Temporal Trend of PM2.5 and the Associated Risk to Human Health in the Lima Metropolitan Area

Justiniano Palomino Quispe![]() | Domingo Zapana Diaz
| Domingo Zapana Diaz![]() | Daniel Alvarez-Tolentino
| Daniel Alvarez-Tolentino![]() | Alex Huaman De La Cruz*
| Alex Huaman De La Cruz*![]() | Ide Unchupaico Payano
| Ide Unchupaico Payano![]() | Andres Camargo Caysahuana
| Andres Camargo Caysahuana![]() | Roger Aguilar Rojas
| Roger Aguilar Rojas![]() | Ronald Panduro Durand
| Ronald Panduro Durand![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The objective of this study was to evaluate the human health risk associated with PM2.5 exposure in residents of the Metropolitan area of Lima (MAL), Peru, for a best-case scenario and a worst-case scenario based on the monthly average of PM2.5 and 90th percentile of PM2.5 concentration, respectively. Hourly concentrations of PM2.5 between 2014 and 2023 corresponding to five monitoring stations were provided by the National Meteorology and Hydrology Service (SENAMHI). Air quality was assessed using the air quality index (AQI). The hazard quotient to evaluate the risk to human health was calculated using the annual limit value established by the European Union (EU, 25 µg/m3) and World Health Organization (WHO, 10 µg/m3) because there is no toxicity value for PM2.5. Annual average PM2.5 concentration ranged from 19.5 µg/m3 to 35.8 µg/m3 with some years below the annual limit established by the EU, while all years exceeded the WHO limits and the Peruvian legislation (ECA (25 µg/m3), except 2015, 2020, and 2023). Overall, monthly PM2.5 concentrations were higher in winter versus summer seasons. AQI showed that Lima is classified from moderate to hazardous, indicating that air quality is unhealthy for sensitive population groups. In the best-case scenario and worst-case scenario based on EU, both show greater potential chronic non-carcinogenic risk in the winter months than in the summer months and were identified every year (except 2020), mainly in the winter seasons, which indicates a permanent exposure and risk to the health of the population of Lima, respectively, while WHO AQG for the best-case scenario indicated a potential chronic non-carcinogenic health risk in most months of the year, while for the worst-case scenario, were higher in winter months than in the summer months, showing a constant behavior, indicating that there is a non-carcinogenic risk during almost the entire period. No decrease in HQ values would suggest the presence of air quality improvement measures.
air quality, PM2.5, human health risk, Metropolitan area, Lima
Air pollution, especially that generated by particulate matter (PM), is a major problem in Europe and Latin America. PM is a complex mixture of solids and aerosols containing metals and metalloids, carbonaceous species (elemental carbon and organic carbon), and ionic species [1]. The PM is classified according to their aerodynamic diameter in coarse or “inhalable” particles (PM10, ≤ 10 µm (microns) in diameter) and fine or “respirable” particles (PM2.5, ≤ 2.5 (microns) µm in diameter) [2]. PM2.5 is widely monitored because its short or large exposure time can have adverse health impacts and environmental effects (visibility impairment, environmental damage, and materials damage). The health impacts of PM exposure largely depend on its size, shape, source of emission, and chemical composition. However, exposure to PM2.5 compared to PM10 is more dangerous due to its ability to penetrate directly to the lung and even enter directly into the bloodstream, which may generate decreasing in lung function, exacerbated asthma, intensification of symptoms of diseases related to the circulatory and respiratory systems, and even promote different types of cancer (lung, throat, and laryngeal). For example, Vu et al. [3] reported 103,974 cases of asthma from 2010 to 2016 found in 39 districts of Lima, which were associated with exposure to PM2.5. Likewise, urban populations are particularly susceptible to PM2.5 by factors such as high population density, traffic emissions, limited green spaces, vulnerable groups, and climate conditions [4].
According to WHO, around 7 million people die every year from exposure to fine particles, and 90% of these deaths occur in low- and middle-income countries [5]. Peru´s urbanization rate has been steadily increasing with approximately 79% of the population living in urban areas, which demographic trends are migration, rural depopulation, economic disparity, and increased pressure on housing and infrastructure. In the Metropolitan area of Lima, the Urban Transport Authority of Lima and Callao (ATU) revealed that the vehicular fleet is responsible for 58% of air pollution in this area, with 85% of the vehicular fleet using diesel as fuel, while a small proportion is powered by natural gas and electricity. Besides, 24% of these vehicular fleets are more than 20 years old, being necessary for renovation [6]. Faced with all this information, the population is the most affected because daily it is exposed to different contaminations and concentrations of PM2.5.
