Fara Randrianarivelo | Adel Badri* | François Gauthier | Bryan Boudreau-Trudel
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Prevention of accidents and occupational diseases plays a major role in the viability of small and medium-sized manufacturing enterprises. However, occupational health and safety conditions in this setting are often precarious compared to large corporations, in which occupational diseases occur eight times less frequently. In a previous study [1], it has been identified, by reviewing the literature, the measures practiced by managers of businesses in this category in the province of Quebec in their efforts to decrease the incidence of occupational diseases. The initial research work reduced these measures to a catalog of elements of management. In the present article, the findings on the application of these elements will be presented, based on a survey of about 400 manufacturing businesses, of which 252 agreed to answer the questionnaire. The present article provides a descriptive statistic from the analysis of the responses. This work allowed to portray the strengths and deficiencies of occupational disease risk management practices in Quebec based on complete and valid responses from 32 small and medium-sized enterprises (SMEs). Overall, this portrayal reflects a serious effort to take up the cause of occupational health and safety in this type of business. It nevertheless reveals room for improvement of the implementation of health and safety risk management systems, and prevention of musculoskeletal diseases and hearing loss, which were found to occur in respectively 63% and 25% of these companies. This work therefore recommends that these diseases be treated as a priority by researchers and expert practitioners of occupational health and safety.
occupational health and safety, prevention, management, occupational diseases, small and medium-sized enterprises (SMEs), manufacturing, Quebec (Canada)
The alarming statistics for occupational health and safety (OHS) in small and medium-sized manufacturing enterprises in Quebec (SMEs) are mentioned in the review of the literature [1], the prelude to the present article. Two findings emerge from these numbers: 1) OHS performance, in terms of occupational diseases and particularly diseases, lags that of large corporations, based on the period of 2007 to 2012 [2], and 2) risk factors are on the rise in SMEs, notably for musculoskeletal diseases and hearing loss [3].
This same literature review retrieved very few analyses of the deficiencies in OHS or the suitability of proposed preventive measures in SMEs. One study does focus on OHS (perception of risk, participation of employees and prevention at the source) in small companies [4], based on a survey of the opinions of managers, employees, and OHS practitioners. Though informative, these observations are difficult to compare, since statistics in the province of Quebec do not differentiate between small and medium-sized enterprises. In addition, the focus of the study was management of workplace accident risk.
Several elements drawn from the literature review indicate that uptake of occupational disease prevention culture is weak in SMEs, based on the rareness of effective activities and the apparent difficulty of implementing OHS management systems and of complying with the monitoring and record-keeping requirements specified in regulations [5-7]. The economic, technical, and human wherewithal necessary for proactive prevention is often limited in the SME setting. It comes almost as no surprise that OHS is not a priority of most managers of these businesses. Deficiencies in work organization (scheduling, subcontracting, temporary work, manager-labor relations, etc.) and inadequacies in the management of occupational risks (risk evaluation methods, risk reduction activities, etc.) are conspicuous.
The overall aim of this research, of which the results are presented in two articles, this being the second, is to identify the elements of occupational disease prevention practiced in SMEs and evaluate the rigor with which they are practiced, and the success thus achieved, at least in terms of changes in attitude. The results related in this article are presented in three steps: 1) the catalog of the relevant elements of management of occupational disease prevention, drawn from article 1 [1], 2) collection of field data, and 3) analysis of the data to reveal inadequacies and propose recommendations to improve occupational disease prevention and therefore the health of workers in Quebec. Following this introduction, the research methodology is described in section 2, the results are summarized in section 3 then discussed along with the limitations of the study in section 4. We present our conclusion in section 5.
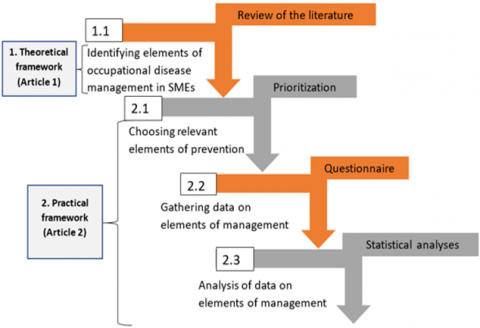
The review of the literature from which we compiled the elements of management practiced in SMEs is described in detail in the first article [1]. The steps of the study (cataloging the elements of management, collecting data in the industrial context of interest, evaluating the practice of OHS, and identifying inadequacies and obstacles) are summarized in Figure 1.
Figure 1. Methodological structure of the study overall (parts 1 and 2)
This study received prior approval from the Université du Québec à Trois-Rivières (UQTR) ethics committee for research involving human subjects (certificate no. CER-18-249-07.6, delivered September 28, 2018, prior to recruitment of SME participants and collection of data). In this study, “elements of management” refer to variables or factors that allow practitioners to influence the effectiveness of occupational disease prevention measures. The “practice” of elements of management refers to how the SME overall applies or complies with these elements.
2.1 Choosing relevant elements of management relevant to the prevention of occupational diseases
Each of the elements of management identified from the literature and considered relevant to the context of SMEs took on an understandable name that complied with OHS legislative and regulatory vocabulary (standard form) and it was explained in detail (general form) to ensure that each of these elements was properly understood by the OHS experts involved in the assessment of their relevance to the SME context. Subsequently, four OHS experts (more than 5 years of experience in OHS) individually assessed the potential influence of each of the elements of management on occupational diseases using a three-level Likert scale (1, 2 or 3). Then, each of these elements was assigned a weighting factor (Pi) obtained by summing the Likert scores of individual assessments, as explained in Table 1. Depending on Pi, the elements of management were ranked in descending order. Finally, all the experts met together to study the results and they unanimously excluded the low weighted elements which were deemed to be definitely not relevant for this research work.
This exercise allowed us to obtain a shorter list of relevant elements and therefore a questionnaire that was more likely to be answered completely. Figure 2 summarizes the process of cataloging the relevant elements of prevention management.
