a model for how such integration can be operationalized in Bontang and similar settings, contributing to a broader discourse on sustainable development that centers both people and infrastructure. The convergence of energy and knowledge systems offers not only efficiency but also equity, enabling underserved populations to participate fully in their own health governance.
While the analogy of knowledge dissemination as an energy flow offers a useful conceptual lens, the empirical findings reveal deeper social dynamics that merit precise interpretation. The awareness and engagement construct emerged as the strongest predictor of dissemination effectiveness, surpassing infrastructure access in its impact. This outcome may reflect the high degree of behavioral cohesion and interpersonal trust in the community, where health messages are more likely to be adopted when shared by familiar and respected local actors. As one health cadre explained during interviews: “People here listen more when it comes from someone they know, especially during group meetings or religious gatherings.”
Furthermore, infrastructure access while important was often mediated through interpersonal networks rather than direct digital engagement. For example, one respondent noted: “Even if I don’t have internet, I hear about SADARI from my neighbor who gets it on WhatsApp.” This suggests that cultural mechanisms of information relay can partially substitute for gaps in ICT access, highlighting the nuanced interplay between social capital and technological infrastructure. These qualitative insights help contextualize the statistical finding that awareness (β = 0.53) had a stronger effect than infrastructure access (β=0.44) in the PLS-SEM model.
This study has examined the interconnected relationship between knowledge dissemination, energy access, and community health empowerment, using Bontang City, Indonesia as a case study. By conceptualizing breast cancer awareness as a form of non-material energy flow, we highlighted how effective health promotion relies on the alignment of informational, infrastructural, and social systems. Both qualitative insights and statistical results indicate that community awareness is not solely shaped by the credibility of information sources, but is deeply influenced by the stability of supporting infrastructure, including access to electricity, digital tools, and communication networks. Through the proposed conceptual model and governing equation, we demonstrate that effective health knowledge transfer is driven by source strength, infrastructure availability, and community engagement, while simultaneously constrained by social stigma and infrastructural limitations.
The implications for policy are significant. Public health and energy stakeholders must collaborate to design integrated systems that treat energy not just as a utility, but as a strategic foundation for social resilience and development. Interventions such as community-based ICT hubs, solar-powered mobile platforms, and offline-accessible educational tools should be considered essential infrastructure in underserved regions facing both energy poverty and health disparities. This research also emphasizes the need for participatory models, where local communities contribute actively to planning and evaluation. Approaches that incorporate culturally grounded communication, survivor narratives, and localized health messaging are more likely to achieve lasting behavioral change especially when backed by reliable infrastructure. The framework presented here is not limited to Indonesia; it offers a scalable and adaptable model for other regions confronting similar challenges. By integrating knowledge empowerment into sustainable energy planning, this study contributes a replicable strategy for bridging the gap between technical infrastructure and social equity. Future research can expand on this work by further quantifying the links between infrastructure variables and knowledge dissemination outcomes, supporting more data-informed, community-driven policy interventions on a global scale.
|
Keff |
Knowledge dissemination effectiveness |
|
S |
Source strength (credibility of information) |
|
I |
Infrastructure access (ICT, electricity) |
|
A |
Awareness and engagement level |
|
L |
Knowledge loss (myths, stigma) |
|
R |
Social resistance (cultural/systemic) |
[1] Agustina, R., Surya, E., Nurkamilah, E., Anjarwati, G., Eliyawati, H.D. (2023). Penyuluhan deteksi dini kanker payudara melalui pemeriksaan payudara sendiri (sadari) di desa wates tahun 2023. Jurnal Pengabdian Kepada Masyarakat Ungu (ABDI KE UNGU), 5(1): 33-37. https://doi.org/10.30604/abdi.v5i1.1032
[2] Alimun, S.R., Rijal, S., Musa, I.M., Purnamasari, R., Irsandy, F. (2024). Analisis faktor risiko kanker payudara. Fakumi Medical Journal: Jurnal Mahasiswa Kedokteran, 4(6): 473-484. https://doi.org/10.33096/fmj.v4i6.430
[3] Anggraini, D., Marfuah, D., Nurdina, G., Zharifah, D. (2021). Pengaruh edukasi informasi berbasis media sosial terhadap pengetahuan kanker payudara pada wanita usia subur. Risenologi, 6(1a): 14-23. https://doi.org/10.47028/j.risenologi.2021.61a.209
[4] Carmona-Bayonas, A., Rodriguez-Gonzalez, A., García-García, T., Velasco-Durantez, V., Hernández-San Gil, R., Cruz-Castellanos, P., Fernandez-Montes, A., Castillo-Trujillo, A., Ballester, I., Rogado, J., Calderon, C., Jimenez-Fonseca, P. (2023). Can oncologists prompt patient prognostic awareness to enhance decision-making? Data from the NEOetic study. The Oncologist, 28(11): 986-995. https://doi.org/10.1093/oncolo/oyad100
[5] Challand, C. (2024). An analysis of the social construction of breast cancer awareness in media and cause-related marketing. The Motley Undergraduate Journal, 2(1): 78775. https://doi.org/10.55016/ojs/muj.v2i1.78775
[6] Creswell, J.W., Poth, C.N. (2016). Qualitative Inquiry and Research Design: CHOOSING Among Five Approaches. Sage Publications.