There is significant scientific evidence that fine particulate matter (PM2.5) has a greater negative impact on human health. Several studies have reported levels of PM2.5 in different cities around the world [7-9]. Human health risks related to PM2.5 exposure and its toxic elements also were carried out in several cities [10, 11]. Most of these studies showed that even though PM2.5 concentrations stayed within the set air quality standards, the health effects of air pollution exposure are crucial for evaluating human health risks and for managing and reducing urban air pollution.
This study aimed to assess the health risks linked to PM2.5 for residents of the Metropolitan Area of Lima (MAL), Peru. The Air Quality Index (AQI) was used to gather information on air quality and the temporal variations in PM2.5 levels in MAL from 2014 to 2023, to identify periods when air quality became a concern for the local population. Besides, the health risk assessment (HRA) was estimated using the EU and WHO recommended values. The HRA offers information on the risk or danger that a place represents to human health. The data collected can assist local governments in effectively managing air quality and guide decision-makers in developing and implementing improved strategies and regulations to enhance air quality and reduce impacts on human health.
2.1 Study area
The study was carried out in the Lima Metropolitan Area (AML) or Metropolitan Lima (75º30'18" S and 77º53'02" W), which includes the districts of Lima Province and the Constitutional Province of Callao. It is the largest, most extensive, and most populated urban area in Peru and one of the five largest megacities in Latin America, with a territorial area of 2683 km2 and an estimated population of 11.3 million inhabitants (population density of Lima 3620 inhabitants/km2 and Callao 8050 inhabitants/km2) in 2023 [12]. According to the environmental quality bulletin of the Urban Transport Authority (ATU), the AML owns 68.6% (more than 2 million vehicles) of Peru's light and heavy vehicle fleet [13], which runs mainly on petroleum, its derivatives, and natural gas liquids such as diesel (about 46% of total liquid fuel consumption), LPG (24%) and gasoline/diesel (20%) [14]. Fixed sources of air pollution in AML include chemical, metallurgical, steel, textile, non-metallic mining, and paper and printing industries. The climate of the AML is subtropical, with an average annual temperature of 19 °C, relative humidity of 80% average annual precipitation of 10 mm per year, and cloudy skies almost all year.
2.2 PM2.5 air quality data
The AML has a network of real-time air quality monitoring stations installed in 10 districts: Ate Vitarte (ATE), Huachipa (HUA), San Juan de Lurigancho (SJL), Santa Anita (STA), Puente Piedra (PP), San Borja (SBJ), Campo de Marte (CM), Carabayllo (CRB), Villa María del Triunfo (VMT), and San Martin de Porres (SMP) which are in charge of the National Meteorology and Hydrology Service (SEHAMHI). These stations are installed in urban environments and report the concentrations of PM10, PM2.5, O3, and NO2 every hour. PM10 data (period 2010-2023) from five monitoring stations (SBJ, STA, VMT, SJL, and CRB) were provided by SENAMHI (Table 1). (Information related to each monitoring station, instrument, and principle used is presented in the supplementary material). PM2.5 data (period 2014-2023) from five monitoring stations (SBJ, STA, VMT, SJL, and CRB) were provided by SENAMHI (Figure 1 and Table 1).
Figure 1. Map of localization of AML and the monitoring stations network
Table 1. Localization of air quality monitoring station from the SENAMHI
|
Monitoring Station |
Latitude and Longitude |
Population [15] |
Superficial Area (km2) |
Elevation m.a.s.l |
|
San Borja (SBJ) |
12º6´31.1''S, 77º0'27.9''W |
133328 |
11.5 |
128 |
|
Carabayllo (CRB) |
11º54´7.9''S, 77º2'1.1''W |
426895 |
384.89 |
179 |
|
San Juan Lurigancho (SJL) |
12º1'8.0''S, 76º59'57.4''W |
1240489 |
131.25 |
240 |
|
Santa Anita (STA) |
12º2´35.9''S, 76º58'17.0''W |
232739 |
10.69 |
253 |
|
Villa María del Triunfo (VMT) |
12º9´59.0''S, 77º55'12.0'' |
459010 |
70.57 |
292 |
2.3 Air Quality Index (AQI)
The AQI is an indicator that provides related information on the air quality of a certain area. It is as a rule utilized to get data on the everyday discussion quality of each observing station, in this inquiry about it was connected to analyzing the month-to-month inconstancy and discovering multi-year patterns utilizing the five checking stations introduced within the AML, considering that only one station isn't an agent and would not reflect well the varieties of PM2.5 inside the AML. Thus, the daily AQI was calculated using the mean PM2.5 concentration of each monitoring station and the daily limit value of the EU (25 μg/m3) using Eq. (1) [16].
AQI=PM2.5concentrationthreshold concentration×100 (1)
The AQI has six scales ranging from 0 to 500, and are categorized as good (0-50), moderate (51-100), harmful to health for sensitive groups (101-150), harmful to health (151-200), very harmful to health (201-300), and dangerous (greater than 300). AQI values less than 100 are considered satisfactory, while values above 100 indicate air pollution and health risks [17].
