Wenkai Duan![]() | Tianxiao Fu
| Tianxiao Fu![]() | Ningyuan Zhou
| Ningyuan Zhou![]() | Chuncui Zheng
| Chuncui Zheng![]() | Zhenya Zhu
| Zhenya Zhu![]() | Lingyao Peng*
| Lingyao Peng*![]()
© 2023 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
This study selected the medical record data of patients who underwent ultrasound examination and surgical treatment at Shaw Hospital, affiliated with Zhejiang University Medical College, from January 2018 to June 2020 and screened nine high-risk patients with thyroid papillary carcinoma and eight low-risk patients who met the enrollment criteria. The pathological and ultrasonic imaging data of the thyroid nodules and cervical lymph nodes of the enrolled patients were retrospectively analyzed. Clinicopathological aspects: age, number of lesions, lymph node area, and number of lymph nodes were significant. The younger the age, the higher the risk of cancer metastasis; the more the lymph node metastasis areas, the greater the number of lesions, and the higher the risk of cancer metastasis. An ultrasound image analysis of thyroid nodules showed that the number of microcalcifications and lesions was significantly and positively correlated with the risk of cancer metastasis. Ultrasonic image analysis of cervical lymph nodes showed that the indicators of cystic change, the number of calcifications, number of lymph node fusions, and number of clear lymph node boundaries were significantly and positively correlated with the risk of cancer metastasis. This study is crucial in the clinical diagnosis of thyroid papillary carcinoma metastasis and provides a theoretical basis for surgeons to formulate diagnosis and treatment plans for thyroid carcinoma.
papillary thyroid carcinoma, transfer, pathological analysis, ultrasonic analysis, diagnosis
Thyroid cancer accounts for approximately 90% of all endocrine system malignant tumors and 3.1% of all human malignant tumors [1]. Recently, thyroid cancer has become the fastest-growing solid tumor [2]. Among these, papillary thyroid carcinoma (PTC) is the main pathological type, accounting for approximately 89.9% of cases [3]. The prognosis of PTC is good, with a 5-year mortality rate of < 2%. However, approximately 25% of PTC patients experience recurrence during follow-up, and cervical lymph node metastasis can occur in early PTC [4]. Cervical lymph node metastasis, a regular, step-by-step process, is an independent risk factor that affects local recurrence and prognosis. It is usually "primary focus-central lymph node-ipsilateral cervical lymph node-contralateral cervical lymph node-distant metastasis" [5]. Therefore, cervical lymph node metastasis usually occurs first in central lymph node metastasis and rarely in leaping metastasis [6]. Theoretically, the size of the primary tumor is an essential clinicopathological feature, and the smaller the tumor's diameter, the lower the probability of lymph node metastasis. However, in our clinical practice, we found that some patients had small tumor diameters, but the number and area of lymph node metastases were high. These patients are also prone to the postoperative recurrence of regional lymph nodes.
Presently, clinical surgery routinely requires total or subtotal thyroidectomy and preventive neck central lymph node dissection for patients with PTC. However, there is still controversy about whether lymph nodes in the contralateral neck region should be resected [7]. Generally, the surgical method is determined based on imaging examination. If the preoperative report indicates suspicious abnormal lymph nodes in the lateral cervical region, corresponding regional lymph node dissection should be performed. Conversely, if the preoperative report indicates no suspicious abnormal lymph nodes in the lateral cervical region, the lateral cervical lymph node dissection should not be performed [8]. Therefore, surgeons must make surgical plans and select the scope of lymph node dissection to accurately evaluate the metastasis of cervical lymph nodes by preoperative neck ultrasound-selective enhanced examination, which can reduce the recurrence rate and improve the prognosis of patients [9]. Owing to its simplicity, safety, good repeatability, and low cost, ultrasound has become the most commonly used examination method to evaluate cervical lymph node metastasis [10, 11]. High-frequency ultrasound can describe and accurately evaluate the area, number, size, shape, internal structure, and blood vessel distribution of lymph nodes from all aspects and make more accurate qualitative judgments of lymph nodes.
In this study, the diagnosis of lateral cervical lymph node metastasis in patients with PTC was determined using neck-selective enhanced ultrasound, and its clinical value was discussed.