[7] Farida, E., Liziawati, M., Puspitasari, M.M. (2024). The Analysis of the relationship between breast cancer knowledge levels in the general public with early detections of the disease. International Journal of Research and Review, 11(5): 402-411. https://doi.org/10.52403/ijrr.20240547
[8] Ghahramani, S., Kasraei, H., Shahabi, S., Lankarani, K.B. (2020). Facilitating factors and barriers of women's cancer screening in Iran: A systematic review. International Journal of Preventive Medicine, 11(1): 199. https://doi.org/10.4103/ijpvm.IJPVM_509_18
[9] Hijrah, H., Usman, A.N., Sanusi Baso, Y., Syarif, S., Ahmad, M., Nulandari, Z. (2024). Influence of variables on breast self-examination: Potential barrier or enhancement of breast cancer prevention. Breast Disease, 43(1): 145-155. https://doi.org/10.3233/bd-249001
[10] Inagaki, J., Rodriguez, V., Bodey, G.P. (1974). Causes of death in cancer patients. Cancer, 33(2): 568-573. https://doi.org/10.1002/1097-0142(197402)33:2<568::aid-cncr2820330236>3.0.co;2-2
[11] Inayah, H.K., Netty, N., Widyarni, A., Octaviana, E.S.L. (2023). Pelatihan pemeriksaan payudara sendiri (SADARI) untuk deteksi dini kanker payudara di gang purnawirawan RT 2 kelurahan pelambuan banjarmasin. Jurnal Abdimas Kesehatan (JAK), 5(1): 18-23. https://doi.org/10.36565/jak.v5i1.378
[12] Jackline, W., Charles, M., John, O., Edward, M. (2021). Influence of knowledge, attitudes and practices on breast cancer early detection. International Journal of Medical Science and Clinical Invention, 8(11): 5753-5760. https://doi.org/10.18535/ijmsci/v8i011.03
[13] Kawasaki, Y., Hirai, K., Nii, M., Kizawa, Y., Uchinuno, A. (2024). Factors involved in shared decision-making regarding treatment selection by patients with cancer. Cancer Diagnosis & Prognosis, 4(1): 57-65. https://doi.org/10.21873/cdp.10286
[14] Kurniawati, H. (2023). Deteksi dini kanker payudara dengan sadari dan sadarnis. BAKTIMU J. Pengabdian Kepada Masyarakat, 3(2): 55-64. https://doi.org/10.37874/bm.v3i2.821
[15] Lamont, E.B., Christakis, N.A. (2001). Prognostic disclosure to patients with cancer near the end of life. Annals of Internal Medicine, 134(12): 1096-1105. https://doi.org/10.7326/0003-4819-134-12-200106190-00009
[16] Li, X., Sun, S., Tang, T., Lu, J., Zhang, L., Yin, J., Geng, Q., Wu, Y. (2023). Construction of a knowledge graph for breast cancer diagnosis based on Chinese electronic medical records: Development and usability study. BMC Medical Informatics and Decision Making, 23(1): 210. https://doi.org/10.1186/s12911-023-02322-0
[17] Lubis, S., Nasution, N.F. (2024). Utilizing digital literacy in anticipating the political education gap for women. Journal Elections and Political Parties, 1(2): 9-16. https://jurnal.literasipublisher.co.id/index.php/jepp/article/view/61
[18] Maghfiroh, A., Jati, R.P., Ayuningtyas, F. (2023). Edukasi pentingnya sadari (Pemeriksaan payudara sendiri) dan sadanis (pemeriksaan payudara klinis) untuk deteksi dini kanker payudara. Jurnal Pengabdian Masyarakat Kesosi, 6(2): 36-43. https://doi.org/10.57213/abdimas.v6i2.178
[19] Marhaeni, G.A., Suindri, N.N., Arneni, N.P.G., Habibah, N., Dewi, N.N.A. (2024). Edukasi tentang kanker payudara meningkatkan perilaku pemeriksaan payudara sendiri (sadari) pada remaja putri. Jurnal Pengabdian Masyarakat Sasambo, 5(2): 136-141. https://doi.org/10.32807/jpms.v5i2.1438
[20] McNeill, L.H., Wu, I.H., Cho, D., Lu, Q., Escoto, K., Harris, C. (2020). Community outreach and engagement strategies to address breast cancer disparities. Current Breast Cancer Reports, 12: 209-215. https://doi.org/10.1007/s12609-020-00374-z
[21] Tulus, T., Sutarman, S., Syahputra, M.R., Marpaung, T.J. (2024). Computational analysis of stability of wave propagation against submerged permeable breakwater using hybrid finite element method. In AIP Conference Proceedings, 3029(1): 040022. https://doi.org/10.1063/5.0192099