Figure 2. Process for deeming elements of prevention management as relevant or not
2.2 Gathering data on the elements of management
2.2.1 Choice and description of the study sample
Quebec-based manufacturing businesses employing fewer than 450 persons were asked to participate in the study. These numbered about 400 and were located in the Mauricie Centre-du-Québec, Estrie, Montréal, and Abitibi-Témiscamingue regions of the province, which have the highest numbers of manufacturers in the SME category. The directory at the Ministère du Travail, de l’Emploi et de la Solidarité sociale website was used to identify them.
2.2.2 Development of the questionnaire
The questionnaire queried managers on four aspects of their business activity: internal characteristics of the company, applicable OHS legislative and regulatory framework, approach to OHS, and management of occupational disease risk factors. About three quarters of the 86 questions were of the closed type. The respondent was required to check one or more possible answers. In some cases, the respondent was invited to support his choice with an explanation.
The questionnaire was provided in an on-line format and included information on the study and a consent form to which the respondent was directed before answering the questions. The time required to respond completely to the questionnaire was estimated at 45 minutes.
Table 1. Example of calculation of the influence of elements of management on prevention achieved
|
Element of management |
Likert level |
Weighting factor (Pi) calculation |
||
|
1 |
2 |
3 |
||
|
Structural interventions targeting noise (machinery maintenance, ear protectors, etc.) |
1* |
1 |
2 |
P1 = (1x1) + (1x2) + (2x3) = 9 |
|
Procedures targeting dangerous substances |
0 |
1 |
3 |
P2 = (1x2) + (3x3) = 11 |
* Number of experts who voted for this level
Table 2. Calendar of the data collection process
|
Date |
Activity |
Response |
|||
|
Opened the questionnaire |
Began to answer but did not finish |
Completed and returned the questionnaire |
Percent response |
||
|
January 1, 2019 |
Questionnaire sent to 209 participants (177 received, 32 non-deliveries) |
--- |
--- |
--- |
--- |
|
January 15, 2019 |
Questionnaire re-sent to 30 participants (after correction of e-mail address) |
||||
|
January 16, 2019 |
Questionnaire sent to 30 other participants (back from holiday vacations) |
||||
|
January 18, 2019 |
1st tally of answered questionnaires |
90 |
36 |
18 |
7.59 % |
|
January 28, 2019 |
2nd tally of answered questionnaires |
100 |
41 |
18 |
7.59 % |
|
January 31, 2019 |
Reminders sent by e-mail |
--- |
--- |
--- |
--- |
|
February 11, 2019 |
3rd tally of answered questionnaires |
144 |
59 |
22 |
9.28 % |
|
Feb. 18–25, 2019 |
Reminders by phone |
--- |
--- |
--- |
--- |
|
February 25, 2019 |
4th tally of answered questionnaires |
170 |
76 |
23 |
9.70 % |
|
March 4, 2019 |
Questionnaire sent to 15 other businesses |
--- |
--- |
--- |
--- |
|
March 8, 2019 |
5th tally of answered questionnaires |
179 |
80 |
32 |
12.69 % |
|
March 8, 2019 |
Closing of on-line access |
--- |
--- |
--- |
--- |
2.2.3 Validation of the questionnaire
The developed questionnaire was sent to three members of the research team, who answered it as representatives of fictitious SMEs. Any malfunctions of the platform were thus detected, the clarity of the questions was discussed, the database functionality was validated, and the time required to answer the questionnaire was determined more precisely. This process went through several iterations. The resulting researcher version was then tested again by sending it to the same team members, to two participating managers of companies, and to two UQTR graduate students having no connection to the project.
2.2.4 Distribution of the questionnaire
The manufacturing businesses were contacted by phone to present and explain the project. The call was usually directed to the human resources director or the employee responsible for OHS. Many companies did not wish to participate in the project, citing lack of time or interest or some internal restriction. In some cases, confidentiality, or suspicion that we had some connection to the Commission des normes, de l’équité, de la santé et de la sécurité du travail (CNESST), may have been the real issue. However, 237 companies agreed to participate and provided e-mail addresses to receive the questionnaire. The e-mail contained a link for one-click access to the questionnaire.
The follow-up calls and e-mails were necessary to get many of the questionnaires. An additional 44 companies were contacted for participation, of which 15 provided e-mail addresses. In all, 444 businesses were contacted and 252 received the questionnaire. Table 2 summarizes the time course of data collection.
2.3 Analysis of data on elements of management
The 80 answered questionnaires were checked for completeness. The number of incomplete responses was 48. The other 32 were retained for data analysis. The data were downloaded from the web application into a spreadsheet (MS Excel®) and grouped into six sections as follows: 1) company internal characteristics, 2) OHS legislative and regulatory framework, 3) OHS management systems, 4) implementation of OHS, 5) workplace organization, and 6) management of occupational risks.
The measurement of the “Elements of management” is carried out by the control of its presence according to the answer of the company. The element takes the value “1” when it is present or “0” when it is absent.
Descriptive analyses were performed to obtain a frequency distribution table for the application of the elements of occupational disease prevention and the percentage of companies that applied or complied with the element of management.
The distribution of frequencies (or percentage) is calculated by dividing the element of management present in the SME by the total of SMEs having questionnaires retained (32 SMEs, absolute %) or by the total of SMEs having the specific aspect (relative %). Depending on these frequencies, a discussion is carried out to bring out the key information related to each of the six sections mentioned above.
3.1 Profile of the respondents
The respondent profile section of the questionnaire comprised two questions.
Only 28% of the respondents were OHS coordinators. The remaining respondents occupied functions unrelated to OHS: human resources staff (25%), purchasing (9%), upper management (9%), production supervisors (6%), quality control (6%), company founders (6%), one engineer (3%), one technical director (3%) and one industrial manager (3%). About 91% of these 32 respondents indicated that they manage OHS in their company. Table 3 shows the distribution of the respondent profiles.
