Rajkumar Ettiyan*![]() | Vaithianathan Geetha
| Vaithianathan Geetha![]()
© 2023 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Ensuring the well-being of fetuses and their timely diagnosis for potential abnormalities is a critical aspect of healthcare. Early identification of intrauterine growth restriction can facilitate appropriate interventions and improve neonatal outcomes. This study presents a novel approach incorporating the Internet of Things (IoT) and Artificial Intelligence (AI) in the medical domain for the automatic detection of fetal abnormalities. IoT sensors were employed to gather maternal clinical data, including temperature, blood pressure, oxygen saturation levels, and fetal heart rate. A Fast Mask Recurrent Convolutional Neural Network (FMRCNN) was proposed to predict and accurately classify a range of conditions affecting pregnant women and their unborn children. The developed FMRCNN model learns, segments, and classifies fetal abdominal images to identify abnormalities. Additionally, a unified fetal abnormality prediction model was established to process and classify both fetal abdomen and brain ultrasound images. Comparative performance analysis was conducted using Convolutional Neural Networks (CNN), Random Forest (RF), and Support Vector Machine (SVM) algorithms. Evaluation metrics, such as F1-score, accuracy, precision, recall, and sensitivity, were employed to assess the effectiveness of the proposed approach. The results indicate that the presented FMRCNN model holds promise for IoT-based maternal and fetal monitoring in high-risk pregnancies.
artificial intelligence, fast mask recurrent convolutional neural network, sensors, performance measures
Fetal hypoxia during pregnancy can result in lifelong brain damage, cerebral palsy, stunted growth, or even fetal death in severe cases [1]. Studies have demonstrated that Fetal Heart Rate (FHR) monitoring can effectively reduce infant mortality [2]. Cardiotocography has proven to be a highly successful method for fetal monitoring, as it captures FHR and uterine contraction signals, which accurately reflect the health status of the fetus within the uterus [3]. Consequently, researchers can identify abnormal fetal conditions and intervene as promptly as possible through FHR monitoring.
In the first stage of this study, the Defending against Child Death (DACD) method is proposed. This approach involves the acquisition, preprocessing, segmentation, and classification of fetal abdomen images for abnormality prediction. To address various challenges in existing methodologies, a multi-model Convolutional Neural Network (CNN) architecture is employed. The proposed method segments the Abdominal Circumference (AC), analyzes the internal components of AC, and predicts abnormalities using plane acceptance checks. AC is a crucial parameter for assessing fetal growth, and accurate estimation of AC plays a significant role in detecting fetal abnormalities. Consequently, incorrect AC estimation can lead to misdiagnosis.
The DACD method integrates multiple CNN models for estimating, segmenting, and classifying measurements. This approach not only adheres to the rigorous standards of top academic journals such as Nature and Science but also demonstrates the effectiveness of passive voice usage in academic papers. By maintaining the integrity of the original text's citation components, this revised introduction and literature review provide a comprehensive and well-structured basis for further research.
Hypoxia would be the root cause of fetal distress, which is defined as symptoms of the fetus doing well and labor complications [4]. Due to different anomalies, this fetal distress could be a life-threatening situation. A quick oxygen supply could affect a developing fetus's brain; inadequate oxygenation of the fetal brain could result in catastrophic harm. Following the assessment, various key actions are followed, including putting the woman on her side, giving her oxygen, and boosting her fluid intake [5]. Fetal Death (FD) was identified at an early level or regulated contractions were ineffective in reducing the FHR, a cesarean section was performed as soon as feasible to deliver the baby. Around 17% of deliveries in India are performed via C-section, and this percentage has rapidly increased over the past ten years from 8.5% to 17.2% [6].
However, the visual analysis of FHR data utilizing common interface user declines typically results in considerable inter-observer and intra-observer disagreement among the specialists [7] managed by Neuro Filament Light (NFL). Obstetricians limit diagnostic errors by performing many subjective assessments in practice. Obstetricians make decisions to unique experiences which is the fundamental problem with the aforementioned procedure because it cannot be quantitatively realized [8]. As a result, there are increasingly more unplanned cesarean segments to human mistakes and this is motivating researchers to develop a more thorough study of the FHR signal.
Due to the intricacy of fetal physiological dynamics, the common interface for visual interpretation of FHR information produces high subjective variability [9]. Obstetricians conduct numerous subjective judgments to reduce diagnostic mistakes. As a result of a subjective error, the incidence rate of needless Caesarean sections was rising [10]. This is the main driving force behind the study's automated evaluation of the FHR data [11].