2.4 Human health risk assessment
This assessment makes it possible to calculate and estimate the hazard or risk that a place (residence, work area, or site) represents to human health [18]. Thus, the risk of PM2.5 exposure to human health was estimated using the hazard quotient (HQ) (Eq. (2)).
HQ=EC/TV (2)
where, TV is the toxicity value and EC refers to the exposure concentration of PM2.5 (μg/m3) which is calculated through Eq. (3) [19]. As no toxicity esteem for PM2.5 was found within the scientific literature, TV expected the EU yearly constraint value of 20 μg/m3 (HQ1) and WHO AQG of 10 μg/m3 (HQ2).
EC=(CA×ET×EF×ED)/AT (3)
where CA is the monthly average concentration of PM2.5 for the best-case scenario, while the monthly 90 quartile for the worst-case scenario, ET is the exposure time (hours/day), EF exposure frequency (days/year), ED is the duration of exposure (year), and AT is the average time obtained by multiplying ED × 365 days/year× 24 h/day. To calculate the exposure of the residents, it was considered ET to take a value of 24 h/day, EF was 350 days/year, and ED was 30 years for adults [19].
Non-carcinogenic risk refers to all adverse health effects except cancer caused by exposure. The security reference level for HQ is 1. Based on this, exposure to PM2.5 could induce chronic non-carcinogenic effects if HQ ˃ 1, and no non-carcinogenic risk if HQ ˂ 1 [20].
2.5 Statistical analysis
The PM2.5 values obtained for the period 2014-2023 from each monitoring station were treated independently and jointly (representing the AML) to find their basic statistics (minimum, maximum, average, standard deviation, percentiles (10, 50, and 90), and number of days that exceeded the established limits). All statistical and graphical treatments were carried out in the free software CRAN R version 4.2.1 [21] using the open air [22] and GGPLOT2 [23] packages.
3.1 Air quality
The expressive insights of PM2.5 recorded within the Lima Metropolitan Range between 2014-2023, which were calculated based on everyday values from the five monitoring stations, are displayed in Table 2. From Table 2 it is possible to see that the annual average varies from 19.5 to 35.8 μg/m3, values that are above the annual limit value set by EU legislation and Peruvian regulations (25 μg/m3) except for the years 2015, 2020 and 2023. It is also noted that all the annual average values exceeded the AQS established by the WHO (10 μg/m3) in all years.
In 2018, the highest annual daily value recorded was 157 μg/m3, and the lowest annual maximum was measured in 2023 at 52.4 μg/m3. All the maximum annual values showed a temporal behavior with two periods of high peaks: before (2018) and after (2022) the COVID-19 pandemic. A similar behavior was observed based on the number of days with daily values greater than 25 μg/m3 and in the 10th, 50th, and 90th percentiles, with the peak period being 2022 showed the highest number of infractions (1262) that exceeded the PM2.5 limit value, as well as the highest percentile values.
In the year of the highest violation of annual PM2.5 limits, 329 occurred in SJL, 272 in VMT, and 268 in STA. The year with the lowest number of infractions was 2020 when sanitary measures were applied to control and prevent the increase in infections due to the COVID-19 pandemic with the suspension of industrial activities and transport, producing an improvement in air quality in many cities around the world [24] where Lima was no exception [25].
Table 2. Statistics descriptive of the annual PM2.5 (2014-2023) concentrations (µg/m3) in the Metropolitan area of Lima
|
Year |
N |
Mean ± CI (S.D.) |
[Min, Max] |
10th Percentile |
50th Percentile |
90th Percentile |
Day with PM2.5 >25 µg/m3 |
|
2014 |
1375 |
29.5 ± 0.53 (9.95) |
[9.24, 67.2] |
17.56 |
28.35 |
41.83 |
419 |
|
2015 |
1825 |
24.1 ± 0.37 (8.05) |
[9.70, 70.2] |
14.54 |
23.14 |
34.50 |
626 |
|
2016 |
1830 |
27.8 ± 0.51 (11.1) |
[8.24, 84.8] |
15.42 |
26.09 |
42.33 |
774 |
|
2017 |
1825 |
26.3 ± 0.48 (10.5) |
[8.22, 119] |
13.29 |
25.90 |
39.18 |
725 |
|
2018 |
1825 |
25.6 ± 0.51 (11.1) |
[6.86, 157] |
13.79 |
23.99 |
38.14 |
551 |
|
2019 |
1825 |