Table 3. Profiles of the company respondents to the questionnaire
|
Respondent’s function in the company |
Number of respondents |
% |
|
OHS coordinator |
9 |
28 |
|
Human resources management staff (director, head, assistant, etc.) |
8 |
25 |
|
Financial service staff (accountant, purchaser, etc.) |
3 |
9 |
|
Production supervisors |
2 |
6 |
|
Quality supervisors |
2 |
6 |
|
Engineer |
1 |
3 |
|
Technical director |
1 |
3 |
|
Industrial manager |
1 |
3 |
|
Upper managerial staff (CEO, vice-president, etc.) |
3 |
9 |
|
Business owner |
2 |
6 |
3.2 Company internal characteristics
Nine questions concerned the internal characteristics of the company.
About 56% of the businesses contacted had 20 to 99 employees. The rest (44%) were in the category 100 to 499 employees. Many of them (50%) had total annual sales of $15–49 million. In the vast majority (84%) of these, the directors claimed to be committed to OHS. Overall, 84% of the respondents indicated that their company made sure that staff was available to manage OHS properly. About 88% of SMEs claimed to employ a person whose tasks included explicitly the management of OHS. Among managers of these, 25% reported having formal training in OHS. Many of them (43%) indicated that they were spending less than 5 hours per week on OHS-related tasks.
In most of the companies (69%), the respondent estimated at less than 4% of total sales the amount budgeted for OHS. The amount was 10–19% of total sales in 9% of the companies.
The internal characteristics of the companies who returned the completed questionnaire are presented in Table 4.
3.3 Legislative and regulatory framework
The questionnaire contained 22 questions on legislative and regulatory framework applicable to the company. All companies mentioned known OHS standards. The most often cited were OHSAS 18001, CSA Z1006, CSA Z94 and CSA Z432. To monitor compliance with standards, regulations, and laws, 38% of SMEs carried out internal evaluations, 28% turned to external experts, and 34% used both types of evaluation.
Table 4. Internal characteristics of the businesses based on the questionnaire
|
Characteristic |
Range of values |
Number of companies |
% |
|
Size (number of employees) |
20–99 100–499 |
18 14 |
56 44 |
|
Annual sales |
Below $1 million $1–4 million $5–14 million $15–29 million $30–49 million |
0 11 5 7 9 |
0 35 16 22 28 |
|
Proportion of workers with 0–2 years of experience |
0–24% 25–49% 50–75% 75–100% |
16 6 6 4 |
50 19 19 12 |
|
Proportion of workers with 3–5 years of experience |
0–24% 25–49% 50–75% 75–100% |
19 7 5 1 |
59 22 16 3 |
|
Proportion of workers with over 5 years of experience |
0–24% 25–49% 50–75% 75–100% |
8 9 13 2 |
25 28 41 6 |
|
OHS direction |
Commitment to OHS |
27 |
84 |
|
OHS resources (material, technical, economic, human) |
Available |
27 |
84 |
|
Employee whose tasks explicitly include OHS |
Available |
28 |
88 |
|
Time devoted to OHS (hours/week) |
|||
|
0–5 6–10 11–20 21–45 |
12 4 3 9 |
43 14 11 32 |
|
|
Formal training in OHS |
|||
|
Yes No. |
7 21 |
25 75 |
|
|
Percentage of total sales budgeted for OHS |
0–4% 5–9% 10–14% 15–19% |
22 6 1 2 |
69 19 3 6 |
Table 5. Summary of OHS legislative and regulatory frameworks applicable in SMEs
|
Element of management |
Specific aspect |
Number of companies |
% |
|
OHS standards |
Knowledge and implementation |
32 |
100 |
|
Auditing of compliance with OHS standards, regulations, and laws |
Internal evaluation |
12 |
38 |
|
Evaluation by an external expert |
9 |
28 |
|
|
Internal and external |
11 |
34 |
|
|
Training of managers and workers regarding the applicable laws and regulations |
Training offered |
25 |
78 |
|
Health and safety committee |
Committee structure and activities |
29 |
91 |
|
Mandate and functioning |
24 |
83 |
|
|
Support and involvement of directors |
27 |
93 |
|
|
Training of committee members |
24 |
83 |
|
|
Agreement among members |
28 |
97 |
|
|
Availability of the members |
22 |
76 |
|
|
Member leadership |
29 |
100 |
|
|
Prevention program |
Program structure and activities |
25 |
78 |
|
In-house preparation |
13 |
52 |
|
|
Preparation subcontracted |
12 |
48 |
|
|
Identification of risks |
25 |
100 |
|
|
Explaining the details to workers |
21 |
84 |
|
|
Developing, monitoring the plan of action |
21 |
84 |
|
|
Prevention representative |
Presence of a representative |
19 |
59 |
|
On the premises; responsiveness |
15 |
79 |
|
|
OHS experience and knowledge |
10 |
53 |
|
|
Collaboration with health and safety staff |
18 |
95 |
|
|
Collaboration with workers and managers |
15 |
79 |
|
|
Registry of inspections completed |
Content of the inspection registry (exposures) |
31 |
97 |
|
Hazards for which the company was using an inspection form or checklist |
Noise |
20 |
63 |
|
Radiation |
4 |
13 |
|
|
Vibration |
8 |
25 |
|
|
Dangerous substances |
19 |
59 |
|
|
Poor ergonomics |
19 |
59 |
|
|
No inspection form or checklist |
6 |
19 |
About 78% of the respondents indicated that managers and workers were trained in the laws and regulations applicable to their situation. A health and safety committee had been created in 91% of the companies. Among respondents, 93% indicated that company directors supported and were involved in the committee.
Nearly 78% of the companies had a prevention program in place, prepared in-house in 52% of these cases, otherwise by external experts.
A prevention representative was present in the company, according to 59% of respondents. In over half of these companies (53%), this meant a single representative. In companies with at least one representative, this person was present on the premises and responsive to requests, according to 79% of respondents.