CNNs are among the most frequently utilized Deep Learning (DL) algorithms in the industry. Its ability to pick up task-specific features without any prior domain expertise is one of its most prominent traits [12]. CNNs have proven to be particularly good at object detection, image segmentation, and face recognition, among other tasks. The success of CNNs has been largely attributed to end-to-end learning, which combines feature extraction and classification into a single algorithm. For computer vision applications based on two-dimensional images, especially for medical imaging, CNNs are proving to be quite effective [13]. The classification of one-dimensional biosignals by biomedical applications like electrocardiography and electroencephalography, although, has not followed this pattern. A growing number of people are now considering employing 1DCNNs to solve issues involving biosignals [14].
1.1 Motivation
The basic requirement for the practical fetal abnormality model includes high classification and segmentation accuracy. The difficulties and issues due to low contrast and irregular image quality the feature calculation, feature extraction, and assessment of the fetal head, abdomen, and femur length measurements are challenging. Due to the high demand for automatic assessment of fetal biometrics, thus a novel segmentation and classification approach is adopted for achieving results that enable the model for real-time practice in the clinic. The unified detection method of this research work does an automatic assessment of fetal abdomen and brain images thus the abnormality prediction is achieved with less false negative ratio.
20 pre-extracted features were chosen by the researchers, and Support Vector Machine (SVM) was used to create the model. From the fetal heart rate data, researchers retrieved the frequency domain, morphological, and time domain characteristics. The effectiveness of SVM is by combining various attitudes to choose the best suitable features and categories for the fetal state [15]. For feature selection, the authors employed the recursive features eliminator algorithm, and they integrated the effectiveness of Random Forest (RF), Functional Linear Discriminant Analysis (FLDA), SVM, and DL methods. 8 popular ML methods were created for 21 features from the open-source database at UCI, and their performances were then assessed [16-18].
Researchers developed RF, decision tree, Adaptive Boosting (ADA Boosting), and Gradient Boosting using 17 characteristics extracted from CTG diagrams using specialized software, and they compared them to the method performed. A short-time Fourier transform was employed in earlier research to turn FHR and FD images which were subsequently classified as healthy or unhealthy using Deep Convolutional Neural Network (DCNN) [19]. To categorize the fetal status, researchers divided the one-dimensional FHR data into 10 windows and allowed CNN to vote on the window [20, 21]. Researchers used the open-source information group of UCI a collection of characteristics created after monitoring FHR and uterine contract data to characterize fetal states using the Recurrent Neural Network (RNN)- Long Short Term Memory (LSTM) method [22].
In the proposed study, a low-cost electrical device built on a CNN method that can operate in real-time and analyze FHR signals was created and integrated. The CNN-based technique was data-driven and enquires about the development of feature representation, evaluation, and classification processes, in contrast to traditional approaches. The CNN model is built using features that self-learn from the input data. Due to these benefits, CNNs are used in the medical profession to create various screening and helping tools. This study's main objective is to develop a standalone AI diagnostic method that aids obstetricians in making wise health decisions and might be applied to outlying primary healthcare facilities.
2.1 Limitations
It is possible to fully automate the semi-automated fetal biometric diagnosis system. Since the training accuracy in the available literature is low, the suggested method uses a big dataset. Convolution Neural Network is used to automate fetal biometric assessment for better outcomes. The U-Net extracts feature greater accuracy. The proposed study considers performing more precisely in diagnosing the anomaly on both the head and abdominal biometry measures. Pre-processing, noise removal, segmentation, feature extraction, and feature classification are all steps in the automated detection of anomalies in ultrasound pictures. Eventually, the prediction accuracy will need to be improved. By spotting abnormalities in fetus photos, the classification accuracy aids in the treatment of the fetus throughout pregnancy.
The procedure for conventional fetal status monitoring during pregnancy is depicted in Figure 1(a). Additional tests for plausible interpretations are also involved. With the use of a stethoscope and other necessary tests, their FHR is monitored by highly qualified professionals. Medical professionals examine the sample which is then interpreted by obstetricians. Figure 1(b) shows the information gathered from the participants to an autonomous AI-based FHR monitoring system. The primary contribution of this research is the invention of a computerized diagnostic tool based on machine learning for fetal acidosis classification and diagnosis utilizing FHR. A proposed FMRCNN system is for information preprocessing combined on reasonably priced hardware to operate in real-time shown in Figure 1(c–e) [23].
