Comparative Effects of Ginkgo Biloba and Milk Thistle Extracts on Oxidative Stress, Inflammation, and Glycemic Parameters in Alloxan-Induced Diabetic Rats

Nawar R. Jaber*![]() | Sura S Talib
| Sura S Talib![]() | Zahrra A. Abed
| Zahrra A. Abed![]() | Noor Naji Hasan
| Noor Naji Hasan![]() | Hazzim I. Abdilbari
| Hazzim I. Abdilbari![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Diabetes mellitus (DM) has been well-known as a global health issue for decades, due to its elevated occurrence and heightened rates of mortality and morbidity. For a very long time, the usage of herbal therapy has been documented for DM treatment and its complications. The aim of this study was to investigate the effect of Ginkgo biloba leaves ethanol extract (GBE), aqueous milk thistle seeds extract (MTE), and metformin (MET) on some physiological parameters in alloxan-induced diabetic rats. 25 male albino rats were divided into five groups (n = 5/group): control (non-diabetic), diabetic (positive control), metformin-treated diabetic (MET), GBE-treated diabetic (50 mg/kg), and MTE-treated diabetic (60 mg/kg). Diabetes was induced by alloxan injection, and treatments were administered orally. Compared to diabetic control, all treatments (MTE, GBE, and MET) significantly increased serum superoxide dismutase (SOD) activity and decreased malondialdehyde (MDA) levels. MTE significantly elevated serum tumor necrosis factor-alpha (TNF-α). Regarding blood glucose, MET effectively lowered levels, while GBE showed a variable response. Notably, MTE induced a significant increase in blood glucose compared to both the control and diabetic groups. The statistical significance for these findings was (P < 0.05). Our findings indicate that both Ginkgo biloba leaves ethanol and aqueous milk thistle seeds extracts demonstrated ameliorative effects on physiological parameters in diabetic rats, particularly by improving antioxidant status and modulating inflammation. This suggests a potential for the phytotherapeutic modulation of diabetic complications, highlighting these plant-based extracts as promising candidates for further research into managing diabetes.
diabetes, GBE, MTE, alloxan, rat
Diabetes mellitus (DM) has been well-known as a global health issue for decades. Scientific research for possible curative methods from meditative plants has been persistent for this illness [1]. Due to its elevated occurrence and heightened rates of mortality and morbidity, in 2015, the International Diabetes Foundation (IDF) estimated that 415 million people aged 20-79 were encountering diabetes. It is expected that this number will rise by 2040 to more than 600 million adults for various reasons, including obesity [2].
Caused by the insufficiency or poor production of the insulin hormone in the pancreas due to the destruction of ß-cells. Many health complications are generated by DM; some are life-threatening. The development of synthetic medications is ongoing to this day; still, no curative method is provided. Adverse effects can be caused by chronic use of these medications; some can be severe [3]. DM is mainly classified into type 1 DM and type 2 DM; other types include monogenic diabetes syndromes and gestational DM, type 2 DM is the most common type, which represents 90% of the cases [4].
Even though there are many new, improved treatment approaches for DM, the side effects of antidiabetic medications are very grave [5]. One of the cornerstones for type 1 DM treatments is insulin therapy, which has received wide acceptance in many countries. Side effects of this treatment, unfortunately, limited its use, such as hypoglycemia, lipohypertrophy, weight gain, and allergic reactions [6].
As for type 2 DM, there are a lot of flora (plants) in Asian traditional medicine that demonstrate their power in treating DM, totaling 183; and phytochemicals are gaining traction for DM treatment and are highly researched [6].
Recent studies indicated the significant role that active compounds play in comparison with crude herbal extract in DM treatment [7]. Apart from this, improvement in ß-cell in the pancreas was also noted with the use of phytochemicals [8]. Dating back 4000 years in Iraq, the Sumerians recorded the use of herbal plants as remedies for many illnesses in clay tablets as a medical document [1]. The Sumerians utilized these plants to create remedies for ailments ranging from digestive disorders to infections, laying the foundation for herbal medicine. Their knowledge was later passed down to subsequent civilizations, including the Babylonians and Assyrians, who expanded on these practices [9]. The origins of human use can be traced back 60,000 years in fossil records [10].
Used 5000 years ago in traditional Chinese medicine, Ginkgo biloba L. (Ginkgoaceae) (GB) existed 250 million years ago, is a living fossil, an ancient tree with many known remarkable therapeutic properties [11]. GB trees have immense medicinal value in both fruits and leaves (Figure 1(A)) [12]. The paleobotanists elucidated that GB is a member of the Ginkgoaceae family, one of the endemic species and a relic in China [13]. Praised for its enormous adaptability and high resistance to pests, pollution, and almost all pathogens in the environment [14].
(A) Ginkgo biloba leaves
(B) Milk thistle plant
(C) Milk thistle seeds
Figure 1. Study plants
Reaching 20-35 meters tall, GB is a deciduous tree notable for its fan-shaped, bilobed leaves that turn yellow in the fall. Being dioecious, individual trees are either male or female. Female trees produce seeds with a fleshy, foul-smelling covering [15].
Unlike any other antioxidants, GB’s active compound, flavonoids, acts on a mitochondrial level. Plant extract contains more than 60 bioactive ingredients with a unique structure [16]. The leaf extract, which is the most common part of the plant used, has a great deal of phytochemicals like terpenoids and flavone glycosides; other parts of GB can be useful but also toxic, like seeds and fruits [17].
Silybum marianum (L.) Gaertn. is the scientific name of milk thistle (MT), which belongs to the Asteraceae family, one of the most rapidly expanding and ubiquitous medicinal plants across the world [18]. The MT plant has a large brig with purple-colored flowers that grow in sunny areas (Figure 1(B)) [19]. Found originally in Asia, the Mediterranean mountains, and North Africa, MT today is seen growing in other parts of the globe [20]. Native to Australia, Northern Africa, North and South America, Southern Europe, and a handful of places in Asia, MT is known to be an annual or biennial plant [21]. MT is considered to have a cypsela that looks like a seed, but in reality, it is a fruit (Figure 1(C)) [22].
