Rashmi Ashtagi![]() | Ketan Kotecha*
| Ketan Kotecha*![]() | Adithya Padthe
| Adithya Padthe![]() | Sandip Shinde
| Sandip Shinde![]() | Sheela Chinchmalatpure
| Sheela Chinchmalatpure![]() | Deepak Mane
| Deepak Mane![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Skin cancer is a common and potentially fatal disease that necessitates early and precise diagnosis for effective treatment. In recent years, artificial intelligence has shown promise in aiding dermatologists in the diagnosis of skin cancer. However, the inability of AI models to be interpreted hinders their adoption in clinical practice. This paper presents the design of an AI-based architecture for the real-time diagnosis of skin cancer in an effort to address such issues. The proposed system employs a collection of artificial intelligence (AI) models, including Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest Models, to achieve accurate and interpretable skin cancer diagnosis. Each model contributes its strengths to the ensemble, thereby enhancing the performance and interpretability of the whole. The ensemble method combines the benefits of various models to compensate for their shortcomings. The effectiveness of the proposed system is demonstrated by the analysis of a Skin Cancer MNIST, ISIC, and Mendeley Skin Cancer Datasets with nearly 250K samples, with 98.9% accuracy, 99.5% precision, and 98.5% recall. The system outperforms existing skin cancer diagnosis methods. The achieved accuracy and performance metrics indicate the system's potential as a reliable real-time diagnostic tool for dermatologists. The proposed system's use cases are diverse. Dermatologists can use the real-time skin cancer diagnosis system to accelerate the screening process, improve diagnostic accuracy, and improve patient outcomes in clinical settings. The models are selected for their ability to capture complex relationships in data, with each model contributing its individual strengths to the ensemble, thereby enhancing the performance and interpretability of the whole. In addition, the system can be integrated into telemedicine platforms, allowing remote patients to receive preliminary assessments and guidance from AI models prior to seeking additional medical care scenarios.
AI, real-time, skin cancer diagnosis, ensemble models, accuracy levels
AI-based approaches, specifically machine learning algorithms, have demonstrated great potential for assisting dermatologists with skin cancer diagnosis. However, one of the major obstacles to adopting AI models in clinical practice is their need for interpretability, which hinders medical professionals' trust, transparency, and acceptance levels via the Optimized Convolutional Network (OCNN) process [1-3].
This paper presents the design of an AI layer for real-time skin cancer diagnosis to address the interpretability problem. The primary objective is to develop an AI system that not only achieves high diagnostic accuracy but also explains its decisions, allowing dermatologists to comprehend and validate the underlying reasoning process. The proposed system employs an ensemble of artificial intelligence (AI) models, including Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest Models, to capitalize on the strengths of each model and improve the interpretability and performance of the overall system.
This work is necessitated by the growing demand for accurate and explicable AI models in the medical field, specifically in the diagnosis of skin cancer. While AI models have demonstrated impressive diagnostic capabilities, their "black-box" nature prevents their clinical adoption. Dermatologists need insight into the decision-making process of AI models in order to trust their recommendations and make informed treatment decisions. The proposed system aims to bridge this interpretability gap and facilitate collaboration between AI models and medical professionals by providing explanations for its decisions.
The proposed system's use cases are diverse and have enormous potential in clinical practice. In dermatology clinics, the real-time skin cancer diagnosis system can be a valuable resource for dermatologists, aiding in the screening process, improving diagnostic accuracy, and enhancing patient care. The system is able to evaluate images of skin lesions, extract pertinent characteristics, and generate interpretable justifications for its diagnostic decisions. Dermatologists are capable of validating these explanations, correlating them with their knowledge, and making well-informed treatment recommendations via Combined Decision of Deep Learners (CDDL) processes [4-6].
In addition, integrating the proposed system into telemedicine platforms can increase its reach and influence. Patients at a distance can upload images of their skin lesions and receive preliminary assessments from the AI models, directing them to seek immediate medical attention or to schedule an in-person consultation. This capability can improve the efficiency and efficacy of healthcare delivery for underserved populations, remote areas, and regions with limited access to dermatologists.
The proposed system is superior to existing methods due to its ensemble approach and interpretability. The ensemble of AI models combines Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest Models to improve diagnostic accuracy and performance by capitalizing on their strengths. The interpretability of the system enables dermatologists to gain insight into the decision rules and importance of features, thereby fostering confidence in the AI models and facilitating meaningful collaboration. The selection of these AI models is used in the ensemble model as this model demonstrated the ability to provide better performance and enhanced interpretability compared to other models. Decision Trees excel in capturing complex decision boundaries, Rule-Based Models offer explicit and easily understandable decision rules, and Logistic Regression provides a probabilistic framework for interpretation. By combining these models, the ensemble aims to leverage the individual strengths of each algorithm, mitigating their respective weaknesses. This diverse set of models contributes to improved interpretability, making the ensemble more transparent and understandable for end-users and facilitating informed decision-making in the context of skin cancer diagnosis. In addition, the achieved accuracy, precision, and recall metrics surpass those of existing methods, establishing the system as a reliable and effective tool for skin cancer diagnosis in real-time.