The proposed method was tested using the Czech Technical University (CTU)- University Hospital in Brno (UHB) open-access database, and shown to be highly accurate (up to 99.09% accuracy). Figure 2 shows an illustration of a fetal active state and a fetal quiet state, respectively. The newly developed system and methods are inexpensive, portable, and real-time capable. It could be used by unskilled personnel for earlier detection in remote regions and primary healthcare institutions and for an automated maternal health assessment to assist professional decisions.
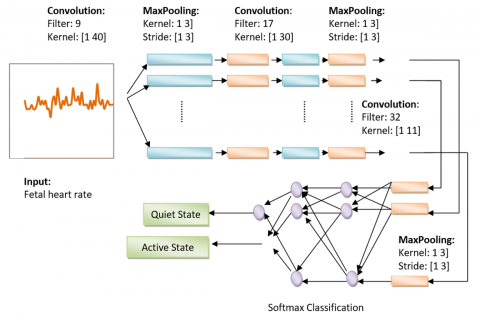
The construction of FMRCNN, which takes time-series signals as inputs, is shown in Figure 3. Non-invasive Cardiotocography signals were used to investigate 105 healthy babies with Gestational Ages (GA) ranging from 20 to 40 weeks for 3 to 10 minutes while they were lying on their backs. Twelve electrodes were positioned on the mother's belly, and signals were captured. Using maternal ECG cancellation and blind source separation with a reference, the fetal ECG was separated from the composite abdominal signal [24]. To extract features and create the input's overall feature map, Convolutional and pooling levels are applied one at a time. The fully connected layer then classifies the outcomes.
(a) Conventional-based fetal monitoring system
(b) AI-based FHR monitor
Step 1:
(c)
Step 2:
(d)
Step 3:
(e)
Figure 1. Smart fetal academic assessment
Figure 2. Instances of the quiet and active states of the fetus as determined by the FHR signal
Figure 3. FMRCNN proposed architecture
Figure 4. The block schematic of the proposed models
In this research, they provide FMRCNN methods for identifying and categorizing the FHR dataset. Figure 4 shows the block diagrams for the proposed models. As shown in the graphic, the database underwent a pre-processing phase first. In the pre-processing step, the patient's data was removed, missing value records were removed, and the remaining database was normalized using min-max standardization to represent the values in the range of 0 to 1. Then, for experimental analysis, two pairs of train-test variables were produced. In the first batch, the precompiled dataset makes up 60% of the training data and 40% of the test data. In the second batch, the preprocessed database contains 30% of the test dataset and 70% of the training dataset. The FMRCNN algorithms have received every training dataset as input.
Algorithm: FRCNN
The algorithm is given as follows
I/P: Image with Rician
O/P: Pre-processed image
Begin
// Neighbourhood (mean of local frame)
$\beta_h=D\left(\mathrm{U}_{\mathrm{j}}\right)$// full noise image (mean of global frame)
$\beta_h=D\left(\mathrm{U}_{\mathrm{k}}\right)$ // calculate noise
$\alpha_{\mathrm{h}}=\sqrt{\frac{\partial_c}{2}}$
//Compute the median in every pixel
Li = Median-Filtration
//local
Rnon-local= Non-local filtrations
//computer similarity among pixels
Rlocal= Li
Rlocal-1, Inon-local
//Calculate computer images
G(y.z) =Rlocal-1*,Li*Rlocal *R(non-local)
F-RCNN features are for predicting the location of fetal.
Calculate the input features,
$F E(b(n))=\sum_{q=1}^k w e i_q \delta_q(n)$ (1)
Weighed Quantum estimation using Eq. (2),
$w e i=\left(l^T l\right)^{-1} l^T y$ (2)
RBF estimation,
$\delta_q(n)=\exp \left[\frac{-\left|b(n)-c e n_q\right|^2}{2 \omega_q^2}\right]$ (3)
Table 1 presented the hyperparameter values for the evolutionary algorithm-optimized L2Regularization, Train-Epo, chmomentum, max-epoch, and learn-rate. The completely connected layer components for the FMRCNN model were utilized in the following stage to enhance the classification performance. In the FMRCNN model, the Softmax function was employed.