MT chemical composition contains (70–80%) silymarin, which contains six flavonolignans [23]. More than 2000 years ago, conventionally, this plant usage was not limited to liver issues but also for kidney, gallbladder, and spleen treatment [24]. Research in 2023 indicated that a topical gel can be utilized for wound recovery [25].
This study hypothesizes that both Ginkgo biloba leaf ethanol extract (GBE), aqueous milk thistle seed extract (MTE), and metformin (MET) can ameliorate diabetic-induced oxidative and inflammatory damage.
2.1 Experimental animals
The study was conducted on 25 male albino rats, 8 weeks old, and weighing 250-300 g. The animals were obtained from the animal house of the Biotechnology Research Center/Al-Nahrain University in Baghdad. The rats were put under the same standard conditions of room temperature, a 12/12 h light/dark cycle, humidity, and ventilation, and had free access to food and water ad libitum throughout the study period.
2.2 Diabetes induction
Alloxan was used to induce type 1 diabetes in this experiment [26]. The alloxan-induced diabetic rat model was selected for this study as it represents a well-established and consistent model for studying type 1 diabetes and evaluating the efficacy of potential therapeutic compounds against hyperglycemia and associated oxidative stress, purchased from Sigma-Aldrich Chemical Co. (St. Louis, MO, USA). Each animal was injected intraperitoneally with 36 mg/kg of the diabetogenic agent alloxan in a single injection.
2.3 Plant extracts preparation
The cold ethanol extraction method was utilized on 100 g of dried GB leaves; the leaves were cleaned, ground, and soaked in 70% ethanol at room temperature for 7 days in a dark place with occasional stirring. After filtration, the ethanol was evaporated at 40℃, and the extract was concentrated [27]. The extraction process resulted in a yield of 12.0% for the GBE from the GB leaves.
The aqua extraction method was performed on 100 g of dried MT seeds to acquire the extract. MT seeds were ground thoroughly, mixed with water, and heated to 60℃. Then, the mixture was filtered with filter paper to remove solids. The aqueous extract was then concentrated and dried to obtain a stable powder [24]. The extraction process resulted in a yield of 10.5% for the MTE from the MT seeds.
2.4 Other chemicals
Metformin (500 g) (Metforal) was purchased from Laboratori Guidotti (S.p.A., Pisa, Italy).
2.5 Study groups and treatment schedule
The rats were divided into five groups; each group contained five rats. After 24 h of alloxan injection, the diabetic state was confirmed using a blood glucose monitor (On Call Plus, ACON Laboratories, Inc., Germany). Rats with blood glucose >200 mg/dl were considered diabetic; the detection was performed using blood samples from the tail vein using a sterile lancet [28]. Groups: Non-diabetic control (Cont), diabetic positive control (Pos.Allox), diabetic + metformin (MET) (oral), diabetic + GB extract (GBE) (50 mg/kg, oral), diabetic + MT extract (MTE) (60 mg/kg, oral). The specific doses of GBE (50 mg/kg) and MTE (60 mg/kg) were chosen as a novel approach to explore their anti-diabetic effects, as these concentrations had not been previously tested in this specific animal model. All experiments were conducted ten days after diabetic onset. Animals were euthanized using an anesthetic overdose (e.g., sodium pentobarbital, 150 mg/kg i.p.) for a humane and painless procedure. Confirm euthanasia by ensuring the absence of a heartbeat and reflexes [29]. A cardiac puncture was performed for blood and serum sample collection.
2.6 Physiological parameters measurements
Animals blood glucose levels were measured after and before the experiments; furthermore, complete blood count (CBC) was estimated in the blood using GENEX count-60 (GENEX laboratories, USA), along with C- reactive protein slide test (Arlington Scientific ASI CRP-latex, USA), tumor necrosis factor alpha (TNF-α), malondialdehyde (MDA), and superoxide dismutase (SOD) estimated in serum after the experiment was finished using HumaReader HS (Human, Germany).
2.7 Statistical analysis
Data were analyzed using Minitab software analysis of variance (one-way ANOVA) to determine significant differences between group means. Descriptive statistics, including means and standard deviations, were calculated for each group and are presented graphically. Statistical significance was established a priori (P < 0.05).
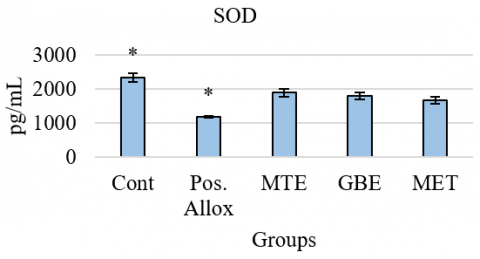
3.1 Activity of superoxide dismutase (SOD) in serum
Figure 2 shows serum total SOD activity, revealing a significant decrease in the treatment groups, specifically, the MTE group had SOD levels of 1881 ± 244, the GBE group had 1783 ± 229, and MET group had 1657.3 ± 221.9 compared to the control group (2333 ± 278) and an increase in the treatment groups compared to the diabetic group (1172 ± 36.9). As for the variations between groups, it was clear that an increase in SOD levels was seen in the MTE group compared to the GBE and MET groups.
The current study revealed that SOD levels decreased in all treated groups compared to the control group. It is well known that all living organisms strive to maintain homeostasis in their internal environment, including redox balance. In this result, introducing antioxidants can disrupt the body’s natural antioxidant response. This disruption makes the body downregulate its own SOD production because it is receiving external antioxidants [30].
The doses of GBE (50 mg/kg) and MTE (60 mg/kg) were selected as a novel approach to explore their anti-diabetic and antioxidant effects, as these specific concentrations have not been previously investigated in alloxan-induced diabetic rats. The findings from this study therefore represent a unique contribution to the literature, providing a foundational dataset for future research, particularly for dose-response studies aimed at identifying the optimal therapeutic concentration.
The use of MET in this study was intentional. While insulin is a more direct control for the type 1 diabetes model, MET allowed us to evaluate if the extracts could act on broader type 1 diabetes complications like oxidative stress and inflammation, similar to MET itself.