28.7 ± 0.72 (15.6) |
[4.89, 148] |
13.03 |
26.87 |
45.49 |
323 |
|
2020 |
1830 |
19.5 ± 0.35 (7.53) |
[3.74, 53.4] |
10.95 |
18.58 |
29.29 |
172 |
|
2021 |
1825 |
29.3 ± 0.53 (11.6) |
[3.71, 71.6] |
15.13 |
27.82 |
44.45 |
354 |
|
2022 |
1825 |
35.8 ± 0.71 (15.4) |
[6.74, 99.9] |
18.01 |
32.75 |
57.20 |
1262 |
|
2023 |
1505 |
23.7 ± 0.37 (7.37) |
[6.72, 52.4] |
14.90 |
22.89 |
33.50 |
474 |
S.D.= standard deviation
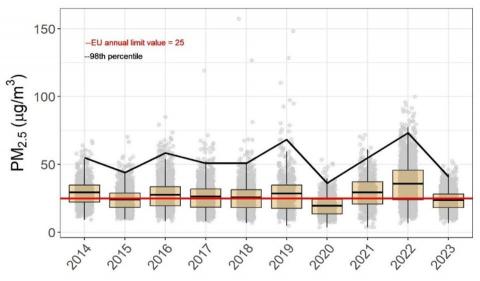
Figure 2 shows a variable trend in the annual average of PM2.5, first a slight increase is noted from 2014 to 2019, then it is observed that it decreases in 2020, but that it increases again until 2022, the year where the highest average value and violations of the limit values of the EU and Peruvian ECA were recorded. The difference between the average and the annual median of PM2.5 increased from 2014 to 2023, increasing the number of days with high PM2.5 values. 2023 shows a decrease in violations. These results coincide with those reported by Valdivia [26] and Ordóñez-Aquino and Gonzales [27], who highlight that PM2.5 is one of the problem pollutants for the city of Lima.
Figure 2. Annual evolution of PM2.5 between 2014 and 2023 inside the Metropolitan area of Lima. Line solid = threshold limit value of EU = 25 µg/m3 and curve = 98th percentile
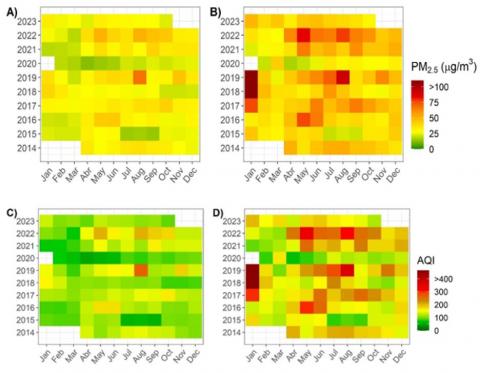
Figure 3. Temporal variation of (A) the average of PM2.5 concentration (B) 90th percentile of PM2.5 (µg/m3) concentration (C) the average of air quality index (AQI) and (D) 90th percentile of air quality index (AQI) in the MAL for 2014 - 2023
Monthly PM2.5 concentrations (Figure 3(A)) were highest in August (48.2±27.7 μg/m3) of 2019, as well as in May (48.4±6.8 μg/m3) and August (48±9.1 μg/m3) of 2022, the lowest recorded in April (13.9±4.3 μg/m3) of 2020. The peak values were recorded in May and August, with a similar behavior in all the stations where most of the infractions occurred between May and September. In general, monthly PM2.5 concentrations were higher in winter seasons than in summer. A possible explanation for the high levels of PM2.5 in winter could be the accumulation of PM in the lower atmosphere due to the reduction in the thickness of the mixing layer, determined by the humid meteorological conditions of a coastal city [28].
The monthly PM2.5 98th percentile (Figure 3(B)) exhibited consistent patterns across the years, except in 2020, indicating ongoing emissions from a significant source in the city, namely the vehicle fleet. Between May and August, the highest values for the 98th percentile were recorded, with 139 μg/m3 and 136 μg/m3 being the most extreme values in 2018 and 2019, respectively. The average monthly AQI (Figure 3(C)) ranged from 56 (April 2020) to 271 (January 2018), indicating that air quality in Lima is classified from moderate to unhealthy. The range for the 98th percentile (Figure 3(D)) was from 58 (April 2020) to 557 (January 2018), showing that in most months, air quality reaches levels that are hazardous and unsafe for more susceptible population segments.
The findings suggest that air pollution continues to be a significant issue in Lima, despite improvements in air quality management. This reality that AML continues to have a critical air quality was also reported in references [26, 29-31].
It is clear that moderate to hazardous air quality is largely attributed to the vehicle fleet [26, 32], responsible for 58% of air pollution. This situation is aggravated by the fact that a significant percentage of vehicles, both in regular transport and in taxi service, are more than fifteen years old, while others are even older, and that a large part of them operate mainly using fossil fuels such as oil, diesel, gasoline, LPG and CNG. In addition, the presence of 25% of vehicles that are more than 20 years old, and that still circulate within the Metropolitan Area of Lima, makes it necessary to take measures and renew the vehicle fleet or take these old cars out of circulation [26]. A similar conclusion was reached by Mousavinezhad et al. [33] who stated that air pollution is largely attributed to the transportation industry.