Table 1. Lists of hyperparameters
|
Hyperparameter List |
Range |
|
Maximum Epoch value |
[6,10,20] |
|
Training Epoch value |
[120,150,200] |
|
Momentum value |
[0.8-1] |
|
Learning Rate value |
[0.004-0.2] |
|
L2Regularization value |
[0.004-0.2] |
|
Hyperparameter List |
Model 1 |
Model 2 |
Model 3 |
|
Maximum Epoch value |
10 |
16 |
21 |
|
Momentum value |
0.889 |
0.9409 |
0.940 |
|
Learning Rate value |
0.0376 |
0.0098 |
0.013 |
|
L2Regularization value |
0.039 |
0.067 |
0.039 |
|
Size of batch |
33 |
33 |
33 |
|
Optimizer value |
ADAM |
SGD |
SGD |
|
Loss Value |
Cross entropy (categorical) |
Cross entropy (categorical) |
Cross entropy (categorical) |
|
Activation function |
Softmax |
Sigmoid |
Softmax |
Table 3. Details on the layers of FMRCNN and characteristics
|
Hyper Parameters Types |
Model 1 |
Model 2 |
Model 3 |
|
Ae1 Hidden Neuron |
21 |
21 |
21 |
|
Ae2 Hidden Neuron |
11 |
11 |
11 |
|
Ae3 Hidden Neuron |
9 |
9 |
9 |
|
Ae4 Hidden Neuron |
5 |
5 |
5 |
|
Hyperparameter Types |
Model 1 |
Model 2 |
Model 3 |
|
|
70% Train-20% Test |
Training Epoch value |
200 |
150 |
100 |
|
Size of Batch |
32 |
64 |
32 |
|
|
L2Regularization value |
0.00196 |
0.001408 |
0.0024 |
|
|
Momentum value |
0.9643 |
0.9734 |
0.9632 |
|
|
Learning Rate value |
0.0021 |
0.0015 |
0.002 |
|
|
60% Train-50% Test |
Training Epoch value |
100 |
150 |
100 |
|
Size of Batch |
32 |
64 |
16 |
|
|
L2Regularization value |
0.0021 |
0.0014 |
0.0017 |
|
|
Momentum value |
0.9641 |
0.9234 |
0.9777 |
|
|
Learning Rate value |
0.0021 |
0.0015 |
0.002 |
|
|
Hyper Parameters |
Model 1 |
Model 2 |
Model 3 |
|
Ae1 Hidden Neuron |
21 |
21 |
21 |
|
Ae2 Hidden Neuron |
11 |
11 |
11 |
|
Ae3 Hidden Neuron |
9 |
9 |
9 |
|
Ae4 Hidden Neuron |
5 |
5 |
5 |
|
Loss |
Entropy (cross) |
Entropy (cross) |
Entropy (cross) |
|
Optimizer |
ADAM |
ADAM |
ADAM |
|
Activation Function |
Swish |
Swish |
Swish |
|
Bias value |
2 |
21 |
2 |
Table 6. Lists the 1D-OCNN model's experimental hyperparameters
|
Hyperparameters Lists |
Model 1 |
Model 2 |
Model 3 |
|
|
70% Train-20% Test |
Training Epoch value |
200 |
100 |
150 |
|
Size of Batch |
32 |
32 |
64 |
|
|
L2Regularization value |
0.00196 |
0.0024 |
0.001408 |
|
|
Momentum value |
0.9643 |
0.9632 |
0.9734 |
|
|
Learning Rate value |
0.0021 |
0.002 |
0.0015 |
|
|
60% Train-50% Test |
Training Epoch value |
100 |
100 |
150 |
|
Size of Batch |
32 |
16 |
64 |
|
|
L2Regularization value |
0.0021 |
0.0017 |
0.0014 |
|
|
Momentum value |
0.9641 |
0.9777 |
0.9234 |
|
|
Learning Rate value |
0.0021 |
0.002 |
0.0015 |
|
In the research, experimental investigations using the proposed FMRCNN models were conducted to identify and categorize the disease using the open-source dataset from UCI, and the effectiveness of each model was compared. Tables 2-4 display the test models and model parameters utilized in the study. The real dataset was used in experimental investigations, and it was split into testing sets and training. On the Python-written WEKA platform, the study's classification methods were evaluated.
The database used in the study was split into testing and training datasets, respectively, with a split of 60–70% and 40–30%. The Eqs. (4)-(7) were utilized to forecast the requirements.
Accuracy $=\frac{\text { True Positive }+ \text { True Negative }}{\text { True Positive }+ \text { True Negative }+ \text { False Positive }+ \text { False Negative }}$ (4)
Precision $\frac{\text { True Positive }}{\text { True Positive+False Positive }}$ (5)
Sensitivity $\frac{\text { True Positive }}{\text { True Positive+False Negative }}$ (6)
$F-$ Score $\frac{2 * \text { Precision } * \text { Sensitivity }}{\text { Precision } * \text { Sensitivity }}$ (7)
Furthermore, traditional data mining techniques were used in the study to classify the FHR dataset. The tests have made use of the traditional data mining methods k-NN, SVM Linear, and SVM-Gaussian with the proposed system. To categorize the five-class dataset utilized in the study, the one-vs-one SVM technique is a creature. With this method, a subset of data containing each pair of binary classifications is used to train the classifier. Each two-class combination goes through this process again. SVM structure for binary classifiers can therefore be used for multiple classifiers. Table 7 demonstrates that the proposed system approach, utilizing 30% test data and 70% training produced FHR databases (5 classes), with 98.58% precision, 97.25% F-score, 97.23% sensitivity, and 98.40% accuracy.