2.1 Sample information
Patients with thyroid diseases at Run Run Shaw Hospital, affiliated with Zhejiang University Medical College, were selected between January 2018 and June 2020. After the inclusion and exclusion criteria were determined, a small amount of diseased tissue was removed from the patients surgically (immediately after surgery). Next, samples were washed with phosphate buffered saline, cut into four pieces, placed in a liquid nitrogen bottle, and then transferred into the sample bank within half an hour and kept at -80℃ for long-term storage. Furthermore, informed consent was obtained from the enrolled patients, for using the samples for scientific research purpose. Subsequently, the relevant experiments were carried out after being approved by the hospital's ethics committee.
PTC inclusion criteria:
1) The postoperative pathological results indicated PTC.
2) No anti-cancer treatment was administered before the operation.
Exclusion criteria for PTC:
1) No preoperative thyroid ultrasound examination
2) Having other malignant tumors at the same time
3) Poor quality of the ultrasound image
4) Pregnant and lactating patients.
2.2 Ultrasound examination and grading criteria for thyroid cancer
GE Logiq E9, Siemens Acuson S3000, Philips EPIQ 7, and other color Doppler ultrasound instruments and linear array probes (frequency: 5-18 MHz) were selected as ultrasonic instruments. Before the operation, the patient's thyroid nodule ultrasound and neck regional lymph ultrasound were examined, focusing on the size of the nodule, growth direction (whether it grows vertically), internal echo (whether it is high or low, whether there is cystic change, etc.), whether the boundary is clear, whether the edge is smooth, whether there is calcification, the type and location of calcification, the relationship between the thyroid capsule and surrounding tissues, and the blood flow distribution. The thyroid nodules were graded according to the report of the Guidelines for the Diagnosis and Treatment of Thyroid Cancer (2018 version) [12] and the American Thyroid Association (ATA) Guidelines for Diagnosis and Treatment of Thyroid Diseases (2015 version) [13], and ultrasound-guided FNA cytological examination of suspicious nodules was carried out according to the guidelines.
PTC classification criteria:
Patients with PTC were classified into high-risk and low-risk PTC groups, according to the Guidelines for the Diagnosis and Treatment of Thyroid Cancer (2018 version) [12] and the ATA Guidelines for Diagnosis and Treatment of Thyroid Diseases (2015 version) [13]. The high-risk PTC group was defined as: tissue invasion around the thyroid, distant metastasis, ≥ 3 regional lymph node metastasis, >5 lymph node metastasis, or metastatic lymph nodes ≥3 cm. Contrastingly, the low-risk PTC group was defined as: no invasion of surrounding thyroid tissue, no distant metastasis, <3 regional lymph node metastasis, ≤ 5 lymph node metastasis, and metastatic lymph nodes <3 cm.
2.3 Statistical analysis
The data were statistically analyzed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). The chi-square test or Fisher's exact test was used for classification variables, and the difference was statistically significant at P<0.05. The measurement data (age) conforming to the normal distribution are expressed as x ± s, and non-normally distributed measurement data are expressed as M (QR). Differences were considered statistically significant at P<0.05, determined using an independent sample t-test.
3.1 Clinicopathological characteristics of patients with PTC of different grades
From January 2018 to June 2020, thyroid patients from Run Run Shaw Hospital, affiliated with Zhejiang University Medical College, were selected for retrospective analysis. PTC patients were screened using strict inclusion and exclusion criteria. According to the set criteria, nine samples from the high-risk PTC group and eight from the low-risk group were screened. The case information for the high-risk and low-risk groups is shown in Tables 1 and 2.
The average age of high-risk patients with PTC was 34.4 ± 4.8 (29-38) years, including two males and seven females, with a ratio of 1:3.5. The average age of patients in the low-risk PTC group was 45.3 ± 11.9 (29-56 years), including two males and six females (ratio, 1:3). The t-test analysis of two independent samples showed that there was a statistically significant difference in the overall mean age of patients in the two groups (t=-2.058, P=0.001<0.05), and the Pearson 2 test showed that there was no significant sex difference between high- and low-risk patients (P2=0.167, P>0.05) (Table 3).