Traffic congestion is also a relevant factor in this problem, as shown by the TomTom Traffic Index 2022, which places our capital as the eighth city in the world with the worst traffic congestion and the first on the continent [34]. Wang et al. [35] maintain that vehicle emissions are regarded as the primary contributor to air pollution of particulate matter, which is related to adverse health impacts. This congestion not only contributes to the emission of air pollutants but also negatively affects the quality of life of the inhabitants. It is imperative to address these issues from a comprehensive strategy that includes both regulatory and incentive measures for the renewal of the vehicle fleet, the promotion of cleaner and more efficient technologies, as well as the improvement of public transport infrastructure, and the implementation of more effective traffic management policies. In addition, it is essential to foster research and innovation in the automotive sector and urban mobility to find long-term sustainable solutions that reduce air pollution and improve the quality of life in our cities. The cost of particulate matter pollution associated with vehicular transport ranged from 0.21-0.29% of the GDP of the city of Metropolitan Lima [29].
3.2 Human health risk assessment
During the study periods, the exposure concentrations (ECs) were determined by averaging the monthly PM2.5 concentrations. These values varied from 12.8 μg/m3 in May 2020 to 133.6 μg/m3 in January 2019. Additionally, the ECs calculated based on the 98th percentile monthly concentration ranged from 17.9 μg/m3 in April 2020 to 150.1 μg/m3 in January 2018. These data show an increase in exposure concentrations from May to September.
The chronic non-carcinogenic HQ1 was calculated using the EU limit value for the optimal residential scenario and ranged from 0.1 to 6.7 in every year under investigation, suggesting a potential chronic non-carcinogenic health hazard throughout the study period, except for 2020 and specific months in 2015.
In the same way, HQ1 values reached higher levels (0.2-7.54) in the worst-case scenario, and annual peaks exceeding the safety benchmark were observed every month. In Figure 4(A), the best-case scenario depicts greater potential for chronic non-carcinogenic risk during the winter months compared to the summer months. Conversely, Figure 4(B), the worst-case scenario, also shows a similar trend of higher risk in the winter months than in the summer months. From the beginning of PM2.5 monitoring in 2014, the best-case scenario involved the identification of non-carcinogenic health risks. Similarly, in the worst-case scenario, non-carcinogenic health risks were identified every year (except 2020) in both exposure scenarios, predominantly during winter seasons. This suggests consistent exposure and risk to the health of Lima's population. Sanchéz-Ccoyllo et al. [36] estimated long-term health effects of PM2.5 using the WHO´s AirQ+ model in the MAL and reported that cases of all-cause mortality, on average, could have been avoided if PM2.5 concentrations would have decreased from 26.53 μg/m3 to 23.9 μg/m3. Likewise, Tapia et al. [37] concluded that PM2.5 is associated with daily cardiorespiratory mortality in Lima, especially for older people.
Figure 4. Temporal variation of Hazard quotient (HQ) computed based on EU limit values for best-case (A) and worst-case (B) scenarios and computed based on World Health Organization air quality guideline for best-case (C) and worst-case (D) scenarios in the Metropolitan area of Lima for 2014 - 2023
Based on the WHO AQG, the chronic non-carcinogenic HQ2 calculated for the best case showed a range of 0.3 to 13.4 in all years studied, suggesting a potential chronic noncarcinogenic health risk for most months of the year. In the worst-case scenario, HQ2 values were higher (0.4-15.1), surpassing the safety benchmark in every month. HQ2 values monthly, as depicted in Figure 4C for the best-case scenario and Figure 4D for the worst-case scenario, exhibited higher values during winter months compared to summer months. This consistent pattern suggests the presence of a non-carcinogenic risk throughout most of the period.
Figure 5 depicts the variations in human health risk measurements of air quality monitoring stations in Lima from 2014 to 2023 for both the best-case and worst-case scenarios. When considering HQ1 values based on EU limit values, it is evident that all monitoring stations, except for SBJ, surpassed the threshold. This indicates a potential health risk in all urban stations, with the highest risk observed in SJL and STA.
In urban stations SJL and STA, the health risk is elevated due to traffic and industrial surroundings in the case of HQ2. The same trend is noticed in the worst-case scenario for both HQ1 and HQ2, with all seasons exceeding 1, signifying a continual potential non-carcinogenic risk in the population, particularly among the most vulnerable. These results complement those reported in references [38-40].
Figure 5. Variation of hazard quotient (HQ) computed based on EU limit values (a) and World Health Organization air quality guidelines (b) between the air quality monitoring stations from the Metropolitan area of Lima for 2010 - 2023
The elevated HQ values indicate that even though PM2.5 levels in the environment are below legal limits, they are still likely to cause different long-term health issues. This shows that the health risks from air pollution exposure in Lima are continuous.