Almost all companies (97%) kept a registry of inspections carried out. Nearly 19% apparently were not using inspection forms or checklists for possible hazards. The legislative and regulatory frameworks applicable according to the respondents are summarized in Table 5.
3.4 OHS management systems
Eight questions covered aspects of in-house OHS management in the companies.
About 34% of the respondents claimed to apply an OHS management system. Only 9% of these SMEs indicated that they were compliant with OHSAS standard 18001 versus 27% with ISO 45001. None of these companies claimed to be compliant with CSA Z1000.
Nearly 50% of the companies were applying a risk management process or structured procedures and claimed to have the means available for such management. OHS risks were analyzed in 81% of the companies, 38% periodically. Structured inquiries took place after the declaration of an occupational disease in 59% of the companies and 53% kept a registry of occupational diseases declared. The diseases or diseases mentioned were distributed as follows:
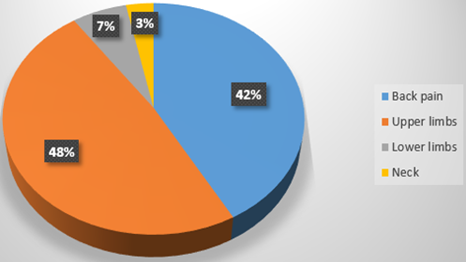
●63% were musculoskeletal diseases, of which 65% concerned the back, 75% upper limbs, 10% lower limbs and 5% neck.
●25% were hearing problems.
●16% were respiratory problems.
●3% were skin conditions, neoplasms, tumors, or cancers.
●34% were for unspecified diseases.
About 75% of the respondents indicated that health professionals were consulted when health problems arose in the workplace. Figure 3 shows the details of the musculoskeletal diseases mentioned to have occurred.
The responses to the questions concerning OHS management systems are summarized in Table 6.
Figure 3. Nature of the musculoskeletal problems that had occurred in the SMEs that responded to the survey
Table 6. OHS management systems in the companies that responded to the survey
|
Element of management |
Specific aspect |
Number of companies |
% |
|
OHS management system |
Compliance with a management system |
11 |
34 |
|
OHSAS 18001 CSA Z1000 ISO 45001 Other |
1 0 3 7 |
9 0 27 64 |
|
|
Risk management process or structured procedure and availability of means for such management |
Management process or procedure is applied |
16 |
50 |
|
Analyses of OHS risks |
OHS risk analyses conducted |
26 |
81 |
|
Periodically Other moments When processes are changed, etc. In conjunction with in-house rearrangement When a new process or equipment is introduced |
10 5 16 15 17 |
38 19 62 58 65 |
|
|
Consideration and structured integration of OHS in company activities (purchasing, design, production, etc.) |
OHS is considered and integrated in a structured manner |
20 |
63 |
|
Structured inquiry into declared occupational diseases or diseases |
Inquiry is conducted |
19 |
59 |
|
Registry of occupational diseases or diseases that have occurred |
Registry is kept |
17 |
53 |
|
Cases of occupational diseases or diseases |
|||
|
0 1–5 110 1,750 Other responses: confidential, not followed up, not determined |
2 7 1 1 6 |
12 41 6 6 35 |
|
|
Health professional involvement in work-related health problem cases |
Health professional is consulted |
24 |
75 |
Table 7. Means used to promote OHS culture in SMEs
|
Element of management |
Specific aspect |
Number of companies |
% |
|
Managers |
|||
|
Knowledge of OHS |
Company possesses knowledge |
28 |
88 |
|
OHS leadership |
|
4 |
13 |
|
Skill in involving workers in OHS problem solving |
Skills possessed or claimed |
26 |
81 |
|
Awareness of the OHS needs of the workers |
Means used: |
|
|
|
Suggestions (ideas and alerts) box Informal interviews Periodical meetings Other |
6 23 20 7 |
19 72 63 22 |
|
|
Incitation of workers to comply with preventive measures |
Means of persuasion |
|
|
|
Reward Reprimand Awareness-raising meetings Other |
4 17 27 4 |
13 53 84 13 |
|
|
Workers |
|||
|
Knowledge of OHS |
Prevalence of knowledge |
24 |
75 |
|
Involvement in OHS |
|
26 |
81 |
|
Wherewithal to alert to OHS problems and declare diseases |
Possess means or culture of alerting and declaring |
32 |
100 |
|
Wherewithal to assert OHS rights (refusal to expose oneself, preventive time off, etc.) |
Awareness of rights |
32 |
100 |
|
OHS training provided by the company |
Upon hiring About standards Other than prescribed by law On the job Time and content adapted Post-training evaluation Knowledge, skills, and aptitudes of instructors |
26 24 12 24 26 16 14 |
81 75 38 75 81 50 44 |
|
Other OHS implementation actions |
|||
|
OHS auditing, inspection, and monitoring programs |
Programs are in place and maintained |
25 |
78 |
|
Systematic inspection of collective protective equipment |
Inspections are carried out regularly |
27 |
84 |
|
Choice and systematic monitoring of personal protective equipment |
Choice is available followed up |
26 |
81 |
|
Systematic inspection of hygiene conditions in the shared spaces |
Inspections carried out |
26 |
81 |
|
Systematic monitoring of working conditions quality (air, moisture, temperature, etc.) |
Monitoring is maintained |
23 |
72 |
|
Systematic medical examinations |
Examinations are carried out |
13 |
41 |
Table 8. Means used to manage risks of developing occupational diseases or diseases
|
Element of management |
Specific aspect |
Number of companies |
% |
|
Management of chemical risks |
|||
|
Dangerous substances and materials |
Risk of exposure |
22 |
69 |
|
Risk management procedures or program |
Use of procedures or program |
19 |
86 |
|
Training, information, and awareness-raising |
Offered or not |
19 |
86 |
|
Use of documents (product labels and safety data sheets) |
Presence of documents |
19 |
86 |
|
Management of physical risks |
|||
|
Noise |
Risk of exposure |
28 |
88 |
|
Measurement, systematic evaluation of sources of noise |
Measurement, evaluation carried out |
22 |
79 |
|
Systematic intervention (machinery maintenance, replacement, noise reduction and absorption, protective equipment, procedures, training, etc.) |
Intervention carried out |
21 |
75 |
|
Radiation |
Risk of exposure |
7 |
22 |
|
Measurement, systematic evaluation of sources of radiation |
Measurement, evaluation carried out |
5 |
71 |
|