In the high-risk PTC group, the number of metastatic lymph nodes was 9-50+, the number of metastatic areas was 5-6, and the maximum diameter of the lesion was 0.8-2 cm. In addition, there were four cases of single lesions and five cases of ≥ 2 lesions. In the low-risk PTC group, the number of metastatic lymph nodes was 0-3, the number of metastatic area was 0-2, and the maximum diameter of the lesion was 1.2-2.5 cm. There was a statistically significant difference in the number of metastatic lymph nodes and metastatic regions between the two groups (P<0.05); however, the difference in the maximum diameter of the lesions was not statistically significant (P>0.05), and the difference in the number of lesions was statistically significant (F=9.251, P=0.008<0.001) (Table 3).
Table 1. Pathological information of cases in the high-risk group of thyroid papillary carcinoma
|
Case |
Gender |
Age |
Single/multiple focus |
Major diameter (cm) |
Number of lymph node metastasis areas |
Number of metastatic lymph nodes |
Larger lymph node tumor type |
Tumor type |
|
1# |
F |
29 |
S |
1.0 |
6 |
23+/79 |
3.89cm×1.35cm |
Thyroid papillary carcinoma (solid subtype), with intraglandular dissemination and invasion of the capsule |
|
2# |
F |
35 |
M |
1.5 |
5 |
50+/113 |
3.52cm×0.86cm |
Thyroid papillary carcinoma with intraglandular dissemination |
|
3# |
F |
34 |
S |
0.8 |
5 |
47+/143 |
1.82cm×0.78cm |
Thyroid papillary carcinoma; invading capsule |
|
4# |
F |
33 |
S |
1.5 |
5 |
9+/57 |
1.60cm×0.86cm |
Thyroid papillary carcinoma with intraglandular dissemination; encapsule invasion |
|
5# |
F |
31 |
M |
1.5 |
5 |
25+/96 |
3.26cm×0.42cm |
Papillary thyroid carcinoma |
|
6# |
F |
29 |
M |
2.2 |
5 |
29+/94 |
1.75cm×0.99cm |
Thyroid papillary carcinoma; invading capsule |
|
7# |
M |
44 |
M |
1.5 |
6 |
41+/228 |
2.49cm×1.34cm |
Thyroid papillary carcinoma with intraglandular dissemination |
|
8# |
M |
38 |
S |
1.0 |
5 |
15+/52 |
1.39cm×1.13cm |
Thyroid papillary carcinoma with intraglandular dissemination |
|
9# |
F |
37 |
M |
2.0 |
5 |
15+/50 |
3.2cm×1.3cm |
Papillary thyroid carcinoma |
Note: The high-risk PTC group is defined as surrounding thyroid tissue invasion, distant metastasis, ≥ 3 regional lymph node metastasis, >5 lymph nodes metastasis, or metastatic lymph nodes ≥ 3 cm. F, female; M, male; S, single; M, multiple
Table 2. Pathological information of cases in the low-risk group of thyroid papillary carcinoma
|
Case |
Gender |
Age |
Single/multiple focus |
Major diameter (cm) |
Number of lymph node metastasis areas |
Number of metastatic lymph nodes |
Larger lymph node tumor type |
Tumor type |
|
10# |
F |
56 |
S |
1.4 |
2 |
2+/53 |
0.69cm×0.57cm |
Papillary thyroid carcinoma |
|
11# |
F |
29 |
M |
1.7 |
2 |
2+/64 |
0.88cm×0.76cm |
Papillary thyroid carcinoma |
|
12# |
F |
56 |
S |
1.5 |
0 |
0 |
/ |
Papillary thyroid carcinoma |
|
13# |
M |
54 |
S |
2.2 |
1 |
2+/14 |
1.15cm×0.23cm |
Papillary thyroid carcinoma |