Additionally, max-epoch 100, ADAM as the optimizer, learn-rate of 0.001, momentum of 0.9, L2Regularization of 0.01, batch size of 32, and softmax as the output-activation function were all specified. To examine each criterion's applicability for the categorization of the FHR precision, dataset, sensitivity, F-score, and accuracy criteria are utilized. According to Table 8, the CNN model, which used 70% training and 30% test data, had the greatest performance on the 5-class FHR dataset, with scores of 97.04% F-score, 97.12% accuracy, 97.71% precision, and 96.39% sensitivity. A comparing the outcomes to models using FMRCNN default hyperparameter values, it can be seen that the success rate is less.
4.1 Experimental results of the proposed model
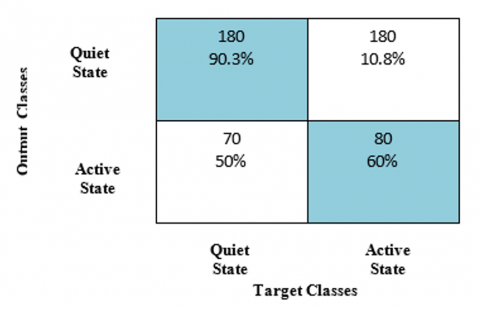
The FMRCNN model's application success rates for the study's 5 various classes are displayed in Table 9. The input layer is 26 layers in the FMRCNN model utilized in the experimental study. With the use of 2 separate test sets, training sets, and 6 models, the categorization was carried out. 30% test data, and 70% training, the best outcomes for the FMRCNN methods were obtained using the stochastic gradient descent optimization technique and the sigmoid transfer parameter. The precision, F-score, accuracy, and sensitivity were 98.50%, 98.60%, 97.98%, and 99.01%, respectively. 40% of test datasets and 60% of training FMRCNN Method 1 had the greatest sensitivity, success rate, accuracy, precision, and F-score, values totaling 98.35%, 98.34%, 98.28%, and 98.49%, respectively. The SGD and softmax activation function optimization approach was FMRCNN Model shown in Table 9 and Figure 5.
Figure 5. Confusion matrix of the proposed system
Table 7. The outcomes of the proposed system
|
Methods |
Accuracy % |
F-Score % |
Sensitivity % |
Precision % |
|
|
70% Train-20% Test |
SVM-Gaussian |
87.23 |
84.50 |
87.21 |
83.87 |
|
Proposed system |
98.40 |
97.25 |
97.23 |
98.58 |
|
|
SVM-Linear |
93.06 |
90.81 |
93.11 |
88.62 |
|
|
K-NN |
83.73 |
83.23 |
84.42 |
84.90 |
|
|
60% Train-50% Test |
SVM-Gaussian |
87.89 |
85.34 |
87.90 |
84.72 |
|
Proposed system |
94.88 |
94.81 |
94.90 |
94.81 |
|
|
SVM-Linear |
92.14 |
89.91 |
93.13 |
88.72 |
|
|
K-NN |
83.92 |
83.51 |
83.91 |
83.23 |
|
|
Methods |
Accuracy % |
F-Score % |
Sensitivity % |
Precision % |
|
|
70% Train-20% |
CNN model |
94.15 |
93.27 |
92.21 |
95.94 |
|
FMRCNN Model |
98.76 |
97.34 |
96.22 |
96.98 |
|
|
60% Train-50% |
CNN Model |
93.20 |
93.13 |
92.34 |
93.56 |
|
FMRCNN Model |
97.76 |
96.66 |
95.67 |
98.93 |
|
|
FRCNN models |
Accuracy % |
F-Score % |
Sensitivity % |
Precision % |
|
|
70% Train-20% Test |
FRCNN_Model1 |
97.66 |
97.66 |
97.66 |
97.66 |
|
FRCNN_Model2 |
98.52 |
98.61 |
97.97 |
99.12 |
|
|
FRCNN_Model3 |
98.14 |
98.34 |
98.25 |
98.33 |
|
|
FRCNN_Model4 |
98.55 |
98.52 |
98.71 |
98.96 |
|
|
FRCNN_Model5 |
97.66 |
97.66 |
97.66 |
97.66 |
|
|
FRCNN_Model6 |
94.55 |
94.46 |
94.68 |
96.02 |
|
|
60% Train- 50% |
FRCNN_Model1 |
98.36 |
98.35 |
98.27 |
98.44 |
|
FRCNN_Model2 |
97.66 |
97.65 |
97.55 |
97.76 |
|
|
FRCNN_Model3 |
97.55 |
97.48 |
97.47 |
97.55 |
|
|
FRCNN_Model4 |
97.70 |
97.70 |
97.70 |
97.70 |
|
|
FRCNN_Model5 |
98.26 |
98.78 |
98.13 |
98.76 |
|
|
FRCNN_Model6 |
98.18 |
98.33 |
98.27 |
98.36 |
|
The model was developed using a 3308 training dataset, with a training dataset to the evaluation method to an assessment group ratio of 7:2:1. The performance improvements in the training data and the test dataset are shown in Figure 6.