MTE, GBE, and MET treatment had some positive effect in comparison to the diabetic state, by increasing SOD levels. SOD’s antioxidant enzymes are considered a defense line against free radicals and illness [31]. The overexpression of SOD in the treated groups can be caused by an imbalance associated with various pathological conditions [32]. Many studies have explored the potential antioxidant properties of plant extracts to mitigate oxidative stress and enhance SOD activity [33]. As for MET, studies suggest that this treatment exerts anti-oxidative effects that elevate SOD levels [34].
MTE might be more effective in boosting SOD activity than GBE and MET. Some studies have shown an increase in SOD activity after using GBE due to its therapeutic applications [35]. As for MTE, the anti-inflammatory and antioxidant abilities aided in reducing the oxidative burden [36], which indicates the beneficial impact on antioxidant defense.
Figure 2. Levels of superoxide dismutase (SOD) in study groups
* stands for significant at P≤0.05 (Pos.Allox)
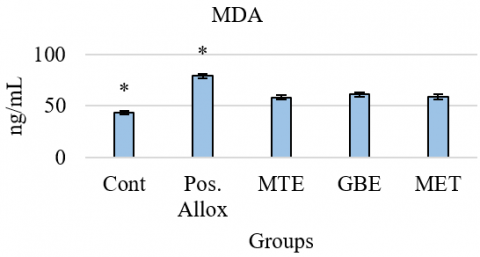
3.2 Activity of malondialdehyde (MDA) in serum
Figure 3 shows serum MDA activity, revealing a significant increase in the treatment groups, specifically, the MTE group had an MDA level of (58.18 ± 4.67), the GBE group had (60.95 ± 5.1), and the MET group had (58.95 ± 5.56) compared to the control group (43.09 ± 3.33) and a decrease in the treatment groups compared to the diabetic group (78.86 ± 5.04). As for the variations between groups, an increase in MDA levels was significant in the GBE group compared to the MTE and MET groups.
On the other hand, MDA levels were decreased in the treatment groups compared to the diabetic group. MDA is an indicator of lipid peroxidation and oxidative stress; high levels can be a biomarker for these processes [37]. Antioxidants in plant extract can reduce MDA by scavenging for free radicals and increasing lipid peroxidation, as some research has shown. GBE is well known to help in MDA reduction as well by increasing lipid peroxidation [38]. MTE has been widely known to reduce MDA levels by mitigating oxidative stress [39, 40], which is in agreement with this study. MET showed its capability in reducing MDA levels in diabetic rats in this study. MET can activate AMP-activated protein kinase (AMPK), improve mitochondrial functions, decrease lipid peroxidation and oxidative stress, resulting in a lowering of MDA levels [40, 41]. MDA levels were about the same between the treated groups. Despite their different mechanisms, this might have converged on a common endpoint in terms of their impact on lipid peroxidation; they may also affect similar signaling pathways that regulate antioxidant enzyme expression.
Figure 3. Levels of malondialdehyde (MDA) in study groups
* stands for significant at P≤0.05 (Pos.Allox)
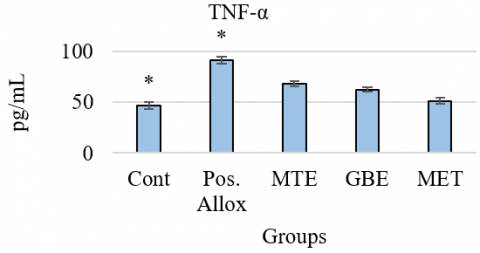
3.3 Activity of tumor necrosis factor alpha (TNF-α) in serum
Figure 4 shows serum TNF-α activity, revealing a significant increase in the treatment groups, specifically, the MTE group had TNF-α levels of (67.94 ± 6.14), the GBE group had (62.39 ± 5.16), and the MET group had (51.28 ± 6.61) compared to the control group (46.83 ± 7.33) and a decrease in the treatment groups compared to the diabetic group (91.28 ± 8.14). As for the variations between groups, an increase in TNF-α levels was significant in the MTE group compared to the GBE and MET groups.
The yielded results revealed that there was an increase in TNF-α levels in the treatment groups compared to the control group. TNF-α is an inflammatory parameter that increases in diseases due to its inflammatory nature [40]. The treatments themselves might induce a cellular stress response, which can activate inflammatory pathways and increase TNF-α expression [40]. Both plant extracts and MET made a substantial reduction in TNF-α levels. According to a previous study, GBE can inhibit inflammation, which causes a significant drop in TNF-α level [42]. The extract has been shown to suppress monocyte activation by blocking the toll-like receptor 4 (TLR4) pathway [43], which leads to a reduction in the production of inflammatory cytokines like TNF-α [44]. MTE was found to demote TNF-α levels in some diseases like insulin resistance [45, 46] and decrease the inflammatory process by primarily targeting the inflammatory markers or has a border effect on the immune system [47, 48]. MTE decreases TNF-α levels through a combination of mechanisms, including AMPK activation, NF-κB inhibition, ROS modulation, and effects on immune cells. Its ability to improve metabolic control also contributes to its anti-inflammatory effects [49].
Figure 4. Levels of tumor necrosis factor alpha (TNF-α) in study groups
* stands for significant at P≤0.05 (Pos.Allox)
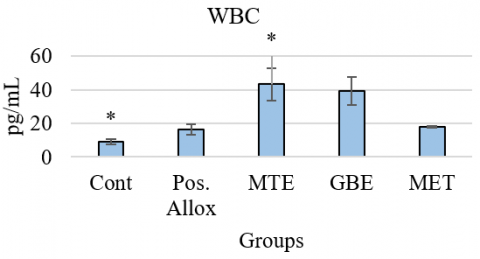
3.4 Total white blood cells (WBCs) activity in blood
Figure 5 shows blood WBC activity, revealing a significant increase in the treatment groups. Specifically, the MTE group had a WBC level of 43.26 ± 21.42, the GBE group had 39.08 ± 18.43, and the MET group had 17.8 ± 1.095 compared to the control group (9.2 ± 3.27) and an increase in the treatment groups compared to the diabetic group (16.22 ± 6.91). As for the variations between groups, an increase in WBC levels was significant in the MTE group compared to the GBE and MET groups.