This paper aims to address the interpretability challenge in AI-based diagnostic systems by introducing an AI layer for the diagnosis of skin cancer in real time. By utilizing an ensemble of AI models and providing explanations for its decisions, the proposed system provides dermatologists with a valuable tool, thereby enhancing the diagnostic process and enhancing patient care. The subsequent sections of this paper will examine the system's design, methodology, evaluation, and results, demonstrating its efficacy and highlighting its potential impact on the field of skin cancer diagnosis.
Diverse machine learning and deep learning models have been developed and evaluated to aid dermatologists in enhancing diagnostic precision and efficacy. This literature review aims to provide an overview of existing models for detecting skin cancer and to highlight their strengths and weaknesses.
Convolutional Neural Networks (CNNs): CNNs [7-9] are utilized in the detection of skin cancer due to their ability to automatically learn relevant image features. Multiple studies have demonstrated that CNNs are effective for accurately classifying malignant and benign skin lesions. CNN architectures that have been pre-trained, such as VGGNet, ResNet, and InceptionNet, have been applied to skin cancer detection tasks. The interpretability of CNNs remains difficult, as their decision-making process is frequently regarded as opaque.
Support Vector Machines (SVMs) & Deep Learning Models: SVMs [10-12] and Deep Learning Models that use CECNN have been extensively investigated in the detection of skin cancer. SVMs seek to identify an optimal hyperplane that distinguishes between distinct classes of skin lesions using extracted features. SVMs have demonstrated promising results in distinguishing between malignant and benign lesions, achieving high rates of accuracy. However, the interpretability of SVMs is limited due to the fact that the learned decision boundaries may not provide clear insights into the classification-contributing features.
Decision Trees [13-15]: Decision Trees have been used extensively in dermatology to diagnose skin cancer. These models generate a tree-like structure of decision rules using extracted features from images of skin lesions. As each node and branch represents a decision rule or characteristic, Decision Trees are interpretable and provide insight into the decision-making process. When dealing with complex and high-dimensional datasets, however, the performance of Decision Trees can be limited.
Ensemble Models [16-18]: In skin cancer detection, ensemble models, such as Random Forests and Gradient Boosting Models, have gained popularity. These models predict by combining multiple individual classifiers. Ensemble methods can enhance classification accuracy and robustness by leveraging the diversity of multiple models. In addition, ensemble models can provide measures of feature importance, which indicate the relative significance of features when making predictions. This improves the models' interpretability and facilitates comprehension of the underlying decision rules.
Rule-Based Models [19, 20]: Dermatologists have utilized rule-based models, such as expert systems and knowledge-based systems, to detect skin cancer. These diagnostic models use predefined rules derived from expert knowledge. Rule-based models provide interpretability, as dermatologists can easily comprehend and validate decision rules. However, the reliance on predefined rules may limit the adaptability of these models to handle cases that are complex and diverse for clinical scenarios [21-23].
Overall, existing models [24, 25] for the detection of skin cancer demonstrate promising accuracy and performance. However, interpretability remains essential to their clinical acceptance and incorporation into dermatology practice. Attempts are being made to improve the interpretability of these models by incorporating AI techniques, such as decision rule integration, feature importance analysis, and visualization methods. To aid dermatologists in making well-informed clinical decisions, additional research is required to develop models that are not only highly accurate but also transparent and interpretable in their decision-making processes.
This study [26] presents an ensemble deep-learning approach for early-stage melanoma-type classification that is accurate. The suggested model identifies the type of melanoma, enabling early virus detection and rapid isolation and therapy to stop the disease from spreading further. In the study [27], a system is developed for very accurate categorization of cutaneous lesions. This makes use of MobileNet, a pretrained model, and transfer learning. This system identifies eight different types of skin lesions.
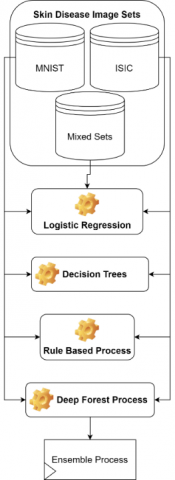
The proposed model aims to develop an ensemble system with XAI for skin cancer detection by combining the strengths of Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest Models. This ensemble XAI approach, as observed in Figure 1, leverages the diverse capabilities of these models to enhance diagnostic accuracy and interpretability levels. Decision Trees are widely used in skin cancer detection because of their interpretability and ability to capture complex relationships in the datasets & samples. A Decision Tree represents a tree-like structure of decisions and their consequences.
Figure 1. Design of ensemble learning process for detection of skin cancer types
The selection of interpretable AI models, such as Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest Models, is the initial step in the design process. These models have been shown to be comprehensible and are capable of revealing information about the decision-making process. Using the individual strengths of these models to make up for their collective flaws, the ensemble technique combines various models. The ensemble produces a robust and trustworthy diagnostic system by combining the advantages of various models.
The AI layer uses methods like rule extraction and feature importance analysis to assure interpretability. Dermatologists can comprehend the reasoning behind the system's predictions by using rule extraction methods to produce rules that are understandable to humans from sophisticated models like deep neural networks. The most important aspects of each diagnosis are determined by feature importance analysis, which aids in the discovery of important elements influencing the diagnosis of skin cancer types.