This risk is of particular concern due to the possible induction of various chronic diseases [41].
Considering the combined impacts of PM2.5 and other air pollutants is essential, as it may raise the risk of experiencing long-term non-cancerous negative effects. These results highlight the need to review and potentially readjust legislative thresholds to ensure adequate protection of public health from exposure to air pollutants [27]. In addition, they underscore the importance of implementing preventive and mitigation measures to reduce the risks associated with air pollution, even when levels appear to be within acceptable limits.
The study's limitations arise from its sole concentration on PM2.5, neglecting concurrent exposure to other air pollutants, resulting in an underestimated risk. Furthermore, the non-carcinogenic health risk assessment relied on assumptions concerning the timing, frequency, and duration of exposure, which are not tailored to the population under study and do not account for individual behavioral differences. The air quality monitoring stations were assumed to provide representative average daily PM2.5 concentrations for the entire city. Although there are limitations, the findings help improve our comprehension of the potential health hazards associated with human exposure to PM2.5 in urban settings. This offers valuable insights to enhance air quality management in Lima involving various stakeholders.
Air quality management and risk reduction strategies for PM2.5 focus on reducing emissions to realize emissions control, public transportation improvements, urban planning, regulatory enforcement, air quality monitoring, and public awareness campaigns, among others.
The average annual level of PM2.5 in the Metropolitan area of Lima exceeds the annual limit value set by EU legislation, WHO limits, and Peruvian regulations, except for three years (2015, 2020, and 2023). Overall, monthly PM2.5 concentrations were higher in winter versus summer seasons. The average monthly AQI ranged from moderate to hazardous, which indicates that air quality is unhealthy for the population in general. The WHO GCA indicates a permanent chronic risk to non-carcinogenic health in all years, being highest from May to September. There is no downward trend in HQ values to indicate the existence of air quality improvement measures; However, the implementation of mitigation measures by those policymakers responsible such as the Ministry of Environment, Metropolitan Municipality of Lima, and public Health agencies addressing together to tackle PM2.5 pollution in Lima´s urban areas.
The authors thank the SENAMHI for providing meteorological and pollution data.
[1] Zhang, G., Ding, C., Jiang, X., Pan, G., Wei, X., Sun, Y. (2020). Chemical compositions and sources contribution of atmospheric particles at a typical steel industrial urban site. Scientific Reports, 10(1): 7654. https://doi.org/10.1038/s41598-020-64519-x
[2] EPA. (2011). Particulate Matter Emissions. Washington, USA. https://www.epa.gov/pm-pollution.
[3] Vu, B.N., Tapia, V., Ebelt, S., Gonzales, G.F., Liu, Y., Steenland, K. (2021). The association between asthma emergency department visits and satellite-derived PM2. 5 in Lima, Peru. Environmental Research, 199: 111226. https://doi.org/10.1016/j.envres.2021.111226
[4] Łowicki, D. (2019). Landscape pattern as an indicator of urban air pollution of particulate matter in Poland. Ecological Indicators, 97: 17-24. https://doi.org/10.1016/j.ecolind.2018.09.050
[5] WHO World Health Organization. http://www.who.int/news-room/headlines/02-05-2018-9-out-of-10-people-worldwide-breathe-polluted-air-but-more-countries-are-taking-action.
[6] Jauregui-Fung, F., Kenworthy, J., Almaaroufi, S., Pulido-Castro, N., Pereira, S., Golda-Pongratz, K. (2019). Anatomy of an informal transit city: Mobility analysis of the metropolitan area of Lima. Urban Science, 3(3): 67. https://doi.org/10.3390/urbansci3030067
[7] Pereira, G.M., Oraggio, B., Teinilä, K., Custódio, D., et al. (2019). A comparative chemical study of PM 10 in three Latin American cities: Lima, Medellín, and Sao Paulo. Air Quality, Atmosphere & Health, 12: 1141-1152. https://doi.org/10.1007/s11869-019-00735-3
[8] Kassomenos, P.A., Vardoulakis, S., Chaloulakou, A., Paschalidou, A.K., Grivas, G., Borge, R., Lumbreras, J. (2014). Study of PM10 and PM2.5 levels in three European cities: Analysis of intra and inter urban variations. Atmospheric Environment, 87: 153-163. https://doi.org/10.1016/j.atmosenv.2014.01.004
[9] Kunecki, P., Franus, W., Wdowin, M. (2020). Statistical study and physicochemical characterization of particulate matter in the context of Kraków, Poland. Atmospheric Pollution Research, 11(3): 520-530. https://doi.org/10.1016/j.apr.2019.12.001
[10] Wang, Y., Wu, Y., Zheng, F., Zhang, T., et al. (2022). Health threat of PM2. 5-bound trace elements exposure on asthma hospital admission: A time-stratified case-crossover study. Environment International, 170: 107604. https://doi.org/10.1016/j.envint.2022.107604
[11] Curtis, L. (2021). PM2.5, NO2, wildfires, and other environmental exposures are linked to higher Covid 19 incidence, severity, and death rates. Environmental Science and Pollution Research, 28(39): 54429-54447. https://doi.org/10.1007/s11356-021-15556-0
[12] INEI población peruana alcanzó los 33 millones 726 mil personas en el año 2023. https://m.inei.gob.pe/prensa/noticias/poblacion-peruana-alcanzo-los-33-millones-726-mil-personas-en-el-ano-2023-14470/.