Figure 5. Levels of white blood cells (WBCs) in study groups
* stands for significant at P≤0.05(Pos.Allox)
The current study revealed that WBC count was elevated in the treatment groups compared to the control group. This indicates a complex immune response and could be due to the body recognizing the treatment as foreign or due to the activation of inflammatory pathways [50]. Both plant extracts have increased the levels of WBCs compared to the diabetic group. The treatment, especially MTE, may indicate that the treatment is causing a non-specific inflammatory or immune-stressed state, rather than a beneficial immunomodulatory effect.
In some studies, MTE was found to increase WBC count and might be related to certain immune cell stimulation or the mobilization of WBC from the storage pool [24].
GBE can influence the production of cytokines, which are signaling molecules that regulate immune responses. Some cytokines, like TNF-α and IL-1, are known to stimulate WBC production. Therefore, GBE's interaction with cytokine pathways could lead to an increase in WBCs [51].
As for the MET group, the levels of WBC count were lower than those of the diabetic, GBE, and MTE groups. MET's ability to lower WBC count is linked to its anti-inflammatory and immunomodulatory effects, by macrophage polarization, T cell Modulation, and reducing chemokine production [52].
3.5 Differential white blood cells (WBCs) activity in blood
Figure 6 shows the lymphocyte (LYM) activity, revealing a significant increase in LYM activity in the treatment groups, specifically, the MTE group had an LYM levels of (20.8 ± 5.02), the GBE group had (20.2 ± 4.96), and MET group had (15.08 ± 1.479) compared to the control group (5.44 ± 2.62) and an increase in the treatment groups compared to the diabetic group (12.54 ± 6.22). As for the variations between groups, the MTE and GBE groups showed an increase in LYM activity compared to the MET group, but not between them.
Figure 6. Levels of lymphocyte (LYM) cells in study groups
* stands for significant at P≤0.05 (Pos.Allox)
The findings indicated that CRP agglutination concentrations in serum were lower than 5 mg/dl, thereby considered negative values for all groups.
Lymphocyte is an excellent indicator for innate immunity [53]; the negative results of the CRP test are in correlation with this finding. Our observations confirmed that there was an increase in LYM levels in the treated groups compared to the control and diabetic groups. The effect of the extracts on innate response may be explained partially by their influence on cytokine production and antioxidant activity [54]. MET might have differential effects on various lymphocyte subsets (e.g., T cells, B cells, NK cells). It could potentially stimulate the proliferation or activation of specific lymphocyte populations, leading to an overall increase in LYM count. While Metformin is broadly anti-inflammatory, an elevated LYM can be indicative of heightened systemic inflammation or the expansion of pro-inflammatory T-cell subsets [55].
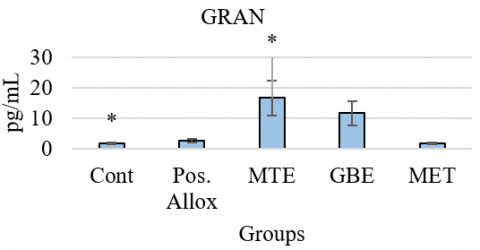
Figure 7 shows the granulocyte (GRAN) activity, revealing a significant increase in GRAN activity in the treatment groups. Specifically, the MTE group had GRAN levels of (16.6 ± 12.87), the GBE group had (11.6 ± 8.79), compared to the control group (1.56 ± 0.602). Yet, the MET group had a slight increase of (1.64 ± 0.669) compared to the control group, and an increase in the MTE and GBE groups compared to the diabetic group (2.57 ± 1.117). As for the variations between groups, MTE group LYM levels were higher than both GBE and MET groups, and GBE group LYM levels were higher than MET group.
Figure 7. Levels of granulocyte (GRAN) cells in study groups
* stands for significant at P≤0.05 (Pos.Allox)
Comparing the GBE and MTE groups to the diabetic group, it was noticed that the treated groups had an increase in GRAN activity. Some studies suggest that GBE can modulate the activity of neutrophils and other granulocytes [56], while MTE, particularly silymarin, and MET can also modulate immune responses. However, in the context of chronic diabetic inflammation, persistently elevated levels of granulocytes are often a marker of a sustained inflammatory state [57-59]. The increase observed here could be a non-specific inflammatory response to the extract, highlighting a potential limitation of the extract's therapeutic application [60-62].
3.6 Blood sugar levels(glucose) in serum
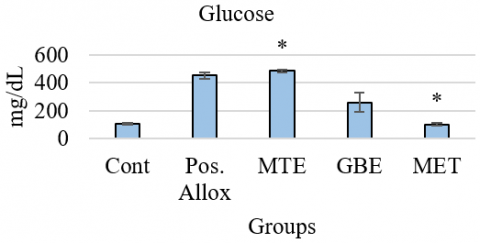
Figure 8 displays blood glucose levels. The MTE group exhibited a highly unexpected and significant increase in glucose levels (483.6 ± 20.28) compared to both the control group (103.8 ± 15.42) and the diabetic group (450.6 ± 50.8). The GBE group also showed a significant increase in glucose levels (259 ± 153.1) compared to the control group, but a significant decrease compared to the diabetic group. The MET group showed a slight decrease in glucose levels (101 ± 22.15) compared to the control group, and a significant decrease compared to the diabetic group. Notably, the GBE group exhibited high variability in glucose levels. As for the variations between treated groups, the MTE group recorded the highest glucose levels, and the MET group recorded the lowest.
Figure 8. Levels of blood sugar (glucose) in study groups
* stands for significant at P≤0.05 (Pos.Allox)
A notable variation in blood sugar levels was seen in this study. The treatment groups showed a significant increase in glucose levels compared to the control group. These findings suggest that GBE may have partial hypoglycemic effects in a diabetic environment but is unable to fully normalize blood glucose levels. It is also possible that GBE has hyperglycemic effects, or that the already disrupted glucose regulation of the diabetic rats altered the effects of the GBE [63].