|
14# |
F |
56 |
S |
2.5 |
1 |
3+/13 |
1.05cm×0.37cm |
Papillary thyroid carcinoma |
|
15# |
F |
29 |
S |
2.3 |
0 |
0 |
/ |
Papillary thyroid carcinoma |
|
16# |
F |
43 |
S |
1.2 |
0 |
0 |
/ |
Papillary thyroid carcinoma |
|
17# |
M |
39 |
S |
2 |
1 |
1+/118 |
1.50cm×0.45cm |
Papillary thyroid carcinoma |
Note: The low-risk PTC group is defined as follows: no surrounding thyroid tissue invasion, no distant metastasis, <3 regional lymph node metastases, ≤ 5 lymph node metastases, or < 3 cm metastatic lymph nodes. F, female; M, male; S, single; M, multiple
Table 3. Statistical analysis of pathological information of PTC case samples
|
Classification |
Gender F (M) |
Age |
Single multiple foci (number of cases) |
Focus size |
Number of lymph node areas |
Number of lymph nodes |
|
High-risk |
7 (2) |
34.4±4.8 |
4 (5) |
|
≥3 |
>5 |
|
Low-risk |
6 (2) |
45.3±11.9 |
7 (1) |
|
≤2 |
≤5 |
|
P-Value |
p>0.05 |
p<0.05 |
p<0.05 |
p>0.05 |
p<0.05 |
p<0.05 |
|
|
|
* |
* |
|
* |
* |
F, female; M, male
3.2 Ultrasound analysis of cases in the high and low-risk PTC groups
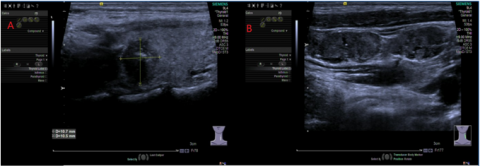
Partial ultrasound images of the large and small PTC transfer are shown in Figures 1 and 2. It can be seen from the figure that the number of regional lymph node metastases in the ultrasound images of the PTC high-risk group was significantly higher than that of the low-risk group.
Figure 1. Ultrasound and pathological examination results of the PTC high-risk group; image A: A hypoechoic nodule with a size of 1.07 cm was detected in the superior thyroid on the left side × 0.88 cm × 1.05 cm, the boundary is unclear, the edge is not smooth, growing in a vertical position, and small dotted strong echo can be seen. Ultrasonic findings: left thyroid nodule (TI-RADS 5); ultrasonographic appearance of image B: there are several hypoechoic areas in the left cervical region III, with unclear demarcations between the cortex and medulla, small bright spots and irregular cystic dark areas can be seen, and some of them are fused with each other. Ultrasound showed the left cervical region III abnormally swollen lymph nodes
The ultrasonographic manifestations of patients in the high-risk and low-risk PTC groups are summarized in Tables 4 and 5. As shown in the table, among the ultrasonic characteristics of thyroid nodules, the number of microcalcifications and lesions are significant indicators of difference, positively correlated with the risk of cancer metastasis. The ultrasonic characteristics of the cervical lymph nodes showed statistical differences in the indicators of cystic change, calcification, cases of lymph node fusion, and whether the lymph node boundary was clear in the high- and low-risk PTC groups. Cystic change, calcification, and lymph node fusion positively correlated with the risk of cancer metastasis. In addition, the clearer the lymph node boundary, the lower the risk of cancer metastasis.