Systematic intervention (maintenance, replacement, reduction, and absorption of radiation, use of protective equipment, procedures, training, etc.) |
Intervention carried out |
5 |
71 |
|
Vibrations |
Risk of exposure |
10 |
31 |
|
Measurement, systematic evaluation of sources of vibration |
Measurement, evaluation carried out |
5 |
50 |
|
Systematic intervention (machinery maintenance, replacement, vibration reduction and absorption, protective equipment, procedures, training, etc.) |
Intervention carried out |
7 |
70 |
|
Thermic constraints |
Risk of exposure |
13 |
41 |
|
Measurement, systematic evaluation of thermic constraints |
Measurement, evaluation carried out |
9 |
69 |
|
Systematic intervention (machinery maintenance, replacement, reduction and absorption of heat losses, protective equipment, procedures, training, etc.) |
Intervention carried out |
12 |
92 |
|
Management of ergonomic risks |
|||
|
Ergonomic risks |
Risk of exposure |
26 |
81 |
|
Measurement, systematic evaluation of ergonomic risks |
Measurement, evaluation carried out |
14 |
54 |
|
Control of all risks |
|||
|
All personal protective equipment required |
Use of personal protective equipment |
28 |
88 |
|
Adequate structures for managing the use of personal protective equipment (choice, training, monitoring of use, maintenance and replacement, etc.) |
Presence of structures |
27 |
84 |
3.5 Promotion of OHS culture
How OHS culture was promoted in the companies was the subject of 26 questions. Most of the respondents (88%) indicated that their managers had adequate knowledge of OHS. Only 13% indicated that the company managers assumed a leadership role regarding OHS, whereas 81% claimed that at least one manager was skilled in involving workers in the solving of OHS problems. To maintain awareness of worker OHS needs, 19% of managers were using an idea (complaints or suggestions) box, 72% conducted informal interviews with workers, 63% conducted periodical meetings, and 13% cited other means, including:
●Deviations forms
●A “toolbox” meeting at the beginning of the shift
A majority of managers (84%) conducted awareness-raising meetings to encourage workers to respect OHS guidelines. About 75% of respondents indicated that their workers possessed knowledge of OHS (laws, regulations, hazards, procedures, rules, etc.), and 81% indicated worker involvement in OHS. About 81% of SMEs were offering in-house OHS training and 75% were offering structured training in compliance with the minimal standards prescribed by the applicable laws and regulations. Formal medical examinations (pre-hiring, periodic, unannounced, upon return to the job, etc.) were practiced systematically according to 41% of the respondents. How OHS culture was being promoted in SMEs is summarized in Table 7.
3.6 Management of risks of developing occupational diseases or diseases
The management of the risks of developing occupational diseases was the subject of 24 questions.
About 69% of the respondents indicated that the risk of exposure to dangerous materials existed in their company. In the cases of exposure, 86% had a hazardous material handling procedure or program in place, 86% provided training activities, awareness-raising, and information sessions on dangerous materials and 86% had the documents necessary for proper management of these materials (product labeling and safety data sheets).
Most of the respondents (88%) emphasized that some of their activities carried a high risk of exposure to noise. Among these, 69% were measuring noise levels and conducting systematic evaluation of noise sources and 66% appeared to put sufficient effort into reducing the risks associated with noise.
Nearly 22% of the respondents indicated that some of their activities carried a risk of exposure to radiation. 71% of these companies were measuring radiation levels and conducting systematic evaluation of radiation sources and intervening to reduce levels at the source.
Most of the respondents (80%) indicated that some of their activities carried risks related to poor ergonomics. A few examples of the situations mentioned are:
●Working in a standing position with heavy parts
●Stationary work on machinery
Only 54% of the SMEs concerned by ergonomic risks were conducting measurements and systematic evaluation and intervening systematically to reduce these risks. A few examples of interventions are:
●An ergonomics expert observes, recommends job rotation
●Training sessions with ergonomists
●Use of OHS software (trained preventionist)
Finally, 88% of the SMEs were using all required personal protective equipment and 84% possessed adequate structures for managing the use of this equipment. The means by which the risk of occupational diseases or diseases were being managed are summarized in Table 8.
The results of the survey are discussed here in view of those of the literature review that guided the formulation of the questionnaire [1].
4.1 Internal characteristics of the business
About 75% of the SMEs from which completed questionnaires were received were dealing with at least one of the main occupational diseases or diseases declared in Quebec: musculoskeletal problems, hearing loss, respiratory disease, skin conditions, cancer, tumors, and neoplasms. Among these businesses, 58% were small companies and 42% were medium-sized.
Musculoskeletal diseases were the most prevalent, affecting 42% of small companies and 33% of medium-sized companies, which was consistent with the previously noted relationship between company size and prevalence of occupational diseases more generally [8-10] and of musculoskeletal risk factors in particular [11].
Most of the OHS managers of the SMEs consulted were employed mainly in other capacities. This likely explains why many of them devoted less than five hours per week to OHS management. Among the comments provided to justify the absence of a position devoted to OHS management, we note in particular:
●“We don’t have the financial means to afford a full-time position.”
●“The directors do not see the importance of investing in human resources devoted to OHS.”
●“One person working part-time is sufficient, given the size of the company.”