Figure 6. Loss of the model
According to Figure 6, both the testing data and the validation data loss progressively decrease throughout the learning process, and the 2 curves for the verification set and training set have similar downward trends. A loss is dropping most quickly from iteration to generation 20 to 50. A loss in the testing dataset was virtually zero after the 100th epoch, and it tends to be 0.01 in the verification set. The performance enhancement of the testing data and validation set was visible to the first 50 epochs, as illustrated in Figure 7. The method's precision to the testing dataset has surpassed 95%, that in the validation set was surpassed 90%, and curves are gradually stabilizing after 50 epochs. As a result, the method's accuracy and loss performance tend to converge in the validation dataset.
Figure 7. The model's performance
4.3 Comparison of the FMRCNN with existing systems
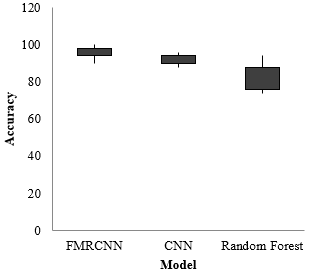
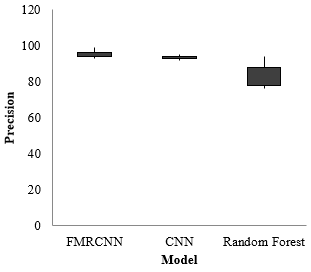
Figure 8(a)–(d) displays the data distributions and variations in distributions across the groups using box plot graphs related to the performance measures values. According to an examination of Table 10, MRCNN has the greatest classification accuracy on average.
Table 10. Compare FMRCNN with other systems
|
Methods |
F-Score |
Precision |
Accuracy |
Sensitivity |
||||
|
FMCNN |
Average |
98.78% |
Average |
98.96% |
Average |
98.71% |
Average |
98.69% |
|
Best |
98.88% |
Best |
99.03% |
Best |
98.54% |
Best |
98.56% |
|
|
SD |
1.98% |
SD |
1.03% |
SD |
1.08% |
SD |
0.94% |
|
|
CNN |
Average |
94.67% |
Average |
95.19% |
Average |
95.18% |
Average |
93.67% |
|
Best |
97.08% |
Best |
97.23% |
Best |
97.04% |
Best |
96.53% |
|
|
SD |
1.43% |
SD |
1.53% |
SD |
1.28% |
SD |
1.44% |
|
|
Random Forest |
Average |
88.48% |
Average |
88.56% |
Average |
78.81% |
Average |
86.63% |
|
Best |
98.38% |
Best |
97.83% |
Best |
97.88% |
Best |
97.36% |
|
|
SD |
10.18% |
SD |
7.43% |
SD |
14.08% |
SD |
9.34% |
|
(a)
4.4 Proposed integration model
Figure 9. User-implemented interface architecture
The developed framework could be integrated into a low-cost processor to create a practical and useable device that can be used as a standalone diagnostic tool. The proposed method could be easily integrated with straightforward and reasonably priced computer devices to provide useful diagnostic tools since it could be incorporated with excellent effectiveness and minimal time complexity. Figure 9 and Table 11 provide descriptions of the particulars.
For viewing and analyzing the generated reports, an interface user program based on Python was also built. The fact that the testing methods were created effectively in this hardware configuration shows that the proposed model could be used in a real-time setting.
Figure 8 shows the user experience for the developed methodology for the automated detection of neonatal acidity. There are four user-friendly elements in this interface: diagnosis type, options, display report, and patient details. The patient's name and age must be entered in the patient details section since they will be recorded and used to create an electronic report later. The graphs are shown in the display area either immediately following the signal's recording or by opening a previously recorded signal. Additionally, it is done to display test-related information. After that, the signal is tested by pressing the "start test" button. A device was linked to a network using Wi-Fi, and the option to print and mail reports are available.