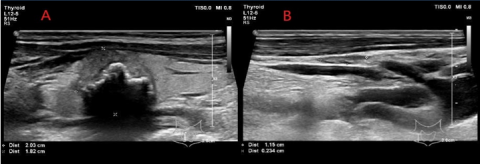
Figure 2. Ultrasound and pathological examination results of the PTC low-risk group; image A: A hypoechoic nodule with a size of 2.03 cm was detected in the middle and upper parts of the right thyroid × 1.95 cm × 1.82 cm; the boundary is unclear, the edge is not smooth, and it grows vertically. It is close to the front and back envelopes, and thick and small strong echoes can be seen inside, with a good shadow behind. Ultrasonic findings: right thyroid nodule (TI-RADS 4C); B-image ultrasound findings: several hypoechoic areas in the right cervical region IV, with a clear boundary between cortex and medulla, and uniform cortical echo. Ultrasound showed that the right cervical region IV lymph nodes were detected
Table 4. Ultrasonic characteristics of thyroid nodules
|
Classification |
Number of internal echoes: Yes (No) |
Boundary: unclear (clear) |
Growth number in an upright position: yes (no) |
Number of microcalcifications: yes (no) |
Number of adjacent capsules: yes (no) |
Number of consolidated bridgeheads: Yes (No) |
Number of single and multiple stoves: single (multiple) |
|
High-risk |
7(2) |
6(2) |
7(1) |
8(1) |
5(4) |
2(7) |
2(6) |
|
Low-risk |
6(2) |
6(2) |
6(2) |
3(5) |
2(6) |
1(7) |
7(1) |
|
P-Value |
F=0.036, p=0.853 |
F=0.000, p=1 |
F=1.577, p=0.230 |
F=7.136, p=0.017<0.05 |
F=2.229, p=0.156 |
F=1.053, p=0.321 |
F=105, p=0.000<0.01 |
|
|
|
|
|
* |
|
|
** |
Table 5. Ultrasonic characteristics of the cervical lymph nodes
|
Classification |
Number of cystic variants: yes (no) |
Cases with calcification: yes (no) |
Number of cases with clear lymphatic hilar structure: yes (no) |
Number of cases of lymph node fusion: yes (no) |
Number of cases with a clear lymph node boundary: yes (no) |
|
High-risk |
6(3) |
5(4) |
1(8) |
4(5) |
5(4) |
|
Low-risk |
0(8) |
0(8) |
6(2) |
0(8) |
8(0) |
|
P-Value |
F=56.471, p=0.000 |
F=564.706, p=0.000 |
F=2.192, p=0.159 |
F=564.706, p=0.000 |
F=564.706, p=0.000 |
|
|
** |
** |
|
** |
** |
Cervical lymph node metastasis of PTC significantly impacts local tumor recurrence and even affects the survival of patients. Generally, PTC is the most common metastasis of the cervical lymph nodes in the central region, followed by the lateral cervical lymph nodes. Some studies have found that 7.7% of patients with PTC have metastatic lesions. Therefore, the selection and scope of lateral neck lymph node dissection have become an important part of the treatment of PTC.
As the most sensitive way to detect thyroid lesions, ultrasound is the most commonly used imaging diagnostic tool for differentiating benign and malignant thyroid nodules [14]. Imaging examination can determine the location, size, and structure of lymph nodes according to dynamic and static images, providing more valuable information for determining lymph nodes; however, there are still a few atypical lymph nodes that are difficult to determine. Based on postoperative pathology as the gold standard, this study categorized PTC into high-risk and low-risk groups, according to the Diagnostic and Treatment Guidelines for Thyroid Cancer (2018) and the ATA Guidelines for Diagnosis and Treatment of Thyroid Diseases (2015). Pathological analysis showed that age, single and multiple foci, lymph node areas, and the number of lymph nodes were significantly correlated with PTC risk grouping. Regarding PTC ultrasound indicators, the number of microcalcifications associated with PTC risk groups was significantly correlated, and the number of single multiple lesions was also significantly correlated. In addition, the ultrasonic characteristics of cervical lymph nodes, the number of cystic changes, calcification cases, lymph node fusion cases, clear lymph node boundaries, and other indicators were significantly correlated with risk.
Presently, many scholars [15-17] believe that microcalcification of lymph nodes has high specificity for thyroid cancer and can be used as the most specific ultrasound indicator for the diagnosis of lymph node metastasis. The results of thyroid nodule ultrasound and neck lymph node ultrasound with microcalcification in the high- and low-risk PTC groups in this study are consistent with those of previous studies, indicating that it can be used as an ultrasound indicator of lymph node metastasis. According to a previous study [18], the sensitivity and accuracy of lymph node metastasis diagnosis can be as high as 97% and 58%, respectively, but the specificity is low (5.8%). In this study, the clear structure of the lymph nodes was not significant in diagnosing lymph node metastasis. However, some scholars [19-21] believe that lymph nodes with cystic changes are precise indicators of cervical lymph node metastasis in PTC. The sensitivity, specificity, positive and negative predictive values, and accuracy were 69%, 96.6%, 90.9%, 83.6%, and 87.4%, respectively. Therefore, when cystic changes occur, lymph node metastasis is highly indicated. This study found that the indicators of cystic changes were very significant, which is consistent with previous studies. In addition, the number of lymph node fusions and the number of clear lymph node boundaries are highly significant, which may provide us with a new indicator for diagnosing lymph node metastasis in thyroid cancer.