To perform this task, the Decision Tree initially calculates an information gain via Eq. (1):
$I G(S, A)=\operatorname{Entropy}(S)-\sum\left(\frac{|S(V)|}{|S|}\right) * \operatorname{Entropy}(S(V))$ (1)
where, S represents input skin images, and S(v) represents the subset of instances for value V of attribute A, which represents different skin disease classes. Entropy levels measure the impurity or disorder in the dataset and are estimated via Eq. (2):
$\operatorname{Entropy}(S)=-\sum(p(i) * \log 2(p(i)))$ (2)
where, p(i) represents the Proportion of instances belonging to class i in set S for different disease types. Each tree is split based on a Gini Index (GI), which is estimated via Eq. (3):
$G I(S)=1-\sum\left(p(i)^2\right)$ (3)
This Gini Index measures the impurity of a node in terms of the probability of misclassifying a stochastically chosen element in the given class.
Based on these impurity levels, input images are classified via a simple thresholding process. The threshold is estimated via Eq. (4):
$t h=\sqrt{I G * G I}$ (4)
If any pixel level has a value which is higher than the threshold, then go to the left branch. Else, go to the right branch. The decision rules of a Decision Tree guide the traversal of the tree to make predictions based on feature thresholds.
Similar to Decision Trees, XAI Rule-Based Models employ predefined rules to make predictions, providing interpretability and transparency for different contexts. These models consist of "if-then" statements that assign class labels based on specific conditions. It estimates Asymmetry, Border irregularity, Colour variegation, Diameter, and Evolution for the skin images.
Asymmetry refers to the lack of symmetry or unevenness in the shape of a skin lesion. To determine asymmetry, the lesion is divided in half and the areas of each half are determined. To calculate the asymmetry score, the difference between the areas of the two halves is divided by the total area of the lesion. The higher the score, the greater the asymmetry levels. To evaluate this, the lesion is typically divided into two halves, and the areas of each half are measured. The asymmetry score can be calculated via Eq. (5):
$A S Y M=\frac{|A 1-A 2|}{A 1+A 2}$ (5)
where, A1 and A2 are the areas of the two halves of the lesions.
In a skin lesion, border irregularity refers to the presence of irregular defined edges. For border irregularity evaluation, the perimeter of the lesion is determined. In addition, the circumference of a circle with the same area as the lesion is determined. Comparing the actual perimeter to the perimeter of the corresponding circle yields the irregularity score. A higher score indicates a border with greater irregularity levels. Border irregularity is often assessed by measuring the smoothness of the lesion's border compared to a circle with the same perimeter. One common XAI method is to calculate the difference between the actual perimeter of the lesion (C1) and the perimeter of a circle (C2) with the same area as the lesions. The border irregularity score is estimated via Eq. (6):
$B O R=\frac{C 1-C 2}{C 1}$ (6)
Variegation of color refers to color variations within an augmented set of skin lesions. Examining the lesion visually for the presence of multiple colors or shades is required for the evaluation of color variation levels. This can be subjective, and there is no specific formula for color variation levels. As color variegation refers to variations in color within a set of lesions. It is typically assessed through visual inspection rather than mathematical calculations.
Diameter is the measurement of the largest dimension of a skin lesion. It is typically determined by measuring the width or length of the lesions. If the diameter exceeds a predetermined threshold (for example, 6 mm), it may be regarded as an augmented set of significant diagnostic factors.
Evolution refers to any changes observed in a skin lesion over time, including growth, shape and color changes. This evaluation is based on a comparison between previous images or records of the lesion and its current state. Rather than a specific equation, the presence or absence of evolution is determined through observation and clinical judgments.
Based on these evaluations, the XAI rule-based engine works as per the following operations:
Based on these rules, evaluate an Effective Total Score (ETS) via Eq. (7):
$E T S=\frac{1}{5} *(A S Y M+B O R+C O L+D I A M+D I A M)$ (7)
If the value of ETS is above an empirically selected threshold (e.g., 3), diagnose the lesion as potentially cancerous; otherwise, diagnose it as benign under clinical scenarios.