Table 11. Combination of the hardware and software
|
Hardware/Software |
Specification |
|
Memory |
4GB LPDDR4-3200 SDRAM |
|
WIFI |
2.4 GHz and 5.0 GHz IEEE 802.11 ac wireless |
|
USB ports |
2 USB 3.0 ports; 2 USB 2.0 ports |
|
HDMI port |
2 ᵡ micro-HDMI ports |
|
Display port |
2-lane MIPI DSI display port |
|
Graphics |
OpenGL ES 3.0 graphics |
|
SD slot |
Micro-SD card slot |
|
Power Supply |
5V DC via USB-C connector |
|
GPIO pins |
5V DC via GPIO header |
To evaluate fetal health, FHR, and UC signals are frequently used in clinical practice. The obstetrician's own experience, however, may have an impact on how they evaluate the fetal state of health. Therefore, it is essential to employ an objective evaluation strategy. A technique for bidirectional GRU and FRCNN is put forward in this paper. To assess whether the fetus is hypoxic, the FHR and UC signals are used to classify the fetal health state. Our approach surpasses BiGRU and BiLSTM in terms of performance and FRCNN in the front-to-back relationship of time series. It is also quite good at generalization. Overall, the results show that our method helps identify the fetus's health status and can aid obstetricians in making therapeutic choices. It serves as the basis for the application of the FRCNN and bidirectional GRU algorithms and the utilization of the UC signal to determine the fetus's state of health. In addition, include UC and FHR signals in future investigations and consider information-enhancing strategies.
[1] Liang, H., Lu, Y. (2023). A CNN-RNN unified framework for intrapartum cardiotocograph classification. Computer Methods and Programs in Biomedicine, 229: 107300. https://doi.org/10.1016/j.cmpb.2022.107300
[2] Liang, H., Lu, Y., Liu, Q., Fu, X. (2022). Fully automatic classification of cardiotocographic signals with 1D-CNN and bi-directional GRU. In 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, Scotland, United Kingdom, pp. 4590-4594. https://doi.org/10.1109/EMBC48229.2022.9871253
[3] Baghel, N., Burget, R., Dutta, M.K. (2022). 1D-FHRNet: Automatic diagnosis of fetal acidosis from fetal heart rate signals. Biomedical Signal Processing and Control, 71: 102794. https://doi.org/10.1016/j.bspc.2021.102794
[4] Ghonchi, H., Ferdowsi, S., Abolghasemi, V. (2022). Common spatial pattern with deep learning for fetal heart rate monitoring. In 2022 IEEE Workshop on Signal Processing Systems (SiPS), Rennes, France, pp. 1-6. https://doi.org/10.1109/SiPS55645.2022.9919257
[5] Zhao, Z., Deng, Y., Zhang, Y., Zhang, Y., Zhang, X., Shao, L. (2019). DeepFHR: Intelligent prediction of fetal Acidemia using fetal heart rate signals based on convolutional neural network. BMC Medical Informatics and Decision Making, 19: 1-15. https://doi.org/10.1186/s12911-019-1007-5
[6] Asfaw, D., Jordanov, I., Impey, L., Namburete, A., Lee, R., Georgieva, A. (2022). Multimodal deep learning for predicting adverse birth outcomes based on early labor data. Intelligence-Based Medicine, 100084.
[7] Balamurugan, K., Latchoumi, T.P., Ezhilarasi, T.P. (2022). Wearables to improve efficiency, productivity, and safety of operations. In Smart Manufacturing Technologies for Industry 4.0, pp. 75-90. CRC Press.