In summary, this study is crucial regarding the ultrasound diagnosis of PTC metastasis and provides vital information for surgical treatment to avoid incomplete or unnecessary lymph node dissection. However, this study also has limitations: the number of samples included was too small, and there was no retrospective validation analysis of the prognosis of patients undergoing PTC surgery. Therefore, in the next step, this study will expand the number of samples and verify the prognosis of the key indicators.
This research was supported by Zhejiang Medical and Health Science and Technology Plan Project (Grant No.: 2023RC069).
[1] Lloyd, R.V., Osamura, R.Y., Kloppel, G., Rosai, J. (2017). WHO classification of tumours of endocrine organs. Lyon: International Agency for Research on Cancer (IARC).
[2] Koelsch, B., Theurer, S., Staniszewska, M., Heupel, J., Koch, A., Mergener, S., Walk, F., Fischer, C., Kutritz, A., Schmid, K.W., Kindler-Röhrborn, A. (2020). An animal model further uncovers the role of mutant brafV600E during papillary thyroid cancer development. The American Journal of Pathology, 19(3): 702-710. https://doi.org/10.1016/j.ajpath.2019.11.006
[3] Decaussin-Petrucci, M., Descotes, F., Depaepe, L., Lapras, V., Denier, M. L., Borson-Chazot, F., Lifante, J.C., Lopez, J. (2017). Molecular testing of BRAF, RAS and TERT on thyroid FNAs with indeterminate cytology improves diagnostic accuracy. Cytopathology, 28(6): 482-487. https://doi.org/10.1111/cyt.12493
[4] Jeon, M.J., Chun, S.M., Kim, D., Kwon, H., Jang, E.K., Kim, T.Y., Shong, Y.K., Jang, S.J., Song, D.E., Kim, W.G. (2016). Genomic alterations of anaplastic thyroid carcinoma detected by targeted massive parallel sequencing in a BRAFV600E mutation-prevalent area. Thyroid, 26(5): 683-690. https://doi.org/10.1089/thy.2015.0506
[5] Sykorova, V., Dvorakova, S., Vcelak, J., Vaclavikova, E., Halkova, T., Kodetova, D., Lastuvka, P., Betka, J., Vlcek, P., Reboun, M., Katra, R., Bendlova, B. Bendlova, B. (2015). Search for new genetic biomarkers in poorly differentiated and anaplastic thyroid carcinomas using next generation sequencing. Anticancer Research, 35(4): 2029-2036.
[6] Kunstman, J.W., Juhlin, C.C., Goh, G., Brown, T.C., Stenman, A., Healy, J.M., Rubinstein, J.C., Choi, M., Kiss, N., Nelson-Williams, C., Mane, S., Rimm, D.L., Prasad, M.L., Höög, A., Zedenius, J., Larsson, C., Korah, R., Lifton, R.P., Carling, T. (2015). Characterization of the mutational landscape of anaplastic thyroid cancer via whole-exome sequencing. Human Molecular Genetics, 24(8): 2318-2329. https://doi.org/10.1093/hmg/ddu749
[7] Kumar, S., Burgess, C., Moorthy, R. (2013). The extent of lateral lymph node dissection in differentiated thyroid cancer in the N+ neck. European Archives of Oto-Rhino-Laryngology, 270: 2947-2952. https://doi.org/10.1007/s00405-013-2434-z
[8] Hannallah, J., Rose, J., Guerrero, M.A. (2013). Comprehensive literature review: Recent advances in diagnosing and managing patients with poorly differentiated thyroid carcinoma. International Journal of Endocrinology, Article ID: 317487. https://doi.org/10.1155/2013/317487
[9] Wang, Y., Duan, Y., Zhou, M., Liu, J., Lai, Q., Ye, B., Liu, D., Li, L., Fang, Y., Yue, K., Jing, C., Wu, Y., Wang, X. (2021). The diagnostic value of thyroglobulin in fine-needle aspiration of metastatic lymph nodes in patients with papillary thyroid cancer and its influential factors. Surgical Oncology, 39: 101666. https://doi.org/10.1016/j.suronc.2021.101666