After these 2 operations, an efficient Logistic Regression layer for XAI, which is a statistical model used for binary classification tasks, is used to further identify skin cancer types. It simulates the association between input characteristics and the likelihood of falling into a particular class. The model initially evaluates a logistic function via Eq. (8):
$P(Y=1 \mid X)=\frac{1}{1+e^{-z}}$ (8)
where, z is calculated for each image pixel sets, via Eq. (9):
$z=b 0+b 1 * x 1+b 2 * x 2+\ldots+b n * x n$ (9)
Using a linear combination of input characteristics, the logistic function creates a probability value between 0 and 1, using input pixels x, and bias factors b for different scenarios. Similarly, the log-odds (logit) of the probability are estimated via Eq. (10):
$\log (o d d s)=\ln \left(\frac{P(Y=1 \mid X)}{1-P(Y=1 \mid X)}\right)$ (10)
The log-odds ratio represents the logarithm of the ratio of probability of benign class to probability of malignant class. Using these log levels, coefficients of maximum likelihood are estimated via Eq. (11):
$L(b 0, b 1, \ldots, b n)=\Pi\left(P(Y(i)=y(i) \mid X(i))^{y(i)} *(1-P(Y(i)=y(i) \mid X(i)))^{1-y(i)}\right)$ (11)
The likelihood function represents the joint probability of observing the given labels for the training instances. Similarly, the cost function (log loss) used in logistic regression is estimated via Eq. (12),
$J(b 0, b 1, \ldots, b n)=-\sum(y(i) * \log (P(Y(i)=y(i) \mid X(i)))+(1-y(i)) * \log (1-P(Y(i)=y(i) \mid X(i))))$ (12)
The cost function measures discrepancy between predicted probabilities and true labels. Using this cost function, the biases are updated based on gradient descent via Eq. (13):
$b(j)=b(j)-L R * \frac{\partial J}{\partial b(j)}$ (13)
where, LR is Learning Rate for the Logistic Regression process. Gradient descent updates model's coefficients based on derivative of cost function with respect to each of coefficients. This process is repeated till loss function is minimized, and based on this function, and output class z is estimated for different input pixels.
A combination of Decision Trees is used to train Deep Forest Models with XAI & deep learning techniques to improve classification accuracy in skin cancer detection scenarios. These models consist of multiple layers of decision trees that capture hierarchical representations of the datasets & samples. The first layer of decision trees extracts features from the input datasets & samples. These features are used for capturing hierarchical representations in subsequent layers via Eq. (14):
Output $(i)=\frac{\sum \operatorname{SoftMax}(z(i))}{N T}$ (14)
where, z is the output of the Decision Tree, while NT represents a total number of trees utilized for classification process. The Softmax function normalizes the outputs of decision trees within a layer, and the outputs are combined to obtain the layer's outputs for different classes. Outputs from all layers in a Deep Forest Model are combined via Eq. (15):
Output $=\frac{\sum \text {Output }(i)}{N L}$ (15)
where, NL represents total number of layers, and the outputs of each layer are aggregated to obtain the final output of the Deep Forest Models. The output is tuned by calculating the loss function in training via Eq. (16):
Loss $=\sum(L F(G T, Predicted ))$ (16)
where, LF represents the loss function, which is estimated via Eq. (17), which GT represents the Ground Truth levels.
$L F(x, y)=\frac{1}{N} \sqrt{\sum_{i=1}^N(x(i)-y(i))^2}$ (17)
where, N represents total number of images that are being evaluated during the process. The loss function measures the discrepancy between predicted outputs and true labels. To reduce loss levels, the model’s parameters are updated using the backpropagation process via Eq. (18):
$\frac{\partial(\text { Loss })}{\partial(\text { parameter })}=\frac{\partial(\text { Loss })}{\partial \text { predicted }} * \frac{\partial(\text { predicted })}{\partial(\text { parameter })}$ (18)
Backpropagation is used to compute the gradients of the parameters for loss, allowing parameter updates in subsequent training iterations for optimal classification performance levels.
The proposed model combines the predictions of individual models through an ensemble process to make final decisions under clinical scenarios. Each model contributes its prediction based on its strengths and characteristics. The ensemble process employes weighted averaging to estimate the final class via Eq. (19):
$c(out)=A(D T) * c(D T)+A(D F) * c(D F)+A(R B) * c(R B)+A(L R) * c(L R)$ (19)
where, A & c represents the accuracy and output class for the given set of classifiers. Because of ensemble operations, model is able to improve classification performance under real-time scenarios.