In addition, most of these companies were spending less than 5% of their total annual sales on OHS. The most of any of them spent was 19% for one year, in one case. The effect of budget and staff constraints on OHS-related expenditure in SMEs has been noted previously [12-17].
4.2 OHS legislative and regulatory framework
In most SMEs, the frequency of the various regulatory OHS auditing or evaluation activities was once per year. One respondent also mentioned that “the prevention mutual conducts an audit each year, but even if we are found non-compliant, the directors do not invest in compliance”. This low frequency of OHS audits in SMEs has been noted previously [4, 15, 18, 19]. Some authors even describe the directors of these businesses as negligent [20, 21].
Whereas all medium-sized companies have a health and safety committee, not all small companies do. In these cases, the respondents mentioned some of the reasons for the absence of a committee:
●“Young company”
●“Lack of trained staff”
The effect of company size on the inclusion of a health and safety committee has been noted previously [4].
Only 36% of the SMEs were conducting OHS meetings once or twice a month whereas 39% of small companies were having these meetings at least every other month. The frequency of health and safety committee meetings has a considerable impact on OHS performance [22]. At least once a month is recommended for companies with more than 100 employees and at least once every two months for those with 25 to 100 employees.
Some of the respondents mentioned constraints on the development and application of a prevention program. These were expressed for example as follows:
●“Difficult to achieve realistically. Small workshops with many customized manual tasks.”
●“The CEO does not like being structured and does not want to spend time on this.”
This difficulty of developing and applying a prevention program in SMEs has been noted previously [4].
4.3 OHS management systems
The comments provided by the respondents reveal that some SMEs do devote resources to setting up an OHS management system. Two examples are:
●“Before, there was no system of OHS management in my two companies. Having worked for 12 years with OHSAS 18001, I have been applying these methods daily. I have been on this job for a year, and I can say that our system is now structured, and even though it does not meet the standard, it will in three years!”
●“In the process of implementation: development of the manufacturing diagram and the operations schematic for risk analysis at each step and piece of equipment involved in the manufacture of our products.”
The difficulty of implementing an OHS management system in SMEs has been emphasized in previous studies [6, 23].
The most common diseases of concern in the SMEs studied in detail were musculoskeletal, followed by hearing problems. Both have been noted previously as preponderant, although hearing problems were found to be the more widespread of the two in at least one study [2]. The most common musculoskeletal problems were chronic back pain or spinal disc damage and then upper limb injury. This too has been noted previously in a study by the Quebec Ministry of Health, published in 2018 [24].
4.4 Promotion of OHS culture
Most of the respondents claimed to have sufficient knowledge of OHS for the purposes of their company. This is in contrast with the findings of studies of managers in this type of company over the years [14, 25, 26]. In addition, all respondents mentioned at least some of the tools and means used by the managers to keep informed about worker needs regarding OHS. At least one study has found that managers of SMEs frequently pay too little attention to workers wellbeing [15].
Most of the respondents indicated that workers were adequately involved in promoting OHS. However, getting workers involved in prevention has previously been found difficult to achieve [4]. In addition, all respondents claimed that their workers were free to assert all their OHS rights. However, workers often do not have the possibility of defending their right to refuse to expose themselves to hazards.
Almost all the structured training offered in the SMEs in accordance with minimal standards set forth in OHS law and regulations was focused only on machinery safety (forklifts and other stock handling vehicles and equipment, lockout/tagout). This confirms deficiencies in OHS training noted previously in the case of SMEs [27].
Most of the SMEs consulted were conducting regular tests or in-house inspections of the workplace security. This practice has been found to be less frequent in businesses of this size [7].
4.5 Management of risks of developing occupational diseases or diseases
Among the SMEs whose respondent indicated the presence of dangerous materials on their premises and a risk of exposure thereto, 59% were in the small business category. The greater exposure to chemical risks in small businesses has been discussed previously [20, 28]. In addition, only 50% of these SMEs mentioned Workplace Hazardous Materials Information System (WHMIS) training and management. The low level of hazardous materials management in SMEs has been emphasized in at least one previous study [29].
Most of the respondents confirmed the risk of exposure to noise on their premises, a risk found heightened in SMEs in a previous study [30]. In most cases, noise risk reduction measures amounted to using personal protective equipment. Turning to such equipment rather than administrative and technical measures in the SMEs context has been discussed previously [29, 31]. Among the mentioned measurements and evaluations of risks associated with noise are the following:
●“Calculation of exposure to noise throughout the factory (production and stock areas)”
●“Noise measurement and audiometric”
●“Sound intensity measurement”
Not very long ago, noise measurement and control were not always practiced or considered important in the SMEs setting.
Among the SMEs where exposure to vibrations was acknowledged, 70% were small businesses. The greater exposure to vibrations in the employ of smaller companies has been discussed in relatively recent articles [3, 32].
Only half of the respondents indicated that their enterprises conducted ergonomic analyses and interventions. Studies over the years have concluded that most interventions in this realm are too expensive and fastidious for businesses of this size [32].
Most of the SMEs apparently possessed adequate structures for providing and monitoring the use of personal protective equipment. Among the examples mentioned by the respondents are:
●“Periodic replacement of safety boots and glasses, use and wear monitored by supervisors”
●“Chosen according to the hazard and risk level, considering work reality and worker preference”
●“Use and maintenance supervised and managed, chosen by the health and safety committee, training by supervisors, replaced as needed”
However, the use of personal protective equipment has been found wanting in the SMEs setting [33-35].
4.6 Limitations and future work
Among the several limitations of the present study, the choice of elements of management of occupational disease and disease prevention and the perceived effectiveness of these elements were based entirely on the OHS expert’s opinions were involved in the planning of the research. The subjectivity of these opinions obviously cannot be ruled out. In addition, the sample of businesses and their regions (Mauricie, Centre-du-Québec, Estrie, Montréal and Abitibi-Témiscamingue) limited the possibility of generalizing our findings, even to the management of occupational disease prevention practices in SMEs in the Quebec manufacturing sector overall.