[22] Sinulingga, S., Nasution, V.A., Meutia, A., Indra, S., Kesuma, F.T., Marpaung, J.L. (2024). Automated and measured managerial systems in the management of independent tourism villages: A case study of parsingguran II village, polung subdistrict, Humbang Hasundutan regency. Jurnal Pengabdian Masyarakat Bestari, 3: 527-540. https://doi.org/10.55927/jpmb.v3i9.11334
[23] Hasibuan, C.D., Siahaan, D.A.S., Manurung, A., Marpaung, J.L. (2024). Stability analysis of spread of infectious diseases COVID-19 using SEIAR-V1V2Q model for asymptomatic condition with runge-kutta order 4. Mathematical Modelling of Engineering Problems, 11(5): 1348–1354. https://doi.org/10.18280/mmep.110526
[24] Sinulingga, S., Marpaung, J.L., Sibarani, H.S., Amalia, A., Kumalasari, F. (2024). Sustainable tourism development in Lake Toba: A comprehensive analysis of economic, environmental, and cultural impacts. International Journal of Sustainable Development & Planning, 19(8): 2907-2917. https://doi.org/10.18280/ijsdp.190809
[25] Tulus, T., Sy, S., Sugeng, K.A., Simanjuntak, R., Marpaung, J.L. (2024). Improving data security with the utilization of matrix columnar transposition techniques. In E3S Web of Conferences, 501: 02004. https://doi.org/10.1051/e3sconf/202450102004
[26] Sofiyah, F.R., Dilham, A., Lubis, A.S., Marpaung, J.L., Lubis, D. (2024). The impact of artificial intelligence chatbot implementation on customer satisfaction in padangsidimpuan: Study with structural equation modelling approach. Mathematical Modelling of Engineering Problems, 11(8): 2127-2135. https://doi.org/10.18280/mmep.110814
[27] Sofiyah, F.R., Dilham, A., Hutagalung, A.Q., Yulinda, Y., Lubis, A.S., Marpaung, J.L. (2024). The chatbot artificial intelligence as the alternative customer services strategic to improve the customer relationship management in real-time responses. International Journal of Economics and Business Research, 27(5): 45-58. https://doi.org/10.1504/IJEBR.2024.139810
[28] Silalahi, A.S., Lubis, A.S., Gultom, P. (2024). Impacts of PT Pertamina geothermal sibayak’s exploration on economic, social, and environmental aspects: A case study in Semangat Gunung Village, Karo District. International Journal of Energy Production and Management, 9(3): 161-170. https://doi.org/10.18280/ijepm.090305
[29] Tulus, Rasani, M.R., Rahman, Md. M., Suriati., Marpaung, T.J., Siringoringo, Y.B.P., Marpaung, J.L. (2024). Biomedical simulation of non-newtonian fluid dynamics in cardiovascular systems: A finite volume method approach to pulsatile flow and atherosclerosis analysis. International Journal of Energy Production and Management, 9(4): 275-285. https://doi.org/10.18280/ijepm.090408
[30] Gultom, P., Marpaung, J.L., Weber, G.W., Sentosa, I., Sinulingga, S., Putra, P.S.E., Agung, V.R. (2024). Optimizing the selection of the sustainable micro, small, and medium-sized enterprises development center using a multi-criteria approach for regional development. Mathematical Modelling of Engineering Problems, 11(11): 2977-2987. https://doi.org/10.18280/mmep.111110
[31] Syahputra, M.R., Marpaung, T.J., Marpaung, J.L. (2024). Mathematical study simulating hydroelectric power as a renewable green energy alternative. Mathematical Modelling of Engineering Problems, 11(7): 1877-1884. https://doi.org/10.18280/mmep.110717
[32] Gultom, P., Nababan, E.S.M., Marpaung, J.L., Agung, V.R. (2024). Balancing sustainability and decision maker preferences in regional development location selection: a multi-criteria approach using AHP and fuzzy goal programming. Mathematical Modelling of Engineering Problems, 11(7): 1802-1812. https://doi.org/10.18280/mmep.110710