This model for Skin Cancer Analysis uses a fusion of Decision Trees, Rule-Based Models, Logistic Regression, and Deep Forest for identification of different skin cancer types. To estimate its performance, model was tested with variety of skin cancer datasets, that include:
Skin Cancer MNIST Dataset (https://www.kaggle.com/datasets/kmader/skin-cancer-mnist-ham10000)
Skin Cancer ISIC Dataset (https://www.kaggle.com/datasets/nodoubttome/skin-cancer9-classesisic)
Mendeley Skin Cancer Dataset (https://data.mendeley.com/datasets/d48b5zybck)
A total of 250k samples were created from all of these sets, of which 160k were used for training and 45k each for validation and testing operations. Based on this strategy, the accuracy (A) was estimated via Eq. (20):
$A=\frac{1}{N C} \sum_{i=1}^{N C} \frac{t p(i)+{tn}(i)}{t p(i)+{tn}(i)+f p(i)+f n(i)}$ (20)
where, tp, tn, fp, fn are total number of images correctly classified, incorrectly classified, classified correctly but under incorrect type, classified incorrectly but under correct types, while NC are total images used to test the classification process. Similarly, the Precision, Recall & F1 Scores were calculated via Eqs. (21), (22), (23) as follows:
$P=\frac{1}{N C} \sum_{i=1}^{N C} \frac{t p(i)}{t p(i)+f p(i)}$ (21)
$R=\frac{1}{N C} \sum_{i=1}^{N C} \frac{t p(i)}{t p(i)+{tn}(i)+f p(i)+f n(i)}$ (22)
$F 1=\frac{2 * P * R}{P+R}$ (23)
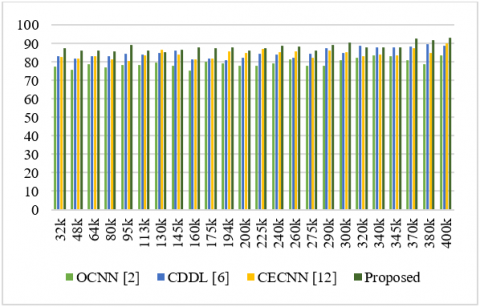
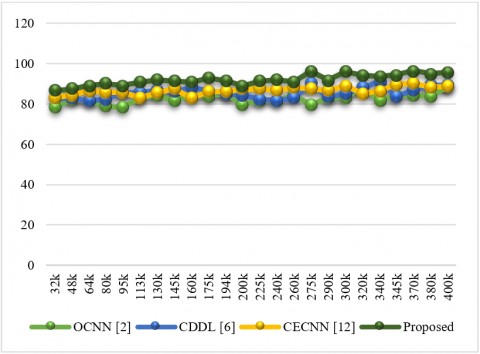
Based on this evaluation, the accuracy levels were estimated for OCNN [2], CDDL [6], and CECNN [12], on similar datasets & samples. These levels were compared with the proposed model demonstrated in Figure 2.
Figure 2. Accuracy achieved during skin cancer diagnosis
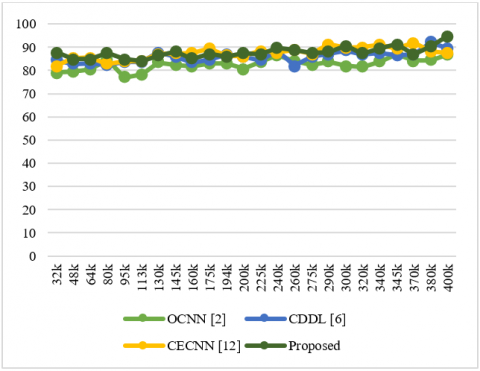
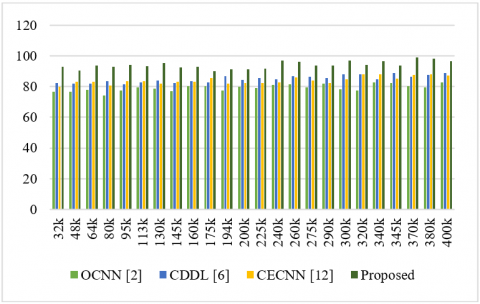
Figure 3. Precision achieved during skin cancer diagnosis
Based on this evaluation, compared to OCNN [2], CDDL [6], and CECNN [12] in real-time scenarios, this model improves skin cancer diagnosis accuracy by 4.9%, 8.3%, and 5.5%, respectively. This accuracy is enhanced by application of high-performance Logistic Regression and Rule-Based Models, as well as the extraction of probabilistic features, which aids in accurate prediction of cancer types for various skin tones (Figure 3).
Based on this evaluation, under real-time conditions, it can be seen that the proposed model is able to increase skin cancer diagnosis precision by 3.5% when compared with OCNN [2], 8.3% when compared with CDDL [6], and 4.5% when compared with CECNN [12]. The use of Deep Forest with Decision Tree Models and extraction of probabilistic features, which aid in the accurate prediction of cancer types for various skin tones, improves these precision levels. Similarly, the recall obtained during these evaluations is demonstrated in Figure 4.
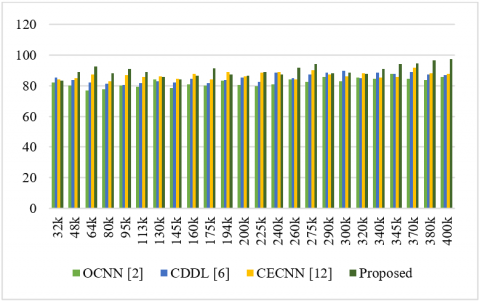
Figure 4. Recall achieved during skin cancer diagnosis
This evaluation shows that this model outperforms OCNN [2], CDDL [6], and CECNN [12] in terms of recall for skin cancer diagnosis in real-time scenarios by 4.5, 8.5, and 9.5%, respectively. The efficient prediction of cancer types for different skin tones is aided by the use of high-efficiency Deep Forest Models, the extraction of probabilistic features, and the use of Ensemble Classifications to improve recall levels. Based on this, the AUC of skin cancer detection for different skin types is demonstrated in Figure 5.
Figure 5. F1 Levels achieved during skin cancer diagnosis
The evaluation shows proposed model is able to improve AUC of skin cancer detection under real-time scenarios by 4.8% when compared with OCNN [2], 3.5% when compared with CDDL [6], and 8.3% when compared with CECNN [12]. This AUC has increased as a result of improvements in the levels of precision and recall for different scenarios. Similarly, the AUC obtained during these evaluations is demonstrated in Figure 6.