[13] MTC parque automotor nacional estimado por clase vehicular, según departamento: 2011-2022. https://www.gob.pe/institucion/mtc/informes-publicaciones/344892-estadistica-servicios-de-transporte-terrestre-por-carretera-parque-automotor.
[14] Indecopi. Informe de Lanzamiento del estudio de mercado sobre combustible liquidos y gas licuado de petróleo en el Perú [Internet]. Lima, Perú. (2022). https://www.gob.pe/institucion/indecopi/informes-publicaciones/5476531-informe-de-lanzamiento-del-estudio-de-mercado-sobre-combustibles-liquidos-y-gas-licuado-de-petroleo-en-el-peru.
[15] INEI. Perú: Proyecciones de población, según departamento, provincia y distrito, 2018-2022. https://cdn.www.gob.pe/uploads/document/file/3624028/Perú%3A Proyecciones de Población Total según Departamento%2C Provincia y Distrito%2C 2018-2022.pdf?v=1663081335.
[16] Levei, L., Hoaghia, M.A., Roman, M., Marmureanu, L., et al. (2020). Temporal trend of PM10 and associated human health risk over the past decade in Cluj-Napoca city, Romania. Applied Sciences, 10(15): 5331. https://doi.org/10.3390/app10155331
[17] Mohan, M., Kandya, A. (2007). An analysis of the annual and seasonal trends of air quality index of Delhi. Environmental Monitoring and Assessment, 131: 267-277. https://doi.org/10.1007/s10661-006-9474-4
[18] EPA. (2007). ¿Qué es la evaluación del riesgo para la salud humana? https://semspub.epa.gov/work/HQ/176357.pdf.
[19] EPA-540-R-070-002. (2009). Risk assessment guidance for superfund volume I: Human health evaluation manual (Part F, supplemental guidance for inhalation risk assessment). https://www.epa.gov/sites/default/files/2015-09/documents/partf_200901_final.pdf.
[20] Miclean, M., Cadar, O., Levei, E.A., Roman, R., Ozunu, A., Levei, L. (2019). Metal (Pb, Cu, Cd, and Zn) transfer along food chain and health risk assessment through raw milk consumption from free-range cows. International Journal of Environmental Research and Public Health, 16(21): 4064. https://doi.org/10.3390/ijerph16214064
[21] The R Project for Statistical Computing. https://www.r-project.org/.
[22] Carslaw, D. (2019). The openair manual open-source tools for analysing air pollution data [Internet]. Environmental Modelling & Software. Nueva York, USA: King College London. https://davidcarslaw.com/files/openairmanual.pdf.
[23] Wickham, H., Chang, W., Henry, L., Pedersen, T.L., Wilke, C., Woo, K. (2023). Create elegant data visualisations using the grammar of graphics [Internet]. CRAN. https://ggplot2.tidyverse.org/reference/ggplot2-package.html.
[24] Rodríguez-Urrego, D., Rodríguez-Urrego, L. (2020). Air quality during the COVID-19: PM2.5 analysis in the 50 most polluted capital cities in the world. Environmental Pollution, 266: 115042. https://doi.org/10.1016/j.envpol.2020.115042
[25] Rojas, J.P., Urdanivia, F.R., Garay, R.A., García, A.J., Enciso, C. (2021). Effects of COVID-19 pandemic control measures on air pollution in Lima metropolitan area, Peru in South America. Air Quality, Atmosphere & Health, 14: 925-933. https://doi.org/10.1007/s11869-021-00990-3
[26] Valdivia, S. (2016). Spatial and temporal analysis of the air quality determined by particulate matter PM10 and PM2.5 in metropolitan Lima. Anales Cientificos, 77(2): 273-283. https://revistas.lamolina.edu.pe/index.php/acu/article/view/699/pdf_37.