Also, even though the questionnaire consisted mostly of closed-type questions, the time allotted to the online completion (about 45 min) remained problematic. Some respondents still found it too long.
The analysis took into consideration the opinions of the respondents, whose participation was voluntary, and no measurement of the exactness or the representativeness of these results was possible. To begin with, no respondent was expected to view their company’s methods and performance with total objectivity. Moreover, results obtained from voluntary participants probably had a bias towards pre-existing awareness of the importance of preventing occupational diseases and therefore were not representative of opinion in SMEs in Quebec overall.
The following considerations can partially remedy the gaps of the use of questionnaires: the working process as indicated in the methodology is sufficiently rigorous (section 2); this process is also certified by the ethics committee for research (section 2); the drafting of the questionnaire was based on questions with a common and simple language and it was tested and validated to avoid all forms of confusion (sections 2.2.2 and 2.2.3); the choice of the most competent respondents was made after our discussions to recruit the SMEs (section 2.2.4); the acceptance of the questionnaires is based on well-established quality criteria (section 2.3). Finally, the work shows a correspondence of the data of this research with those of previous research and government statistics (section 4). This correspondence can show credibility in all the work done.
The results of this study could nevertheless inform the planning of applied research focused on OHS in small and medium-sized manufacturing enterprises. For example, it could guide the design of a decision-aid tool better adapted to protecting workers exposed to myriad hazards in the complex and dynamic SME setting. At this stage, we are still searching for a way of bringing corporate deciders and the legislator to the same table to improve the text of legislation and define more clearly certain concepts pertaining to effective management of OHS in the SME context.
The aim of this research project was to study the practice of managing occupational disease and disease prevention in manufacturing enterprises in the small to medium-sized category in Quebec. A review of the literature [1] allowed us to identify about a hundred elements of management of occupational illness and disease prevention. After ranking these, 86 were deemed particularly pertinent and therefore integrated into our analysis of OHS practices in manufacturing SMEs in Quebec.
The results of our survey lead us to conclude that musculoskeletal problems and hearing loss continue to affect workers in many of the SMEs consulted, respectively 63% and 25%. This study thus confirms the previously observed association between company size (small to medium sized) and heightened risk of developing an occupational disease or disease. It also appears that a lack of financial and human resources continues to have a direct impact (constraining) on OHS management in SMEs like those consulted.
The descriptive statistics provide a preliminary portrayal of the practice of managing the prevention of occupational diseases in 32 small or medium-sized manufacturing enterprises in Quebec. Notwithstanding the limitations of this study, we were able to identify some of the strengths and weaknesses in these practices. We find that SMEs overall do strive to promote OHS culture. However, the management of occupational risks in general could be improved. We recommend that these businesses, as well as OHS experts and researchers, pay particular attention to musculoskeletal problems, hearing loss, and implementation of OHS management systems.
[1] Randrianarivelo, R., Badri, A., Gauthier, F., Boudreau-Trudel, B. (2022) Prevention of occupational diseases in small and medium-sized manufacturing enterprises in Quebec (Canada): Part 1 – portrayal of elements influencing OHS performance.
[2] Duguay, P., Boucher, A., Busque, M.A. (2014). Statistiques sur les maladies professionnelles au Québec. In Colloque IRSST–Maladie Professionnelles: Portrait, défis et Perspectives.
[3] Champoux, D., Prud’homme, P. (2017) Analyse comparative du contexte de travail et portrait statistique des problèmes de santé et sécurité au travail en fonction de la taille des entreprises (R-986) IRSST Consulted May 4, 2021: https://www.irsst.qc.ca/media/documents/PubIRSST/.
[4] Champoux, D., Brun, J.P. (2010). Dispositions, capacités et pratiques de SST dans les petites entreprises: Opinions de patrons, d’employés et d’intervenants en SST au Québec. Perspectives interdisciplinaires sur le travail et la santé, (12-2).
[5] Lescure, E., Nadeau, S., Morency, F. (2015) SME et SST : Quand la résilience est un modèle d’affaires. [Version électronique]. 50e Congrès international de la société d’Ergonomie de Langue Française. Paris: Société d’Ergonomie de Langue Française.
[6] Organisation internationale du travail. (2011). Système de gestion en SST: Un outil pour une amélioration continue. Journée mondiale de la sécurité et de la santé au travail.
[7] Eakin, J.M., Champoux, D., MacEachen, E. (2010). Health and safety in small workplaces: refocusing upstream. Canadian Journal of Public Health, 101(1): S29-S33. https://doi.org/10.1007/BF03403843
[8] Cunningham, T.R., Sinclair, R. (2015) Application of a model for delivering occupational safety and health to smaller businesses: Case studies from the US. Safety Science, 71: 213-225. https://doi.org/10.1016/j.ssci.2014.06.011
[9] Targoutzidis, A., Koukoulaki, T., Schmitz-Felten, E., et al. (2014). The Business Case for Safety and Health at Work: Cost-Benefit Analyses of Interventions in Small and Medium–Sized Enterprises–Study. Publications Office of the European Union, Luxembourg: https://publications. Europa. eu/en/publication-detail/-/publication/8e9e23ea-2270–4d51–8553–94152e503afd, access on 20 June 2019.