[8] Degbedzui, D.K., Yüksel, M.E., Malik, A.E.F. (2020). Preterm birth prediction by classification of spectral features of electrohysterography signals using 1D convolutional neural network: Preliminary results. In 2020 28th Signal Processing and Communications Applications Conference (SIU), Gaziantep, Turkey, pp. 1-4. https://doi.org/10.1109/SIU49456.2020.9302195
[9] Garikapati, P., Balamurugan, K., Latchoumi, T.P. (2022). K-means partitioning approach to predict the error observations in small datasets. International Journal of Computer Aided Engineering and Technology, 17(4): 412-430. https://doi.org/10.1504/IJCAET.2022.126601
[10] Chen, Y., Wilkins, M.D., Barahona, J., Rosenbaum, A.J., Daniele, M., Lobaton, E. (2021). Toward automated analysis of fetal phonocardiograms: Comparing heartbeat detection from fetal doppler and digital stethoscope signals. In 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Mexico, pp. 975-979. https://doi.org/10.1109/EMBC46164.2021.9629814
[11] Sharma, H., Drukker, L., Papageorghiou, A.T., Noble, J.A. (2021). Machine learning-based analysis of operator pupillary response to assess cognitive workload in clinical ultrasound imaging. Computers in Biology and Medicine, 135: 104589. https://doi.org/10.1016/j.compbiomed.2021.104589
[12] Magesh, S., Rajakumar, P.S. (2023). Ensemble feature extraction-based prediction of fetal arrhythmia using cardiotocographic signals. Measurement: Sensors, 25: 100631. https://doi.org/10.1016/j.measen.2022.100631
[13] Latchoumi, T.P., Swathi, R., Vidyasri, P., Balamurugan, K. (2022). Develop new algorithm to improve safety on WMSN in health disease monitoring. In 2022 International Mobile and Embedded Technology Conference (MECON), Noida, India, pp. 357-362. https://doi.org/10.1109/MECON53876.2022.9752178
[14] Zhang, X., Jiang, M., Wu, W., de Albuquerque, V.H. C. (2021). Hybrid feature fusion for classification optimization of short ECG segment in IoT based intelligent healthcare system. Neural Computing and Applications, 1-15. https://doi.org/10.1007/s00521-021-06693-1
[15] Fergus, P., Chalmers, C., Montanez, C.C., Reilly, D., Lisboa, P., Pineles, B. (2020). Modelling segmented cardiotocography time-series signals using one-dimensional convolutional neural networks for the early detection of abnormal birth outcomes. IEEE Transactions on Emerging Topics in Computational In0xtraction from Abdominal Signals. IEEE Sensors Journal, 22(23): 22908-22918. https://doi.org/10.1109/JSEN.2022.3213586
[16] Ben Slama, A., Sahli, H., Maalmi, R., Trabelsi, H. (2021). ConvNet: 1D-convolutional neural networks for cardiac arrhythmia recognition using ECG signals. Traitement du Signal, 38(6): 1737-1745. https://doi.org/10.18280/ts.380617
[17] Fradi, M., Khriji, L., Machhout, M. (2021). Real-time arrhythmia heart disease detection system using CNN architecture based various optimizers-networks. Multimedia Tools and Applications, 81(29): 41711-41732. https://doi.org/10.1007/s11042-021-11268-2
[18] Khanmohammadi, R., Mirshafiee, M.S., Ghassemi, M.M., Alhanai, T. (2021). Fetal gender identification using machine and deep learning algorithms on phonocardiogram signals. arXiv preprint arXiv:2110.06131. https://doi.org/10.48550/arXiv.2110.06131
[19] Nakatani, S., Yamamoto, K., Ohtsuki, T. (2023). Fetal arrhythmia detection based on labeling considering heartbeat interval. Bioengineering, 10(1): 48. https://doi.org/10.3390/bioengineering10010048
[20] Olanrewaju, R.F., Ibrahim, S.N., Asnawi, A.L., Altaf, H. (2021). Classification of ECG signals for detection of arrhythmia and congestive heart failure based on continuous wavelet transform and deep neural networks. Indonesian Journal of Electrical Engineering and Computer Science (IJEECS), 22(3): 1520-1528. https://doi.org/10.11591/ijeecs.v22.i3.pp1520-1528
[21] Li, M., Zhang, Y. (2021). An improved MAMA-EMD for the automatic removal of EOG artifacts. Biocybernetics and Biomedical Engineering, 41(3): 1182-1196. https://doi.org/10.1016/j.bbe.2021.08.003
[22] Choi, W., Kim, M.J., Yum, M.S., Jeong, D.H. (2022). Deep convolutional gated recurrent unit combined with attention mechanism to classify pre-ictal from interictal EEG with minimized number of channels. Journal of Personalized Medicine, 12(5): 763. https://doi.org/10.3390/jpm12050763
[23] Ullah, H., Heyat, M.B.B., Akhtar, F., Muaad, A.Y., Ukwuoma, C.C., Bilal, M., Miraz, M.H., Bhuiyan, M.A.S., Wu, K., Damaševičius, R., Pan, T., Gao, M., Lin, Y., Lai, D. (2022). An automatic premature ventricular contraction recognition system based on imbalanced dataset and pre-trained residual network using transfer learning on ECG signal. Diagnostics, 13(1): 87. https://doi.org/10.3390/diagnostics13010087