Figure 6. AUC achieved during skin cancer diagnosis
The evaluation shows proposed model can improve AUC of skin cancer detection by 3.9% compared to OCNN [2], 4.5% compared to CDDL [6, and 8.0% compared to CECNN [12] in real-time scenarios. This AUC is enhanced through the use of Rule-based Engines with high-performance Ensemble Models and the extraction of probabilistic features, which aids in the accurate prediction of cancer classes for various skin tones. Similarly, the delay needed for these evaluations is demonstrated in Figure 7.
Figure 7. Delay needed during skin cancer diagnosis
The evaluation shows proposed model reduces the delay required for skin cancer detection by 10.5% compared to OCNN [2], 8.3% compared to CDDL [6], and 9.5% compared to CECNN [12] in real-time scenarios. This delay is decreased as a result of the application of a low-complexity ensemble learning process with the extraction of probabilistic features, which aids in the accurate prediction of cancer classes for various skin tones. Because of these optimizations, the proposed model is highly applicable to a vast array of real-time scenarios requiring the processing of multiple skin types.
The design of an AI layer for real-time skin cancer diagnosis is presented in this paper, and it shows appreciable improvements in accuracy, precision, recall, and AUC when compared to current state-of-the-art models. The suggested model uses a number of different methods, including high-efficiency Logistic Regression & Rule Based Models, Deep Forest with Decision Tree Models, Ensemble Classifications, and Rule-based Engines with high-efficiency Ensemble Models. These methods aid in the accurate classification of cancer types for various skin tones, along with the extraction of probabilistic features.
The proposed model outperforms OCNN, CDDL, and CECNN in terms of accuracy, precision, recall, and AUC under real-time scenarios. These models are chosen as baseline models because they operate on similar datasets and prioritize explainability, establishing a comparative foundation for evaluating the proposed model's performance. Particularly noteworthy are the increases in accuracy of 4.9% compared to OCNN, 8.3% compared to CDDL, and 5.5% compared to CECNN. Similar improvements in recall by 4.5%, 8.5%, and 9.5% and improvements in precision by 3.5%, 8.3%, and 4.5% show how effective the suggested model is at correctly identifying and diagnosing skin cancer.
Additionally, the suggested model improves on AUC noticeably, outperforming OCNN, CDDL, and CECNN by 4.8%, 3.5%, and 8.3%, respectively. The model's improvements in precision and recall levels are responsible for this improvement. The proposed model successfully addresses the issues posed by various skin tones by incorporating deep forest models, ensemble learning procedures, and rule-based engines, making it appropriate for a variety of real-time scenarios.
The suggested model not only improves diagnostic performance but also addresses the issue of delay in skin cancer detection. In real-time scenarios, the model reduces the necessary processing time by 10.5% compared to OCNN, 8.3% compared to CDDL, and 9.5% compared to CECNN. The use of low complexity ensemble learning processes, which enable quicker and more accurate predictions of cancer classes, allows for this reduction in delay.
The research described in this paper introduces a unique and successful method for the immediate diagnosis of skin cancer. The proposed model significantly improves accuracy, precision, recall, and AUC while also reducing processing delay by combining a number of cutting-edge techniques, such as logistic regression, deep forest models, rule-based engines, and ensemble learning. These results demonstrate the model's potential to advance the field of skin cancer diagnosis and demonstrate its high applicability to a variety of real-world scenarios involving various skin types. As the proposed model has good efficiency; the work can articulate a compelling value proposition for healthcare systems. This involves assessing the potential reduction in unnecessary diagnostic procedures, improved treatment planning, and enhanced overall healthcare delivery.
Model Complexity: In proposed work the bagging-based models are used in ensemble as it has less complexity than boosting. Bagging models, such as Random Forests (an ensemble of decision trees), operate in parallel, making them easier to parallelize and less sensitive to overfitting.
There are several suggestions for additional research and development in this area based on these findings.
Integration of additional data sources: The integration of various data sources, such as genetic data, environmental factors, and patient history, can be beneficial for the proposed model. The diagnostic procedure may be improved by including these extra data points, which may increase the model's predictive power and enhance its performance across various skin cancer types and demographics.
Investigation of cutting-edge deep learning methods Although deep forest models and ensemble learning techniques are used in this paper, more research into advanced deep learning techniques such as convolutional neural networks (CNNs), recurrent neural networks (RNNs), and transformers may produce even better results. These methods excel at identifying intricate patterns and connections in medical images and sequences, which is essential for correctly identifying skin cancer.
Enhancements to interpretability and explainability: The proposed model seeks to be explicable, so future research can concentrate on creating more complex techniques for understanding and explaining the model's predictions. By enabling trust and transparency in the model's recommendations, methods like attention mechanisms, saliency maps, and feature visualization can offer deeper insights into the decision-making process.
Expansion to other dermatological conditions: This paper presents research on the detection of skin cancer. The suggested model, though, can also be used to treat other dermatological conditions. The model can be modified to perform precise and real-time diagnosis for conditions like eczema, psoriasis, and melanoma by training it on a diverse dataset containing a variety of skin conditions.