As for MET, hypoglycemia is a well-known adverse effect of this medication. Furthermore, this paradoxical effect could be a dose-dependent response, suggesting that the specific concentrations used may be toxic or lead to adverse effects [64].
GBE and MET had a substantial effect by decreasing blood sugar levels compared with the diabetic group. GBE is known to have this ability, particularly in individuals with diabetes or prediabetes conditions, by inhibiting the activity of enzymes involved in carbohydrate digestion and absorption [54]. In addition, GBE has been shown to enhance insulin secretion and sensitivity, a key factor in regulating blood sugar levels [63]. MTE had the opposite effect; high levels of blood sugar were noticed in the treated animals compared with the diabetic group, suggesting a hyperglycemic effect of the extract. This contradicts many studies that reported a hypoglycemic effect of MTE [65]. A study confirmed that using low doses of MTE can have no effect on lowering blood sugar and insulin levels, but can reduce pancreatic damage [66]. While MTE demonstrated a clear adverse effect on blood glucose regulation, its significant ability to increase SOD activity and decrease MDA levels indicates a potent ameliorative effect on oxidative stress, an important complication of diabetes.
The significant elevation in blood glucose with MTE suggests a more complex mechanism of action than initially anticipated. One potential explanation for this paradoxical effect is the presence of endogenous carbohydrates or other glucose-releasing compounds within the crude extract itself, which may have contributed to the observed hyperglycemia. An alternative hypothesis is that the MTE, at the administered dose, may be inducing a physiological stress response. The activation of the hypothalamic-pituitary-adrenal (HPA) axis can lead to an increase in glucocorticoids such as cortisol, which are known to raise blood glucose levels by promoting gluconeogenesis and glycogenolysis.
While these are hypotheses that require further investigation, our findings propose that a border analysis of stress hormones is a critical next step to fully understand the effects of MTE in this model.
GBE and MTE together, these herbal extracts may improve overall metabolic control, reduce inflammation and oxidative stress, and potentially mitigate some side effects of metformin, thereby offering a valuable combined therapeutic strategy in diabetes management. This synthesis is based on clinical trials, pilot studies, and reviews exploring their pharmacological and clinical effects in diabetic and metabolic syndrome patients [67-69].
GBE and MTE can improve several markers of oxidative stress and inflammation in diabetic rats by boosting SOD, WBC count, and reducing MDA and TNF-α. MTE unexpectedly increased blood sugar, while GBE lowered it. These findings suggest potential therapeutic benefits, but the hyperglycemic effect of MTE requires further investigation. In conclusion, GBE is considered the best material in treating diabetes parameters imbalances.
A limitation of the current study is a lack of detailed phytochemical analysis of the extracts, such as quantification of active compounds like silymarin and ginkgolides, and the absence of histopathological analysis of the pancreas and liver. Further studies should aim to chemically characterize the extracts to better correlate specific compounds with the observed physiological effects, and include H&E staining to directly visualize the protective effects of these extracts on pancreatic beta-cell integrity and hepatic architecture. The present study is limited by its lack of a comprehensive dose-response analysis for the GBE and MTE extracts. Future research should focus on testing a wider range of concentrations to better characterize the therapeutic window and dose-dependent effects of these compounds.
The authors are grateful to the Biotechnology Research Center, Environmental Biotechnologies Department, Al-Nahrain University, for their encouragement and support in conducting the study.
Ethics approval and consent to participate
The study protocol was approved by the ethical committee at Al-Nahrain University, as per decision no. (No.E.B.15 in 2.1.2023), Biotechnology Research Center, Environmental Biotechnologies Department, Al-Nahrain University, Baghdad, Iraq.
[1] Asafo-Agyei, T., Appau, Y., Barimah, K.B., Asase, A. (2023). Medicinal plants used for management of diabetes and hypertension in Ghana. Heliyon, 9(12): e22977. https://doi.org/10.1016/j.heliyon.2023.e22977
[2] Ogurtsova, K., da Rocha Fernandes, J.D., Huang, Y., Linnenkamp, U., Guariguata, L., Cho, N.H., Cavan, D., Shaw, J.E., Makaroff, L.E. (2017). IDF diabetes atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Research and Clinical Practice, 128: 40-50. https://doi.org/10.1016/j.diabres.2017.03.024
[3] Kumar, S., Mittal, A., Babu, D., Mittal, A. (2021). Herbal medicines for diabetes management and its secondary complications. Current Diabetes Reviews, 17(4): 437-456. https://doi.org/10.2174/1573399816666201103143225
[4] Yun, J.S., Ko, S.H. (2021). Current trends in epidemiology of cardiovascular disease and cardiovascular risk management in type 2 diabetes. Metabolism Clinical and Experimental, 123: 154838. https://doi.org/10.1016/j.metabol.2021.154838
[5] Chaudhury, A., Duvoor, C., Reddy Dendi, V.S., Kraleti, S., et al. (2017). Clinical review of antidiabetic drugs: Implications for Type 2 diabetes mellitus management. Frontiers in Endocrinology, 8: 6. https://doi.org/10.3389/fendo.2017.00006
[6] American Diabetes Association Professional Practice Committee. (2025). Pharmacologic approaches to glycemic treatment: Standards of care in diabetes. Diabetes Care, 48(Supplement_1): S181-206. https://doi.org/10.2337/dc25-S009
[7] Omale, S., Amagon, K.I., Johnson, T.O., Bremner, S.K., Gould, G.W. (2023). A systematic analysis of anti-diabetic medicinal plants from cells to clinical trials. PeerJ, 11: e14639. https://doi.org/10.7717/peerj.14639
[8] Chigurupati, S., Al-Murikhy, A., Almahmoud, S.A., Almoshari, Y., Saber Ahmed, A., Vijayabalan, S., Ghazi Felemban, S., Raj Palanimuthu, V. (2022). Molecular docking of phenolic compounds and screening of antioxidant and antidiabetic potential of Moringa oleifera ethanolic leaves extract from Qassim region, Saudi Arabia. Saudi Journal of Biological Sciences, 29(2): 854-859. https://doi.org/10.1016/j.sjbs.2021.10.021
[9] Kramer, S.N. (1981). History Begins at Sumer: Thirty-Nine Firsts in Recorded History. University of Pennsylvania Press.