[10] Cracchiolo, J.R., Wong, R.J. (2018). Management of the lateral neck in well differentiated thyroid cancer. European Journal of Surgical Oncology, 44(3): 332-337. https://doi.org/10.1016/j.ejso.2017.06.004
[11] Zhang, X., Ni, T., Zhang, W. (2022). Ultrasonography-guided thermal ablation for cervical lymph node metastasis of recurrent papillary thyroid carcinoma: is it superior to surgical resection? Frontiers in Endocrinology, 13: 907195. https://doi.org/10.3389/fendo.2022.907195
[12] Csco, C.S.O.C.O. (2019). Chinese Society of Clinical Oncology (CSCO) diagnosis and treatment guidelines for colorectal cancer 2018 (English version). Chinese Journal of Cancer Research, 31(1): 117-134. https://doi.org/10.21147/j.issn.1000-9604.2019.01.07
[13] Haugen, B.R., Alexander, E.K., Bible, K.C., Doherty, G.M., Mandel, S.J., Nikiforov, Y.E., Pacini, F., Randolph, G.W., Sawka, A.M., Schlumberger, M., Schuff, K.G., Sherman, S.I., Sosa, J.A., Steward, D.L., Tuttle, R.M., Wartofsky, L. (2016). 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid, 26(1): 1-133. https://doi.org/10.1089/thy.2015.0020
[14] Cornelison, R., Llaneza, D.C., Landen, C.N. (2017). Emerging therapeutics to overcome chemoresistance in epithelial ovarian cancer: A mini-review. International journal of molecular sciences, 18(10): 2171. https://doi.org/10.3390/ijms18102171
[15] Ram, N., Hafeez, S., Qamar, S., Hussain, S.Z., Asghar, A., Anwar, Z., Islam, N. (2015). Diagnostic validity of ultrasonography in thyroid nodules. Journal of Pakistan Medical Association, 65(8): 875-878.
[16] Jeong, S.Y., Kim, Y.S., Kim, K.C. (2017). Predictive factors for central neck lymph node metastasis in patients with papillary thyroid microcarcinoma without suspicious metastasis by preoperative ultrasonography. Journal of Endocrine Surgery, 17(3): 114-121. https://doi.org/10.16956/jes.2017.17.3.114
[17] Wang, N., Xu, Y., Ge, C., Guo, R., Guo, K. (2006). Association of sonographically detected calcification with thyroid carcinoma. Head & Neck, 28(12): 1077-1083. https://doi.org/10.1002/hed.20481
[18] Dragoni, F., Cartoni, C., Pescarmona, E., Chiarotti, F., Puopolo, M., Orsi, E., Pignoloni P, De Gregoris C, Mandelli, F. (1999). The role of high resolution pulsed and color Doppler ultrasound in the differential diagnosis of benign and malignant lymphadenopathy: Results of multivariate analysis. Cancer: Interdisciplinary International Journal of the American Cancer Society, 85(11): 2485-2490. https://doi.org/10.1002/(SICI)1097-0142(19990601)85:11<2485::AID-CNCR26>3.0.CO;2-Y
[19] Kim, D.W., Choo, H.J., Lee, Y.J., Jung, S.J., Eom, J.W., Ha, T.K. (2013). Sonographic features of cervical lymph nodes after thyroidectomy for papillary thyroid carcinoma. Journal of Ultrasound in Medicine, 32(7): 1173-1180. https://doi.org/10.7863/ultra.32.7.1173
[20] Kessler, A., Rappaport, Y., Blank, A., Marmor, S., Weiss, J., Graif, M. (2003). Cystic appearance of cervical lymph nodes is characteristic of metastatic papillary thyroid carcinoma. Journal of Clinical Ultrasound, 31(1): 21-25. https://doi.org/10.1002/jcu.10130
[21] Mišeikytė-Kaubrienė, E., Trakymas, M., Ulys, A. (2008). Cystic lymph node metastasis in papillary thyroid carcinoma. Medicina, 44(6): 455-459 https://doi.org/10.3390/medicina44060059