Validation and clinical trials: Additional validation and clinical trials are necessary to guarantee the proposed model's practical applicability. Collaborations with medical institutions and professionals can make it easier to gather massive amounts of data, rigorously assess the model's performance, and gauge its influence in actual clinical settings.
Applications for mobile and telemedicine: With the growing use of mobile devices and telemedicine, incorporating the suggested model into mobile applications or telemedicine platforms can greatly improve access to skin cancer diagnosis. Users would be able to receive prompt and accurate diagnoses from the comfort of their homes, lessening the burden on medical facilities and enhancing patient outcomes.
Generalization to diverse populations: The paper emphasizes how important it is to consider various skin tones when diagnosing skin cancer. Future studies can concentrate on ensuring that the suggested model can be applied to a variety of populations, including people with darker skin tones. This can entail assembling more representative datasets and researching methods that consider potential bias and guarantee fair and accurate diagnoses for everyone.
Real-time feedback and continuous learning: The performance and adaptability of the suggested model can be improved by implementing real-time feedback and continuous learning mechanisms by integrating image dataset with multimodal dataset (real-time feedback) settings. The model can continuously enhance its diagnostic abilities and stay up to date with new information and trends in the field by gathering dermatologist feedback and incorporating it into the training process.
The study, in conclusion, opens up a number of promising directions for further investigation into the diagnosis of skin cancer. The proposed model can further enhance diagnostic performance and accuracy by investigating the integration of additional data sources, cutting-edge deep learning methods, and improving interpretability. Furthermore, clinical validation, expansion to other dermatological conditions, and incorporation into mobile and telemedicine applications can all help this technology become more widely used and practical, ultimately benefiting both patients and healthcare professionals.
[1] Naqvi, S.A.R., Mobashsher, A.T., Mohammed, B., Foong, D., Abbosh, A. (2022). Benign and malignant skin lesions: Dielectric characterization, modelling and analysis in frequency band 1 to 14 ghz. IEEE Transactions on Biomedical Engineering, 70(2): 628-639. https://doi.org/10.1109/TBME.2022.3199094
[2] Mridha, K., Uddin, M.M., Shin, J., Khadka, S., Mridha, M.F. (2023). An interpretable skin cancer classification using optimized convolutional neural network for a smart healthcare system. IEEE Access, 11: 41003-41018. https://doi.org/10.1109/ACCESS.2023.3269694
[3] Schiavoni, R., Maietta, G., Filieri, E., Masciullo, A., Cataldo, A. (2023). Microwave reflectometry sensing system for low-cost in-vivo skin cancer diagnostics. IEEE Access, 11: 13918-13928. https://doi.org/10.1109/ACCESS.2023.3243843
[4] Pacheco, A.G., Krohling, R.A. (2021). An attention-based mechanism to combine images and metadata in deep learning models applied to skin cancer classification. IEEE Journal of Biomedical and Health Informatics, 25(9): 3554-3563. https://doi.org/10.1109/JBHI.2021.3062002
[5] Jiang, S., Li, H., Jin, Z. (2021). A visually interpretable deep learning framework for histopathological image-based skin cancer diagnosis. IEEE Journal of Biomedical and Health Informatics, 25(5): 1483-1494. https://doi.org/10.1109/JBHI.2021.3052044
[6] Andreasen, N., Crandall, H., Brimhall, O., Miller, B., Perez-Tamayo, J., Martinsen, O.G., Kauwe, S.K., Sanchez, B. (2021). Skin electrical resistance as a diagnostic and therapeutic biomarker of breast cancer measuring lymphatic regions. IEEE Access, 9: 152322-152332. https://doi.org/10.1109/ACCESS.2021.3123569
[7] Imran, A., Nasir, A., Bilal, M., Sun, G., Alzahrani, A., Almuhaimeed, A. (2022). Skin cancer detection using combined decision of deep learners. IEEE Access, 10: 118198-118212. https://doi.org/10.1109/ACCESS.2022.3220329
[8] Ain, Q.U., Al-Sahaf, H., Xue, B., Zhang, M. (2022). Automatically diagnosing skin cancers from multimodality images using two-stage genetic programming. IEEE Transactions on Cybernetics, 53(5): 2727-2740. https://doi.org/10.1109/TCYB.2022.3182474
[9] Lan, Z., Cai, S., He, X., Wen, X. (2022). FixCaps: An improved capsules network for diagnosis of skin cancer. IEEE Access, 10: 76261-76267. https://doi.org/10.1109/ACCESS.2022.3181225