[10] Xiao, P. (1988). A Pictorial Encyclopaedia of Chinese Medicine, v1-10. Commercial Press, Hong Kong.
[11] Shi, Q.W., Li, L.G., Huo, C.H., Zhang, M.L., Wang Y.F. (2010). Study on natural medicinal chemistry and new drug development. Chinese Traditional and Herbal Drugs, 41(10): 1583-1589.
[12] Montes, P., Ruiz-Sanchez, E., Rojas, C., Rojas, P. (2015). Ginkgo biloba extract 761: A review of basic studies and potential clinical use in psychiatric disorders. CNS Neurol Disord Drug Targets, 14(1): 132-149. https://doi.org/10.2174/1871527314666150202151440
[13] Biernacka, P., Adamska, I., Felisiak, K. (2023). The potential of Ginkgo biloba as a source of biologically active compounds-A review of the recent literature and patents. Molecules, 28(10): 3993. https://doi.org/10.3390/molecules28103993
[14] Chen, Y., Fu, C., Wu, Z., Xu, H., Liu, H., Schneider, H., Lin, J. (2021). Ginkgo biloba. Trends in Genetics, 37(11): 1046. https://doi.org/10.1016/j.tig.2021.07.001
[15] Lin, H.Y., Li, W.H., Lin, C.F., Wu, H.R., Zhao, Y.P. (2022). International biological flora: Ginkgo biloba. Journal of Ecology, 110(4): 951-982. https://doi.org/10.1111/1365-2745.13856
[16] Cybulska-Heinrich, A.K., Mozaffarieh, M., Flammer, J. (2012). Ginkgo biloba: an adjuvant therapy for progressive normal and high tension glaucoma. Molecular Vision, 18: 390-402.
[17] Liu, L., Wang, Y., Zhang, J., Wang, S. (2021). Advances in the chemical constituents and chemical analysis of Ginkgo biloba leaf, extract, and phytopharmaceuticals. Journal of Pharmaceutical and Biomedical Analysis, 193: 113704. https://doi.org/10.1016/j.jpba.2020.113704
[18] Jaggy, H., Koch, E. (1997). Chemistry and biology of alkylphenols from Ginkgo biloba L. Die Pharmazie, 52(10): 735-738.
[19] Habán, M., Zvercová, D., Adamjaková, M. (2021). Evaluation of variability of silymarin complex in Silybi mariani fructus harvested during two production years. European Pharmaceutical Journal, 68(1): 40-45. https://doi.org/10.2478/afpuc-2020-0023
[20] Di Martino, J.S., Nobre, A.R., Mondal, C., Taha, I., Farias, E.F., Fertig, E.J., Naba, A., Aguirre-Ghiso, J.A., Bravo-Cordero, J.J. (2022). A tumor-derived type III collagen-rich ECM niche regulates tumor cell dormancy. Nature Cancer, 3(1): 90-107. https://doi.org/10.1038/s43018-021-00291-9
[21] Hlangothia, D., Abdel-Rahman, F., Nguyen, T., Anthony, K., Saleh, M.A. (2016). Distribution of Silymarin in the Fruit of Silybum marianum L. Pharmaceutica Analytica Acta, 7: 511. https://doi.org/10.4172/2153-2435.1000511
[22] Porwal, O., Ameen, M.S.M., Anwer, E.T., Uthirapath, S., Ahama, J., Tahsin A. (2019). Silybum marianum (Milk Thistle): Review on its chemistry, morphology, ethno medical uses, phytochemistry and pharmacological activities. Journal of Drug Delivery and Therapeutics, 9(5): 199-206. https://doi.org/10.22270/jddt.v9i5.3666
[23] Rainone, F. (2005). Milk thistle. American Family Physician, 72(7): 1285-1288.
[24] Khazaei, R., Seidavi, A., Bouyeh, M. (2022). A review on the mechanisms of the effect of silymarin in milk thistle (Silybum marianum) on some laboratory animals. Veterinary Medicine and Science, 8(1): 289-301. https://doi.org/10.1002/vms3.641
[25] Malik, B., Bekir, E. (2023). Formulation and in vitro /in vivo evaluation of Silymarin solid dispersion- based topical gel for wound healing. Iraqi Journal of Pharmaceutical Sciences, 32(Suppl.): 42-53. https://doi.org/10.31351/vol32issSuppl.pp42-53
[26] Lenzen, S. (2008). The mechanisms of alloxan- and streptozotocin-induced diabetes. Diabetologia, 51(2): 216-226. https://doi.org/10.1007/s00125-007-0886-7
[27] Piazza, S., Pacchetti, B., Fumagalli, M., Bonacina, F., Dell'Agli, M., Sangiovanni, E. (2019). Comparison of two Ginkgo biloba L. extracts on oxidative stress and inflammation markers in human endothelial cells. Mediators of Inflammation, 2019(1): 6173893. https://doi.org/10.1155/2019/6173893
[28] Furman, B.L. (2015). Streptozotocin-induced diabetic models in mice and rats. Current Protocols in Pharmacology, 70(1): 5.47.1-5.47.20. https://doi.org/10.1002/0471141755.ph0547s70
[29] American Veterinary Medical Association. (2020). AVMA Guidelines for the Euthanasia of Animals: 2020 Edition. American Veterinary Medical Association.