[10] Micheli, G.J., Cagno, E. (2010). Dealing with SMEs as a whole in OHS issues: Warnings from empirical evidence. Safety Science, 48(6): 729-733. https://doi.org/10.1016/j.ssci.2010.02.010
[11] Morse, T., Dillon, C., Weber, J., Warren, N., Bruneau, H., Fu, R. (2004). Prevalence and reporting of occupational illness by company size: Population trends and regulatory implications. American Journal of Industrial Medicine, 45(4): 361-370. https://doi.org/10.1002/ajim.10354
[12] Holizki, T., McDonald, R., Gagnon, F. (2015). Patterns of underlying causes of work-related traumatic fatalities–comparison between small and larger companies in British Columbia. Safety Science, 71: 197-204. https://doi.org/10.1016/j.ssci.2014.06.008
[13] Cagno, E., Micheli, G.J., Perotti, S. (2011). Identification of OHS-related factors and interactions among those and OHS performance in SMEs. Safety Science, 49(2): 216-225. https://doi.org/10.1016/j.ssci.2010.08.002
[14] Hasle, P., Limborg, H.J. (2006). A review of the literature on preventive occupational health and safety activities in small enterprises. Industrial Health, 44(1): 6-12. https://doi.org/10.2486/indhealth.44.6
[15] Vickers, I., James, P., Smallbone, D., Baldock, R. (2005). Understanding small firm responses to regulation: The case of workplace health and safety. Policy Studies, 26(2): 149-169. https://doi.org/10.1080/01442870500127626
[16] Champoux, D., Brun, J.P. (1999) Prise en charge de la sécurité dans les petites entreprises des secteurs de l’habillement et de la fabrication de produits en métal. Institut de recherche en santé et en sécurité du travail du Québec, 1-26.
[17] Dionne-Proulx, J., Beauchamp, Y., Carrière, J.B. (2003). ISO 9000 et après impact sur la performance en SST dans l'entreprise manufacturière (Vol. 327). Institut de recherche Robert-Sauvé en santé et en sécurité du travail.
[18] Mendeloff, J.M., Nelson, C., Ko, K., Haviland, A. (2006). Small businesses and workplace fatality risk: an exploratory analysis (Vol. 371). Rand Corporation.
[19] Mendeloff, J., Gray, W.B. (2005). Inside the black box: How do OSHA inspections lead to reductions in workplace injuries? Law & Policy, 27(2): 219-237. https://doi.org/10.1111/j.1467-9930.2005.00198.x
[20] MacEachen, E., Kosny, A., Scott-Dixon, K., et al. (2010). Workplace health understandings and processes in small businesses: A systematic review of the qualitative literature. Journal of Occupational Rehabilitation, 20(2): 180-198. https://doi.org/10.1007/s10926-009-9227-7
[21] Martin, C., Guarnieri, F. (2008) Position du problème. Pratiques de prévention des risques professionnels dans les SME-PMI. in Technique & Documentation-Lavoisier. Paris: Lavoisier. Consulted June 18, 2021: https://www.researchgate.net/publication/278767241_Pratiques_de_prevention_des_risques_professionnels_dans_les_SME-PMI.
[22] Desmarais, L. (2009) Le comité de SST — Un rouage essentiel. Prévention au Travail, (22): 8-14.
[23] Vinel, M. (2011) Le système de management par étapes appliqué à une SME (M.Sc.A. inédit., Conservatoire national des arts et métiers. Institut d’Hygiène Industrielle et de l’Environnement, Paris, France) Consulted July 18, 2021: https://dumas.ccsd.cnrs.fr/dumas-00608615/document.
[24] Ministère de la santé et des services sociaux du Québec (2018) Troubles musculosquelettiques liés au travail. Ministère de la santé et des services sociaux du Québec (2018). Consulted July 18, 2021: http://www.msss.gouv.qc.ca/professionnels/statistiques-donnees-sante-bien- etre/statistiques-de-sante-et-de-bien-etre-selon-le-sexe-volet-national/troubles-musculosquelettiques-lies-au-travail/.
[25] Masi, D., Cagno, E., Micheli, G.J. (2014). Developing, implementing and evaluating OSH interventions in SMEs: a pilot, exploratory study. International Journal of Occupational Safety and Ergonomics, 20(3): 385-405. https://doi.org/10.1080/10803548.2014.11077059
[26] Champoux, D., Brun, J.P. (2003). Occupational health and safety management in small size enterprises: An overview of the situation and avenues for intervention and research. Safety Science, 41(4): 301-318. https://doi.org/10.1016/S0925-7535(02)00043-7
[27] Arocena, P., Núñez, I. (2010). An empirical analysis of the effectiveness of occupational health and safety management systems in SMEs. International Small Business Journal, 28(4): 398-419. https://doi.org/10.1177%2F0266242610363521
[28] Sørensen, O.H., Hasle, P., Bach, E. (2007). Working in small enterprises–is there a special risk? Safety Science, 45(10): 1044-1059. https://doi.org/10.1016/j.ssci.2006.09.005
[29] Laird, I., Olsen, K., Harris, L. A., Legg, S., Perry, M.J. (2011). Utilising the characteristics of small enterprises to assist in managing hazardous substances in the workplace. International Journal of Workplace Health Management, 4(2): 140-163. https://doi.org/10.1108/17538351111143312
[30] Singh, L.P., Bhardwaj, A., Deepak, K.K. (2010). Occupational exposure in small and medium scale industry with specific reference to heat and noise. Noise and Health, 12(46): 37-48.
[31] Suter, A.H. (2012). Engineering controls for occupational noise exposure. Sound Vib, 46: 24-31.
[32] Gervais, M. (2006). Conditions de travail, de santé et de sécurité des travailleurs du Québec. Canadian Policy Collection.
[33] Toulouse, G. (2005). Étude de faisabilité en vue d'intégrer la santé et la sécurité du travail et l'ergonomie à l'approche PVA-Kaitzen. desLibris.
[34] Arcury, T.A., Grzywacz, J.G., Anderson, A.M., et al. (2013). Employer, use of personal protective equipment, and work safety climate: Latino poultry processing workers. American Journal of Industrial Medicine, 56(2): 180-188. https://doi.org/10.1002/ajim.22101
[35] Floyde, A., Lawson, G., Shalloe, S., Eastgate, R., D’Cruz, M. (2013). The design and implementation of knowledge management systems and e-learning for improved occupational health and safety in small to medium sized enterprises. Safety Science, 60: 69-76. https://doi.org/10.1016/j.ssci.2013.06.012