[27] Ordoñez-Aquino, C., Gonzales, G.F. (2023). Calidad del aire en Perú no se ajusta a los valores recomendados por la Organización Mundial de la Salud (OMS). Revista Médica Herediana, 34(4): 236-238. https://doi.org/10.20453/rmh.v34i4.5155
[28] Reátegui-Romero, W., Sánchez-Ccoyllo, O.R., de Fatima Andrade, M., Moya-Alvarez, A. (2018). PM2.5 estimation with the WRF/Chem model, produced by vehicular flow in the lima metropolitan area. Open Journal of Air Pollution, 7(3): 215-243. https://doi.org/10.4236/ojap.2018.73011
[29] Silva, J., Rojas, J., Norabuena, M., Molina, C., Toro, R. A., Leiva-Guzmán, M.A. (2017). Particulate matter levels in a South American megacity: The metropolitan area of Lima-Callao, Peru. Environmental Monitoring and Assessment, 189: 635. https://doi.org/10.1007/s10661-017-6327-2
[30] Tapia, V., Carbajal, L., Vásquez, V., Espinoza, R., Vásquez-Velásquez, C., Steenland, K., Gonzales, G. F. (2018). Reordenamiento vehicular y contaminación ambiental por material particulado (2, 5 y 10), dióxido de azufre y dióxido de nitrógeno en Lima Metropolitana, Perú. Revista Peruana de Medicina Experimental y Salud Pública, 35: 190-197. https://doi.org/10.17843/rpmesp.2018.352.3250
[31] Delgado Villanueva, A., Loayza, A.A. (2020). Modeling and air quality assessment through Grey Clustering analysis, case study: Lima Metropolitana. Tecnia, 30(1): 114-120. https://doi.org/10.21754/tecnia.v30i1.588
[32] Ilizarbe-Gonzáles, G.M., Rojas-Quincho, J.P., Cabello-Torres, R.J., Ugarte-Alvan, C.A., Reynoso-Quispe, P., Valdiviezo-Gonzales, L.G. (2020). Chemical characteristics and identification of PM10 sources in two districts of Lima, Peru. Dyna, 87(215): 57-65. http://doi.org/10.15446/dyna.v87n215.83688
[33] Mousavinezhad, S., Choi, Y., Khorshidian, N., Ghahremanloo, M., Momeni, M. (2024). Air quality and health co-benefits of vehicle electrification and emission controls in the most populated United States urban hubs: Insights from New York, Los Angeles, Chicago, and Houston. Science of The Total Environment, 912: 169577. https://doi.org/10.1016/j.scitotenv.2023.169577
[34] Beedham, M. (2023). TomTom traffic index headlines: 2022’s traffic insights and the cost-of-driving. https://www.tomtom.com/newsroom/explainers-and-insights/the-cost-of-driving-in-a-cost-of-living-crisis/.
[35] Wang, P., Zhang, R., Sun, S., Gao, M., Zheng, B. (2023). Aggravated air pollution and health burden due to traffic congestion in urban China. Atmospheric Chemistry and Physics, 23(5): 2983-2996. https://doi.org/10.5194/acp-23-2983-2023
[36] Sánchez-Ccoyllo, O.R., Ordoñez-Aquino, C.G., Arratea-Morán, J., Marín-Huachaca, N.S., Reátegui-Romero, W. (2021). Describing aerosol and assessing health effects in Lima, Peru. International Journal of Environmental Science and Development, 12(12): 355-362. http://doi.org/10.18178/ijesd.2021.12.12.1361
[37] Tapia, V., Steenland, K., Vu, B., Liu, Y., Vásquez, V., Gonzales, G.F. (2020). PM 2.5 exposure on daily cardio-respiratory mortality in Lima, Peru, from 2010 to 2016. Environmental Health, 19: 63. https://doi.org/10.1186/s12940-020-00618-6
[38] Bernal Aybar, C.E. (2020). Contaminación por material particulado (PM10 y PM2.5) y enfermedades respiratorias agudas a menores de 5 años en Lomas de Carabayllo, Lima - Perú. Revista De Investigación Multidisciplinaria CTSCAFE, 3(8): 10.
[39] Davila Cordova, J.E., Tapia Aguirre, V., Vasquez Apestegui, V., Ordoñez Ibarguen, L., Vu, B.N., Steenland, K., Gonzales, G.F. (2020). Association of PM 2.5 concentration with health center outpatient visits for respiratory diseases of children under 5 years old in Lima, Peru. Environmental Health, 19: 7. https://doi.org/10.1186/s12940-020-0564-5
[40] Tapia, V.L., Vasquez-Apestegui, B.V., Alcantara-Zapata, D., Vu, B., Steenland, K., Gonzales, G.F. (2021). Association between maximum temperature and PM2. 5 with pregnancy outcomes in Lima, Peru. Environmental Epidemiology, 5(6): e179. https://doi.org/10.1097/EE9.0000000000000179
[41] Carranza, C.C., Dongo, M.M., Gómez, W.A., Abad, R.P., Vega, A.G., Cárdenas, S.L. (2002). Relaciones entre calidad ambiental y calidad de vida en Lima Metropolitana. Revista del Instituto de Investigación de la Facultad de Minas, Metalurgia y Ciencias Geográficas, 5(9): 47-52.