[30] Rahal, A., Kumar, A., Singh, V., Yadav, B., Tiwari, R., Chakraborty, S., Dhama, K. (2014). Oxidative stress, prooxidants, and antioxidants: The interplay. BioMed Research International, 2014(1): 761264. https://doi.org/10.1155/2014/761264
[31] Ighodaro, O.M., Akinloye, O.A. (2018). First line defence antioxidants-superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPX): Their fundamental role in the entire antioxidant defence grid. Alexandria Journal of Medicine, 54(4): 287-293. https://doi.org/10.1016/j.ajme.2017.09.001
[32] Rosa, A.C., Corsi, D., Cavi, N., Bruni, N., Dosio, F. (2021). Superoxide dismutase administration: A review of proposed human uses. Molecules, 26(7): 1844. https://doi.org/10.3390/molecules26071844
[33] Di Meo, F., Cuciniello, R., Margarucci, S., Bergamo, P., Petillo, O., Peluso, G., Filosa, S., Crispi, S. (2020). Ginkgo biloba prevents oxidative stress-induced apoptosis blocking p53 activation in neuroblastoma cells. Antioxidants, 9(4): 279. https://doi.org/10.3390/antiox9040279
[34] Zhang, S., Xu, H., Yu, X., Wu, Y., Sui, D. (2017). Metformin ameliorates diabetic nephropathy in a rat model of low-dose streptozotocin-induced diabetes. Experimental and Therapeutic Medicine, 14(1): 383-390. https://doi.org/10.3892/etm.2017.4475
[35] Amaldoss, M.J.N., Sorrell, C.C. (2022). ROS modulating inorganic nanoparticles: A novel cancer therapeutic tool. Recent Advances in Drug Delivery and Formulation, 16(2): 84-89. https://doi.org/10.2174/2667387816666220506203123
[36] Younus, H. (2018). Therapeutic potentials of superoxide dismutase. International Journal of Health Sciences, 12(3): 88-93.
[37] Kozlov, A.V., Javadov, S., Sommer, N. (2024). Cellular ROS and antioxidants: Physiological and pathological role. Antioxidants, 13(5): 602. https://doi.org/10.3390/antiox13050602
[38] Rajashekar, C.B. (2023). Dual role of plant phenolic compounds as antioxidants and prooxidants. American Journal of Plant Sciences, 14(1): 15-28. https://doi.org/10.4236/ajps.2023.141002
[39] Buczyńska, A., Sidorkiewicz, I., Krętowski, A.J., Adamska, A. (2024). Examining the clinical relevance of metformin as an antioxidant intervention. Frontiers in Pharmacology, 15: 1330797. https://doi.org/10.3389/fphar.2024.1330797
[40] Bajpai, A., Verma, A.K., Srivastava, M., Srivastava, R. (2014). Oxidative stress and major depression. Journal of Clinical and Diagnostic Research, 8(12). https://doi.org/10.7860/JCDR/2014/10258.5292
[41] Del Rio, D., Stewart, A.J., Pellegrini, N. (2005). A review of recent studies on malondialdehyde as toxic molecule and biological marker of oxidative stress. Nutrition, Metabolism & Cardiovascular Diseases, 15: 316-328. https://doi.org/10.1016/j.numecd.2005.05.003
[42] Naik, S.R., Pilgaonkar, V.W., Panda V.S. (2006). Evaluation of antioxidant activity of Ginkgo biloba phytosomes in rat brain. Phytotherapy Research, 20(11): 1013-1016. https://doi.org/10.1002/ptr.1976
[43] Pernicova, I., Korbonits, M. (2014). Metformin--mode of action and clinical implications for diabetes and cancer. Nature Reviews Endocrinology, 10(3): 143-156. http://doi.org/10.1038/nrendo.2013.256
[44] Chen, J.W., Chen, Y.H., Lin, F.Y., Chen, Y.L., Lin, S.J. (2003). Ginkgo biloba extract inhibits tumor necrosis factor-α–induced reactive oxygen species generation, transcription factor activation, and cell adhesion molecule expression in human aortic endothelial cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 23(9): 1559-1566. http://doi.org/10.1161/01.ATV.0000089012.73180.63
[45] Abdul Kadhim, B.A., Ghafil, F.A., Majeed, S.A., Qassam H., Hadi, N.R. (2023). Hepato-protective effects of Silymarin against methotrexate-induced hepatotoxicity in rat model. Journal of Population Therapeutics & Clinical Pharmacology, 30(1): 373-382. https://doi.org/10.47750/jptcp.2023.1096
[46] Fulda, S., Gorman, A.M., Hori, O., Samali, A. (2010). Cellular stress responses: Cell survival and cell death. International Journal of Cell Biology, 2010(1): 214074. http://doi.org/10.1155/2010/214074
[47] Chen, J.W., Chen, Y.H., Lin, F.Y., Chen, Y.L., Lin, S.J. (2003). Ginkgo biloba extract inhibits tumor necrosis factor-α–induced reactive oxygen species generation, transcription factor activation, and cell adhesion molecule expression in human aortic endothelial cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 23(9): 1559-1566. https://doi.org/10.1161/01.ATV.0000089012.73180.63
[48] Majeed, H.M.S., Abbas, A.A.H., Khudair, M.S. (2022). The role of TNFα in type 2 diabetes mellitus. Revista Bionatura, 7(2): 32. https://doi.org/10.21931/RB/2022.07.02.32
[49] Isoda, K., Young, J.L., Zirlik, A., MacFarlane, L.A, Tsuboi, N., Gerdes, N., Schönbeck, U., Libby, P. (2006). Metformin inhibits proinflammatory responses and nuclear factor-κB in human vascular wall cells. Arteriosclerosis, Thrombosis, and Vascular Biology, 26(3): 611-617. http://doi.org/10.1161/01.ATV.0000201938.78044.75
[50] Achete de Souza, G., de Marqui, S.V., Matias, J.N., Guiguer, E.L., Barbalho, S.M. (2020). Effects on Ginkgo biloba on diseases related to oxidative stress. Planta Medica, 86(6): 376-386. https://doi.org/10.1055/a-1109-3405
[51] Mir, M.A., Albaradie, R.S. (2015). Immunomodulation of inflammatory markers in activated macrophages by leaf extracts of Ginkgo Biloba. Advances in Neuroimmune Biology, 6(1): 9-17. https://doi.org/10.3233/NIB-150103