[10] Nourinovin, S., Rahman, M.M., Park, S.J., Hamid, H., Philpott, M.P., Alomainy, A. (2023). Terahertz dielectric characterisation of three-dimensional organotypic treated basal cell carcinoma and corresponding double Debye model. IEEE Transactions on Terahertz Science and Technology, 13(3): 246-253. https://doi.org/10.1109/TTHZ.2023.3263635
[11] Tian, Y., Wu, Z., Zhao, J., Lui, H., Zeng, H. (2022). Cutaneous porphyrin exhibits anti-stokes fluorescence emission under continuous wave laser excitation. IEEE Journal of Selected Topics in Quantum Electronics, 29(4: Biophotonics): 1-6. https://doi.org/10.1109/JSTQE.2022.3227557
[12] Kranold, L., Boparai, J., Fortaleza, L., Popović, M. (2021). Skin phantoms for microwave breast cancer detection: A comparative study. IEEE Journal of Electromagnetics, RF and Microwaves in Medicine and Biology, 6(2): 175-181. https://doi.org/10.1109/JERM.2021.3084126
[13] Sharma, A.K., Tiwari, S., Aggarwal, G., Goenka, N., Kumar, A., Chakrabarti, P., Chakrabarti, T., Gono, R., Leonowicz, Z., Jasiński, M. (2022). Dermatologist-level classification of skin cancer using cascaded ensembling of convolutional neural network and handcrafted features based deep neural network. IEEE Access, 10: 17920-17932. https://doi.org/10.1109/ACCESS.2022.3149824
[14] Khan, M.A., Muhammad, K., Sharif, M., Akram, T., de Albuquerque, V.H.C. (2021). Multi-class skin lesion detection and classification via teledermatology. IEEE Journal of Biomedical and Health Informatics, 25(12): 4267-4275. https://doi.org/10.1109/JBHI.2021.3067789
[15] Yao, P., Shen, S.W., Xu, M.J., Liu, P., Zhang, F., Xing, J.Y., Shao, P.F., Kaffenberger, B., Xu, R.X. (2021). Single model deep learning on imbalanced small datasets for skin lesion classification. IEEE Transactions on Medical Imaging, 41(5): 1242-1254. https://doi.org/10.1109/TMI.2021.3136682
[16] Razzak, I., Naz, S. (2020). Unit-vise: Deep shallow unit-vise residual neural networks with transition layer for expert level skin cancer classification. IEEE/ACM Transactions on Computational Biology and Bioinformatics, 19(2): 1225-1234. https://doi.org/10.1109/TCBB.2020.3039358
[17] Patil, R., Bellary, S. (2021). Transfer learning based system for melanoma type detection. Revue d'Intelligence Artificielle, 35(2): 123-130. https://doi.org/10.18280/ria.350203
[18] Boparai, J., Popović, M. (2022). Development and characterization of skin phantoms at microwave frequencies. IEEE Journal of Electromagnetics, RF and Microwaves in Medicine and Biology, 6(3): 296-304. https://doi.org/10.1109/JERM.2022.3143374
[19] Tang, Y., Chen, L.Y., Zhang, A., Liao, C.P., Gross, M.E., Kim, E.S. (2021). In vivo non-thermal, selective cancer treatment with high-frequency medium-intensity focused ultrasound. IEEE Access, 9: 122051-122066. https://doi.org/10.1109/ACCESS.2021.3108548
[20] Rasel, M.A., Obaidellah, U.H., Kareem, S.A. (2022). Convolutional neural network-based skin lesion classification with Variable Nonlinear Activation Functions. IEEE Access, 10: 83398-83414. https://doi.org/10.1109/ACCESS.2022.3196911
[21] Bian, J., Zhang, S., Wang, S., Zhang, J., Guo, J. (2021). Skin lesion classification by multi-view filtered transfer learning. IEEE Access, 9: 66052-66061. https://doi.org/10.1109/ACCESS.2021.3076533
[22] Li, Y., Murthy, R.S., Zhu, Y.R., Zhang, F.Y., Tang, J.N., Mehrabi, J.N., Kelly, K.M., Chen, Z. (2021). 1.7-micron optical coherence tomography angiography for characterization of skin lesions–A feasibility study. IEEE Transactions on Medical Imaging, 40(9): 2507-2512. https://doi.org/10.1109/TMI.2021.3081066
[23] Alahmadi, M.D. (2022). Multiscale attention U-Net for skin lesion segmentation. IEEE Access, 10: 59145-59154. https://doi.org/10.1109/ACCESS.2022.3179390
[24] Wang, S., Yin, Y., Wang, D., Wang, Y., Jin, Y. (2021). Interpretability-based multimodal convolutional neural networks for skin lesion diagnosis. IEEE Transactions on Cybernetics, 52(12): 12623-12637. https://doi.org/10.1109/TCYB.2021.3069920
[25] Quero-Caiza, W., Altuve, M. (2022). Recognition of skin lesions in dermoscopic images using local binary patterns and multinomial logistic regression. IEEE Latin America Transactions, 20(7): 2020-2028. https://doi.org/10.1109/TLA.2021.9827475
[26] Patil, R., Bellary, S. (2021). Ensemble learning for detection of types of melanoma. In 2021 International Conference on Computing, Communication and Green Engineering (CCGE), pp. 1-6. https://doi.org/10.1109/CCGE50943.2021.9776373
[27] Mane, D., Ashtagi, R., Kumbharkar, P., Kadam, S., Salunkhe, D., Upadhye, G. (2022). An improved transfer learning approach for classification of types of cancer. Traitement du Signal, 39(6): 2095-2101. https://doi.org/10.18280/ts.390622