[52] Lovelace, E.S., Wagoner, J., MacDonald, J., Bammler, T., et al. (2015). Silymarin suppresses cellular inflammation by inducing reparative stress signaling. Journal of Natural Products, 78(8): 1990-2000. https://doi.org/10.1021/acs.jnatprod.5b00288
[53] Kruk, A., Piwowarski, J.P., Pawłowska, K.A., Popowski, D., Granica, S. (2021). High molecular pyrogens present in plant extracts interfere with examinations of their immunomodulatory properties in vitro. Scientific Reports, 11(1): 799. http://doi.org/10.1038/s41598-020-79579-2
[54] Sochocka, M., Ochnik, M., Sobczyński, M., Gębura, K., Zambrowicz, A., Naporowski, P., Leszek, J. (2022). Ginkgo biloba leaf extract improves an innate immune response of peripheral blood leukocytes of Alzheimer's disease patients. Nutrients, 14(10): 2022. http://doi.org/10.3390/nu14102022
[55] Al Dubayee, M.S., Alayed, H., Almansour, R., Alqaoud, N., Alnamlah, R., Obeid, D., Alshahrani, A., Zahra, M.M., Nasr, A., Al-Bawab, A., Aljada, A. (2018). Differential expression of human peripheral mononuclear cells phenotype markers in Type 2 diabetic patients and Type 2 diabetic patients on metformin. Frontiers in Endocrinology, 9: 537. http://doi.org/10.3389/fendo.2018.00537
[56] Lee, Y., Lin, J., Chang, C., Chen, Y., et al. (2011). Ginkgo biloba extract suppresses endotoxin-mediated monocyte activation by inhibiting nitric oxide- and tristetraprolin-mediated toll-like receptor 4 expression. The Journal of Nutritional Biochemistry, 22(4): 351-359. https://doi.org/10.1016/j.jnutbio.2010.03.002
[57] Guo, Y., Wang, S., Wang, Y., Zhu, T. (2016). Silymarin improved diet-induced liver damage and insulin resistance by decreasing inflammation in mice. Pharmaceutical Biology, 54(12): 2995-3000. https://doi.org/10.1080/13880209.2016.1199042
[58] Cartes-Velásquez, R., Vera, A., Antilef, B., Sanhueza, S., Lamperti, L., González-Ortiz, M., Nova-Lamperti, E. (2024). Metformin restrains the proliferation of CD4+ T lymphocytes by inducing cell cycle arrest in normo- and hyperglycemic conditions. Biomolecules, 14(7): 846. https://doi.org/10.3390/biom14070846
[59] Cameron, A.R., Morrison, V.L., Levin, D., Mohan, M., et al. (2016). Anti-inflammatory effects of metformin irrespective of diabetes status. Circulation Research, 119(5): 652-665. http://doi.org/10.1161/CIRCRESAHA.116.308445
[60] Verbist, K.C., Klonowski, K.D. (2012). Functions of IL-15 in anti-viral immunity: Multiplicity and variety. Cytokine, 59(3): 467-478. https://doi.org/10.1016/j.cyto.2012.05.020
[61] Cheung, I.Y., Hsu, K., Cheung, N.K. (2012). Activation of peripheral-blood granulocytes is strongly correlated with patient outcome after immunotherapy with anti-GD2 monoclonal antibody and granulocyte-macrophage colony-stimulating factor. Journal of Clinical Oncology, 30(4): 426-432. http://doi.org/10.1200/JCO.2011.37.6236
[62] Boira, C., Chapuis, E., Scandolera, A., Reynaud, R. (2024). Silymarin alleviates oxidative stress and inflammation induced by UV and air pollution in human epidermis and activates β-endorphin release through cannabinoid receptor Type 2. Cosmetics, 11(1): 30. https://doi.org/10.3390/cosmetics11010030
[63] Cheng, D., Liang, B., Li, Y. (2013). Antihyperglycemic effect of Ginkgo biloba extract in streptozotocin-induced diabetes in rats. BioMed Research International, 2013(1): 162724. https://doi.org/10.1155/2013/162724
[64] Erices, R., Bravo, M.L., Gonzalez, P., Oliva, B., et al. (2013). Metformin, at concentrations corresponding to the treatment of diabetes, potentiates the cytotoxic effects of carboplatin in cultures of ovarian cancer cells. Reproductive Sciences, 20(12): 1433-1446. https://doi.org/10.1177/1933719113488441
[65] Wilasrusmee, C., Kittur, S., Shah, G., Siddiqui, J., Bruch, D., Wilasrusmee, S., Kittur, D.S. (2002). Immunostimulatory effect of Silybum Marianum (milk thistle) extract. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 8(11): BR439-43.
[66] Guo, X., Zhou, T., Xing, H., Zhang, Y., Fang, J., Kang, T., Yao, C., Yan, J., Huang, Y., Yao, Q. (2023). Antioxidant and in vivo hypoglycemic activities of ethanol extract from the leaves of Engelhardia roxburghiana wall, a comparative study of the extract and astilbin. Foods, 12(5): 927. https://doi.org/10.3390/foods12050927
[67] Nguyen, M.T.T., Hsu, I.C., Liu, H.K., Lin, Y.C., Chen, S.R., Chang, F.R., Cheng, Y.B. (2022). Components with anti-diabetic activity isolated from the leaves and twigs of Glycosmis pentaphylla collected in Vietnam. Pharmaceuticals, 15(12): 1543. https://doi.org/10.3390/ph15121543
[68] Lima, M.D.C., do Nascimento, H.M.A., da Silva, J.Y.P., de Brito Alves, J.L., de Souza, E.L. (2023). Evidence for the beneficial effects of Brazilian native fruits and their by-products on human intestinal microbiota and repercussions on non-communicable chronic diseases—A review. Foods, 12(18): 3491. https://doi.org/10.3390/foods12183491
[69] Aziz, T.A. (2021). The role of Ginkgo biloba extract as monotherapy in improving the outcomes of patients with metabolic syndrome: A pilot comparative study with metformin. Iraqi Journal of Pharmaceutical Sciences, 30(1): 258-269. https://doi.org/10.31351/vol30iss1pp258-269